Page 2 of 11
AS10.1-2 | Positioning Hazards and Perioperative Hazard Prevention — SDL Guide (Part 2)
Management Strategies and the WHO Surgical Safety Checklist
Prevention of perioperative hazards requires a combination of engineering safeguards, standardised checklists, equipment protocols, and a deeply embedded culture of psychological safety in which all members of the operating-theatre team feel genuinely empowered to raise concerns without any fear of hierarchical reprisal. No single intervention is more evidence-based for preventing multiple categories of simultaneous harm than the WHO Surgical Safety Checklist, introduced in 2009 following the Safe Surgery Saves Lives initiative, and now demonstrably associated with a 36% reduction in major complications and a 47% reduction in mortality across eight diverse hospital settings.
The WHO Surgical Safety Checklist has three pause points, each with a designated team leader (typically the anaesthesiologist for Sign-In and Sign-Out, the surgeon for Time-Out, though institutions vary):
- Sign-In (before anaesthesia induction): confirms patient identity, procedure, site, and consent; confirms allergy status; assesses airway risk and aspiration risk; confirms equipment checks (anaesthesia machine, circuit, suction, drugs); arranges pulse oximetry.
- Time-Out (before skin incision): surgeon, anaesthesiologist, and nurse all confirm patient, procedure, and site aloud; surgeon states anticipated critical steps, expected blood loss, and duration; anaesthesiologist states patient-specific concerns; nurse confirms instrument and sponge counts, sterilisation confirmation.
- Sign-Out (before patient leaves the theatre): instrument, sponge, and needle counts confirmed complete; specimens labelled; equipment problems noted for follow-up; surgeon, anaesthesiologist, and nurse confirm key post-operative concerns.
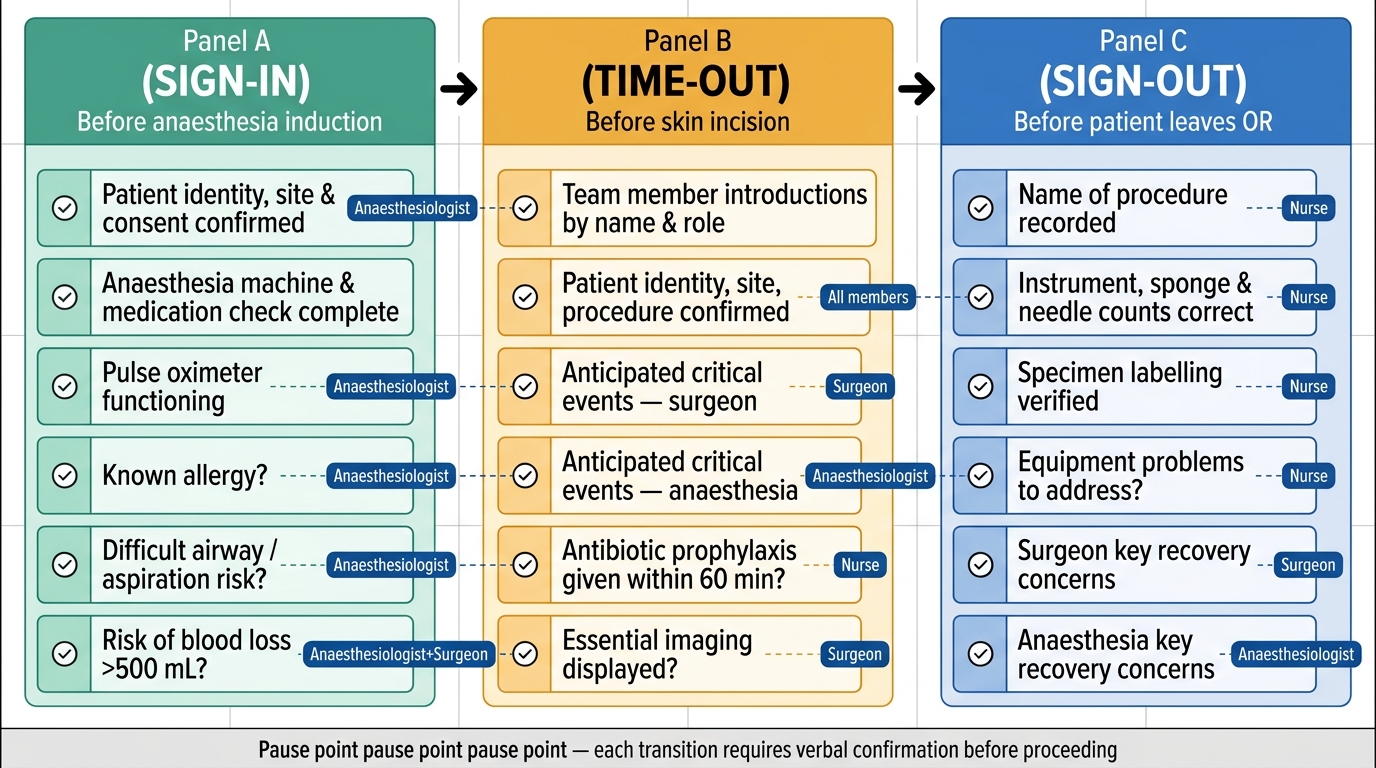
WHO Surgical Safety Checklist: Three Pause Points and Team Responsibilities
Positioning management in practice: the positioning protocol should be executed by at least two people. All bony prominences are padded with foam or gel pads before the drapes go up. The eyes are taped closed and covered. The arms are either tucked with the palms facing inward (supine) or placed on padded arm-boards no more than 90° of abduction. In the lateral position, an axillary roll (not under the axilla but at the rib-cage just caudal to the axilla) prevents compression of the neurovascular bundle. In the lithotomy position, the legs are raised and lowered simultaneously to prevent lumbar torsion, and the calf stirrups are padded. In the prone position, chest rolls support the thorax and the abdomen hangs free, and all facial pressure points are checked after final positioning. Time of position change is documented.
Pressure injury prevention strategies include: the use of pressure-redistributing mattresses (viscoelastic foam or gel) as the primary surface for all cases anticipated to exceed two hours; a team-executed pre-closure position check to confirm no unexpected contact pressure; and a handover note to the recovery nurse specifying any positional vulnerability (e.g., the patient was lateral for 3 hours — inspect the dependent ear, shoulder, and hip).
Thermoregulation management: forced-air warming blanket applied to all accessible body surfaces (upper body for lower-limb surgery, lower body for upper-limb and head-neck surgery); IV fluid warmer for infusions >500 mL; ambient theatre temperature raised to 21–23°C for major paediatric or burn cases; continuous core-temperature monitoring (oesophageal probe, or nasopharyngeal in ENT/oral surgery) with documentation every 15 minutes.
Thromboprophylaxis: sequential compression devices (SCDs) applied before induction to both calves and activated throughout the operation; LMWH timing as per surgical and anaesthetic plan; adequate hydration to avoid haemoconcentration; early physiotherapy mobilisation in the recovery room.
Haemostasis and blood conservation: point-of-care coagulation monitoring (TEG/ROTEM) in anticipated major haemorrhage; tranexamic acid (TXA) administered early (within 3 hours of major haemorrhage or traumatic injury) per CRASH-2 evidence; autologous blood salvage (cell saver) for elective major orthopaedic and vascular surgery; pre-operative optimisation of haemoglobin (iron supplementation, ESA where appropriate); adherence to the patient blood management (PBM) framework which targets restrictive transfusion triggers (Hb transfusion threshold 7–8 g/dL in most elective surgical patients without cardiac disease) to avoid transfusion-associated hazards (TRALI, TACO, transfusion-transmitted infection, immunomodulation).
Preventing specific position-related injuries:
- Brachial plexus: abduction ≤90°, no anterior shoulder stretch, axillary roll correctly placed in lateral decubitus
- Ulnar nerve: elbow padded, neutral forearm rotation, no direct pressure on medial epicondyle
- Common peroneal nerve: padded lateral knee supports in lithotomy, avoid stirrup contact at fibular head
- Eyes: taping closed, moisture chamber or ointment for prolonged cases, avoid any direct orbital pressure, inspect at each position change
- Compartment syndrome prevention: limit lithotomy duration, avoid excessively elevated legs, monitor for postoperative calf pain, tightness, and neurological deficit
SELF-CHECK
A 45-year-old woman is placed in the lithotomy position for a 3-hour gynaecological laparoscopy. Postoperatively she reports inability to dorsiflex her right foot. Which nerve was most likely compressed during positioning?
A. Femoral nerve at the inguinal ligament
B. Common peroneal nerve at the fibular head
C. Sciatic nerve at the greater sciatic notch
D. Sural nerve at the lateral malleolus
Reveal Answer
Answer: B. Common peroneal nerve at the fibular head
The common peroneal nerve is the most frequently injured peripheral nerve in the lithotomy position. It wraps around the fibular head just below and lateral to the knee — precisely where poorly padded stirrups apply sustained lateral pressure. The deficit is foot drop (inability to dorsiflex + evert the foot) with loss of sensation over the dorsum of the foot. The femoral nerve produces quadriceps weakness and loss of knee extension (not foot drop), and it is at risk in extreme hip flexion/external rotation, a less common injury. The sciatic nerve injury would produce combined common peroneal + tibial deficit (global foot and ankle weakness). Prevention: pad the lateral knee support in stirrups; avoid direct contact between the stirrup and the fibular head.
Self-Assessment: Applying the Hazard Framework
Consolidating your understanding of positioning hazards and perioperative risk prevention requires moving from recognition to application — the ability to examine a patient, identify their specific risks, match those risks to preventive strategies, and communicate the plan effectively to the whole operating-theatre team. This self-assessment section poses structured clinical scenarios to test that applied level of reasoning. As a final-year medical student about to enter postgraduate training, you will encounter these situations early in your career, and the mental frameworks you build today will directly influence the safety of patients you care for in your first year of practice.
Scenario A: A 70-year-old man with type 2 diabetes mellitus and peripheral vascular disease is scheduled for a 5-hour posterior lumbar decompression in the prone position. List four specific positioning hazards he faces and the mitigation strategy for each.
Model answer:
1. Eye pressure → CRAO/PION: Use a padded horseshoe headrest; verify no direct orbital contact; inspect eyes after positioning and at intervals; document intraocular check.
2. Pressure injury (heels, anterior iliac spine, sternum): Gel or foam pads under bony prominences; pressure-redistributing mattress; document pad placement.
3. Peripheral nerve injury (ulnar, brachial plexus): Elbow pads; arms tucked with palms inward or on arm-boards ≤90° abduction; check axilla and elbow accessibility after positioning.
4. DVT/PE: He is high-risk (age, vascular disease, prolonged immobility) — SCDs before induction, LMWH postoperatively (timing per surgeon); early mobilisation.
Scenario B: The theatre nurse points out that a patient due for emergency laparotomy has not had a WHO Surgical Safety Checklist performed because the surgical registrar says there is "no time." What is the correct response and what are the minimum elements that must be confirmed in an emergency?
Model answer: The WHO Surgical Safety Checklist is not optional in an emergency — a streamlined version must be completed. At minimum: patient identity and site/procedure confirmation; known allergy status; critical anaesthetic concerns (airway, aspiration risk, current medications); surgeon's anticipated critical steps and blood-loss estimate; equipment check (suction, IV access, blood available). The Sign-Out must still occur to confirm specimen labelling and instrument counts. Leadership assertiveness and closed-loop communication are the tools.
Key take-away principles for the final exam:
- Position-related injuries are often multi-factorial: stretch + compression + duration + pre-existing vulnerability.
- The WHO Surgical Safety Checklist targets multiple hazard categories simultaneously (identity, allergy, airway, blood loss, equipment) and its three pause points have distinct team responsibilities.
- Nerve injuries are the most litigated positioning complication; ulnar nerve and brachial plexus are the two most common sites.
- Postoperative blindness from orbital pressure or ischaemic optic neuropathy, while rare, is catastrophic — prevention requires active intraoperative vigilance, not just pre-positioning setup.
- Temperature management is not a comfort measure — hypothermia causes coagulopathy, infection risk, and arrhythmia.
- ASA I–VI grades systemic disease; Mallampati I–IV grades the oropharyngeal view — do NOT conflate these two classification systems.
CLINICAL PEARL
The three most preventable position-related injuries share a single root cause: they are caused by well-intentioned haste. The brachial plexus is stretched when the team rushes arm positioning without checking abduction angle. The eye is compressed when the prone headrest is not inspected after final draping. The common peroneal nerve is compressed when the stirrups are not padded because the operation is already starting. Build a personal habit: after every position change, before any draping, perform a 60-second checklist — eyes protected, no direct pressure on bony prominences, arms in safe position, axillary roll in correct place, all team members satisfied. This habit costs one minute and prevents a lifetime of harm to the patient.