Page 2 of 8
AS1.1-4 | Evolution, Scope, Ethics and Career Pathways in Anaesthesiology — SDL Guide (Part 2)
Ethical Principles in Anaesthesiology: Consent, Autonomy, and Accountability
Ethics in Anaesthesiology occupies a distinctive position because the anaesthetic encounter uniquely compromises the patient's capacity for autonomous decision-making. When a patient is anaesthetised, they are rendered unconscious, unable to communicate, and entirely dependent on the anaesthesiologist's judgment. This power asymmetry places ethical obligations on the anaesthesiologist that are more immediate and more consequential than in most other specialties. AS1.3 requires you to enumerate and describe the ethical principles as they relate specifically to anaesthesiology practice, drawing on the classical Beauchamp and Childress framework that you have encountered in your ethics and communication curricula.
The four foundational principles — autonomy, beneficence, non-maleficence, and justice — are universally applicable in medicine but each has a specific instantiation in anaesthetic practice that you must understand.
Autonomy and Informed Consent for Anaesthesia
Autonomy is the patient's right to make informed decisions about their own care. In anaesthesia this is operationalised as informed consent — a process, not merely a signed form. The anaesthesiologist must explain the proposed anaesthetic technique in comprehensible language, disclose material risks (awareness under anaesthesia, post-operative nausea and vomiting, dental injury, nerve injury, drug allergy, aspiration pneumonitis), present reasonable alternatives (e.g., regional vs general anaesthesia), and ascertain that the patient genuinely understands and freely consents. Consent for anaesthesia is separate from consent for surgery — this point is frequently misunderstood by students and even by surgeons. A patient may consent to surgery but refuse the proposed anaesthetic technique; the anaesthesiologist must respect this and negotiate alternatives.
Special consent situations in anaesthesia include:
- Paediatric patients — consent from the legal guardian; assent from the child when developmentally appropriate
- Emergency situations — implied consent applies when the patient cannot consent and delay would cause harm; the principle of acting in the patient's best interests governs
- Jehovah's Witness patients — adult patients with capacity may refuse blood transfusion even if refusal risks death; the anaesthesiologist must document the refusal, explore bloodless alternatives, and not override the patient's decision
- Mental health comorbidity — capacity assessment is required; the Mental Healthcare Act 2017 governs treatment of patients with mental illness in India
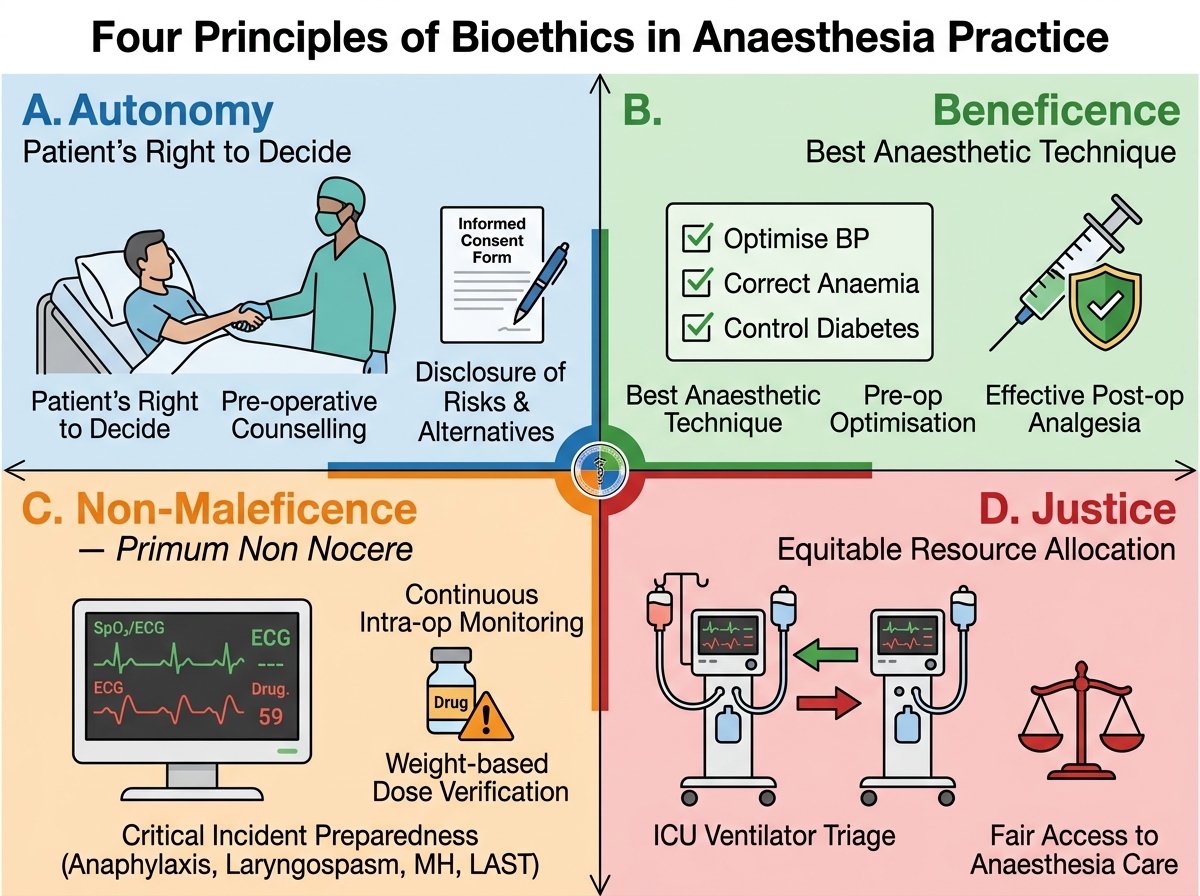
The Four Principles of Bioethics Applied to Anaesthesia Practice
Beneficence
Beneficence — acting in the patient's best interest — is expressed in anaesthesia through the obligation to select the safest and most effective anaesthetic technique for that patient's specific condition, to optimise the patient pre-operatively (manage hypertension, optimise diabetes, correct anaemia), and to provide the best possible post-operative analgesia to enable recovery. It is not merely the absence of harm; it is the active promotion of the patient's well-being.
Non-Maleficence
Non-maleficence — first, do no harm (primum non nocere) — has particular force in anaesthesia because every anaesthetic agent is a potentially lethal drug at the wrong dose. This principle is operationalised through:
- Rigorous pre-operative risk assessment
- Adherence to drug dosing guidelines (never exceeding maximum safe doses; verifying weight-based calculations)
- Maintaining continuous monitoring throughout the anaesthetic
- Preparing for and managing critical incidents (anaphylaxis, laryngospasm, malignant hyperthermia, local anaesthetic systemic toxicity)
Justice
Justice in anaesthesia encompasses equitable access and fair resource allocation. In the ICU context, the anaesthesiologist may need to triage scarce ventilators, ICU beds, or blood products among competing patients — a process governed by objective medical need rather than social worth, ability to pay, or personal relationships. Justice also demands that anaesthetic care of the same quality be provided to all patients regardless of socioeconomic status, gender, caste, religion, or language.
Additional Ethical Issues Specific to Anaesthesiology:
- Awareness under anaesthesia — the anaesthesiologist has an ethical obligation to disclose intra-operative awareness when it occurs, even when distressing to report; suppression of this information violates veracity (truthfulness)
- End-of-life care and withdrawal of life support — intensive care anaesthesiologists frequently lead decisions to withdraw ventilatory support in futile illness; these decisions require clear documentation, multidisciplinary consensus, and family communication following the principles of beneficence and non-maleficence
- Professional boundaries with pharmaceutical industry — the anaesthesiologist must maintain independence from commercial influences when selecting drugs and equipment
- Confidentiality — medical information obtained during anaesthetic assessment is confidential and must be protected per established medical ethics principles
Career Prospects in Anaesthesiology: Pathways, Subspecialties, and Opportunities
Anaesthesiology is among the most versatile specialties for postgraduate career planning in Indian medicine, offering a wide spectrum of roles from purely clinical through academic, administrative, and research-oriented tracks. AS1.4 asks you to describe the prospects of the specialty — a competency with direct personal relevance as you approach MBBS completion and preparation for the NEET-PG examination. Understanding these pathways enables an informed career decision and also helps you understand why your anaesthetic colleagues are highly trained, rigorously examined professionals worthy of collegial respect.
In India, postgraduate training in Anaesthesiology is among the most sought-after streams in the NEET-PG allocation process, reflecting both the breadth of clinical opportunity and the competitive remuneration the specialty commands across public and private sectors. The training transforms the MBBS graduate into a fully-rounded specialist capable of independent practice across surgical anaesthesia, critical care, and pain medicine — a scope that very few other specialties can match. The MBBS graduate takes the NEET-PG examination and seeks admission to either an MD or a DNB programme, both of which are now recognised equivalently for superspeciality entrance and service eligibility. In India, the postgraduate pathway to specialist practice in Anaesthesiology follows a structured route and leads to the two main postgraduate qualifications:
- MD Anaesthesiology — a three-year university-based postgraduate degree
- DNB Anaesthesiology — awarded by the National Board of Examinations (NBE); increasingly equivalent in recognition to MD and recognised for superspeciality admission
Both tracks include structured clinical training across the full scope of the specialty: general anaesthesia, regional anaesthesia, obstetric anaesthesia, paediatric anaesthesia, cardiac and thoracic anaesthesia, neuroanesthesia, and critical care. Most programmes require a minimum of twelve months of ICU posting.
Subspecialty career paths available to the anaesthesiologist:
- Cardiac Anaesthesia — high-acuity work supporting open-heart surgery, valve replacements, bypass procedures, and cardiac transplantation; requires fellowship training (often 1–2 years post-MD/DNB) and competence with transoesophageal echocardiography
- Neuro-anaesthesia — management of neurosurgical patients including awake craniotomies (for functional brain mapping), spinal surgeries, and patients with raised intracranial pressure; requires mastery of cerebral physiology and pharmacology
- Paediatric Anaesthesia — significantly different physiology from adults (higher oxygen consumption per kg, narrow safety margins, hypothermia risk); centres of excellence have dedicated paediatric anaesthesia fellowships
- Pain Medicine — both acute post-surgical pain management and chronic pain conditions; interventional pain fellowship training provides competence in procedures (epidurals, nerve blocks, neuromodulation)
- Obstetric Anaesthesia — high volume, high stakes, round-the-clock service; requires expertise in epidural/spinal techniques and obstetric emergencies
- Critical Care Medicine — many anaesthesiologists pursue joint training or fellowship in critical care; this is the most common single subspecialty destination in India
- Regional Anaesthesia and Acute Pain — ultrasound-guided peripheral nerve blocks have transformed post-surgical recovery; fellowship training in this field is increasingly available
- Academic and Research — university departments offer teaching, examination, curriculum development, and clinical research roles; ICMR-funded and industry-sponsored research in anaesthesia pharmacology and patient safety is growing
The Indian Society of Anaesthesiologists (ISA) and the Society of Anaesthesiologists of the Karnataka Region (SAKR) (among many regional societies) organise continuing professional development, fellowship examinations, and international collaborations. The World Federation of Societies of Anaesthesiologists (WFSA) coordinates global standards for training and patient safety.
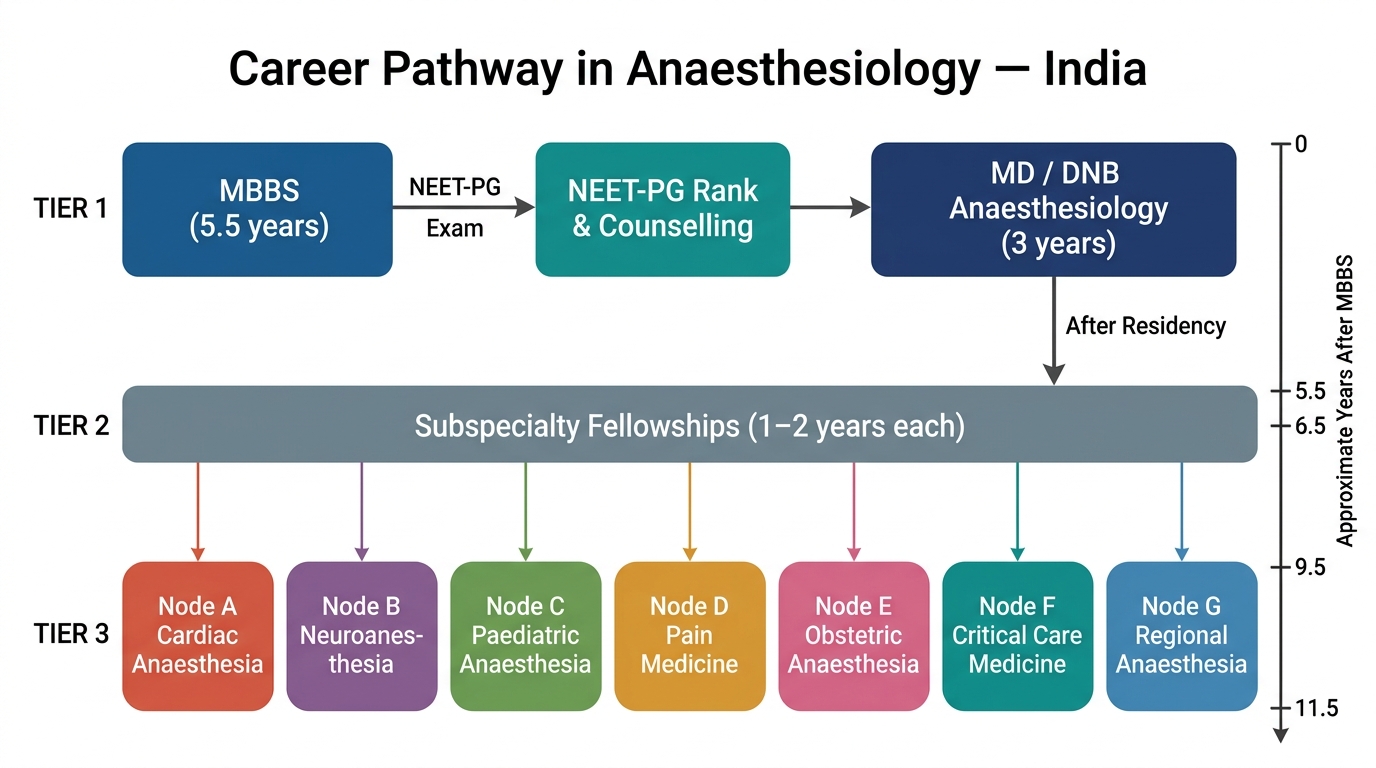
Career Pathway in Anaesthesiology (India): MBBS to Subspecialty Fellowships
Career prospects in anaesthesiology are robust because:
- Surgical volume in India is growing rapidly with expanding health insurance coverage (Ayushman Bharat PM-JAY)
- There is a documented shortage of trained anaesthesiologists in tier-II and tier-III cities, creating both public and private sector opportunities
- The specialty commands competitive remuneration in both government service and private practice
- International opportunities (USMLE/PLAB for USA/UK; Gulf and Southeast Asia demand trained anaesthesiologists) are available for those seeking migration
- The specialty offers the satisfaction of measurable patient impact — a correctly managed anaesthetic and a safely managed post-operative period have immediate, visible consequences for patient welfare
Self-Assessment: Consolidating Your Understanding of Anaesthesiology as a Specialty
Having worked through the evolution, roles, ethical framework, and career prospects of Anaesthesiology, this self-assessment section invites you to actively test and consolidate your understanding before moving to the formative quiz questions that follow. Self-assessment is not passive recall — it is a deliberate retrieval exercise that strengthens long-term retention through the testing effect (Roediger & Karpicke, 2006), which is one of the most robustly replicated findings in educational psychology. Work through the prompts below before reading the answer framework provided, and be honest with yourself about gaps — those gaps are precisely where further study is most productive.
Below are structured self-assessment prompts mapped to the four NMC competencies (AS1.1–AS1.4) covered in this SDL. After each prompt, a brief framework for the expected answer is provided. Use these to identify your own knowledge gaps:
Prompt 1 (AS1.1 — Evolution): Without looking back, name three key milestones in the history of Anaesthesiology, including the year and its significance.
Expected framework: 1846 (ether — first public demonstration, Morton/Warren, MGH; World Anaesthesia Day); 1942 (curare — muscle relaxation, anaesthetic triad formalised); 1980s (pulse oximetry/capnography — mortality drops from ~1 in 5,000 to ~1 in 100,000). Candidates scoring 2/3 should review the Evolution section.
Prompt 2 (AS1.2 — Roles): A surgical team asks why the anaesthesiologist needs to conduct an independent pre-operative assessment rather than relying on the surgeon's clerking. Formulate a three-sentence response.
Expected framework: The response should mention: (a) the anaesthesiologist's independent duty of care, (b) specific anaesthetic concerns (airway, aspiration risk, haemodynamic stability, drug interactions, fasting status) not captured in the surgical assessment, and (c) that consent for anaesthesia is separate from surgical consent.
Prompt 3 (AS1.3 — Ethics): A competent adult patient, after full disclosure of risks, refuses spinal anaesthesia for her hip surgery and requests general anaesthesia instead, despite the anaesthesiologist's clinical preference for regional technique. What should the anaesthesiologist do, and which ethical principle governs this decision?
Expected framework: The governing principle is autonomy. The anaesthesiologist must respect the patient's competently-made decision, document the refusal and the discussion, and proceed with general anaesthesia if it is clinically feasible and safe. The anaesthesiologist's personal preference does not override the patient's autonomous choice.
Prompt 4 (AS1.4 — Career): Compare MD Anaesthesiology and DNB Anaesthesiology in terms of awarding body, duration, and current equivalence in India.
Expected framework: MD = university-awarded, 3 years, traditional route. DNB = awarded by National Board of Examinations (NBE), 3 years, now equivalent to MD for superspeciality admission and service eligibility following regulatory harmonisation. Both require NEET-PG for entry.
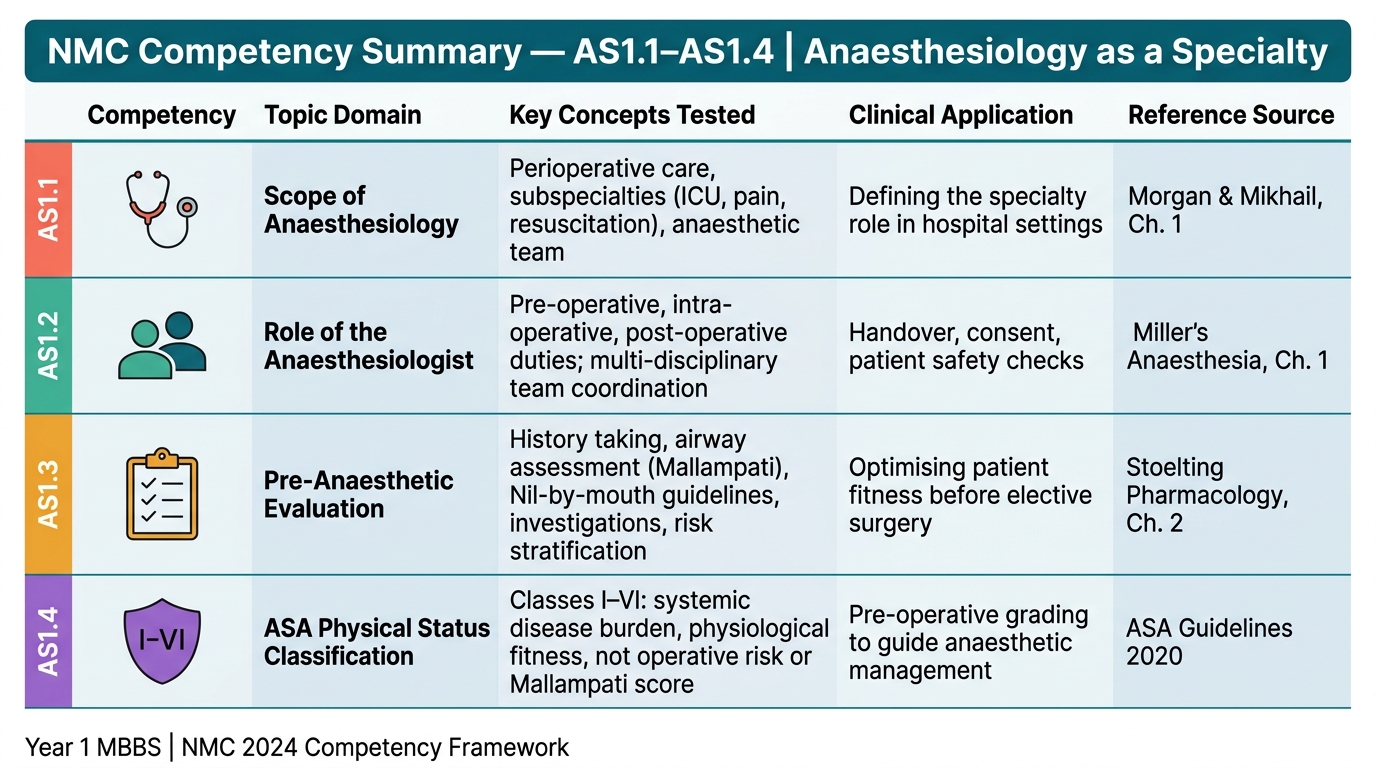
NMC Competency Map: AS1.1–AS1.4 | Anaesthesiology as a Specialty
SELF-CHECK
The ASA Physical Status Classification System (I–VI) is used by anaesthesiologists to grade which of the following?
A. A. The degree of operative technical difficulty anticipated
B. B. The patient's systemic disease burden and physiological fitness
C. C. The predicted risk of postoperative complications
D. D. The Mallampati oropharyngeal view for airway assessment
Reveal Answer
Answer: B. B. The patient's systemic disease burden and physiological fitness
The ASA Physical Status Classification grades the patient's systemic disease burden — I = healthy, II = mild disease, III = severe disease, IV = life-threatening disease, V = not expected to survive without surgery, VI = brain-dead organ donor. It is NOT a measure of operative risk or technical difficulty, and it is NOT the Mallampati score (which grades oropharyngeal view for airway prediction — a completely separate scale). A common error is conflating ASA with Mallampati or using ASA as a direct proxy for peri-operative mortality risk, which it was not designed to estimate precisely.
SELF-CHECK
During adult Basic Life Support (BLS), in which of the following rhythms is immediate defibrillation the correct intervention?
A. A. Asystole
B. B. Pulseless Electrical Activity (PEA)
C. C. Ventricular Fibrillation (VF)
D. D. Sinus bradycardia with pulse
Reveal Answer
Answer: C. C. Ventricular Fibrillation (VF)
Defibrillation is indicated ONLY for shockable rhythms — Ventricular Fibrillation (VF) and pulseless Ventricular Tachycardia (pVT). Asystole and PEA are non-shockable; delivering a shock to these rhythms wastes time and provides no benefit. Sinus bradycardia with a detectable pulse does not constitute cardiac arrest. The distinction between shockable and non-shockable rhythms is critical during resuscitation and is a core competency within the AS curriculum.
CLINICAL PEARL
Consent for anaesthesia is legally and ethically separate from consent for surgery. A patient who signs the surgical consent form has NOT thereby consented to a specific anaesthetic technique. The anaesthesiologist must independently explain the proposed anaesthetic plan, its alternatives, and its material risks (including awareness, aspiration, dental injury, allergy, and nerve damage). If a patient refuses one anaesthetic approach — for example, a Jehovah's Witness who refuses general anaesthesia with the possibility of blood transfusion — the anaesthesiologist must explore alternatives (regional anaesthesia, bloodless surgical techniques) rather than override the patient's competently stated preference. Documenting this conversation is as important as the conversation itself: an undocumented consent process is legally equivalent to no consent process.