Page 5 of 17
AS11.3-4 | Basic Airway Opening and Airway Adjunct Insertion — SDL Guide
CLINICAL SCENARIO
A 55-year-old man collapses in the recovery room five minutes after extubation. He is unconscious, and his breathing is noisy and laboured — the classic snoring sound of partial upper airway obstruction. The nurse calls for help. You arrive and have thirty seconds before he becomes apnoeic. There is no intubation equipment ready. Your hands and two simple manoeuvres are your only tools. You perform a head-tilt chin-lift: the snoring stops and the chest begins to rise symmetrically. Thirty seconds later, with the airway maintained, you insert a Guedel oropharyngeal airway — the jaw relaxes, the tongue lifts off the posterior pharyngeal wall, and the patient's SpO₂ climbs from 83% to 97%. This is the reality of basic airway management: high stakes, simple tools, immediate reward.
WHY THIS MATTERS
Basic airway management skills — the manual manoeuvres that open the airway and the adjuncts that maintain it — are among the very few clinical skills that every doctor, regardless of specialty, must be able to perform competently without assistance or specialist equipment. Airway obstruction is the fastest route to brain death: complete obstruction causes loss of consciousness within 3–5 minutes and irreversible anoxic brain injury within 4–6 minutes. In the pre-hospital setting, in the emergency department, in the recovery room, and on the ward, the physician who arrives first must be able to open the airway and maintain it long enough for definitive help. The NMC 2024 competency framework (AS11.3 and AS11.4) requires students to observe and demonstrate these techniques in a simulated environment — this module prepares you for that encounter and for the real patients who will follow.
RECALL
Activate your knowledge of upper airway anatomy from Year-1 Anatomy. The upper airway consists of the nasal passages, the oral cavity, the oropharynx, the nasopharynx, and the laryngopharynx (hypopharynx). The tongue is the most common cause of upper airway obstruction in the unconscious patient — as muscle tone is lost, the tongue falls posteriorly against the pharyngeal wall. The epiglottis, a leaf-shaped cartilage at the base of the tongue, can also contribute to obstruction by falling over the laryngeal inlet. The hyoid bone, to which the tongue base is attached, is important in understanding why chin lift opens the airway. Also recall the anatomy of the nasopharynx — the soft tissue channel running from the nares to the nasopharynx — relevant to nasopharyngeal airway placement. Finally, recall the gag reflex (cranial nerves IX and X): its presence indicates that a patient has protective airway reflexes and may not tolerate an oropharyngeal airway without stimulating vomiting.
Indications for Basic Airway Manoeuvres
Basic airway opening manoeuvres are indicated whenever a patient has inadequate spontaneous airway patency that is not caused by a foreign body or structural lesion requiring definitive intervention. The most common clinical presentations requiring immediate basic airway management include: the unconscious or deeply sedated patient (post-anaesthesia, opioid or benzodiazepine overdose, head injury, post-ictal state, metabolic encephalopathy); the patient with obstructive sleep apnoea in whom sedation or the supine position causes complete pharyngeal collapse; and the patient in cardiac arrest prior to advanced airway placement. In all these scenarios, loss of muscle tone — particularly of the tongue, soft palate, and pharyngeal constrictors — allows the tongue base to contact the posterior pharyngeal wall, producing partial or complete obstruction. The clinical signs of upper airway obstruction are snoring or gurgling with spontaneous breathing (partial obstruction), paradoxical chest-and-abdomen movement, use of accessory muscles, and — in complete obstruction — silence, absent chest wall movement, and progressive desaturation. The first response to any of these signs is a basic airway manoeuvre, not a call for the difficult airway trolley.
Airway adjuncts (oropharyngeal and nasopharyngeal airways) are indicated when manual manoeuvres alone cannot maintain airway patency, when the clinician's hands are needed for other tasks (bag-valve-mask ventilation), or when prolonged airway maintenance is required without advanced airway placement. The choice of adjunct — oral versus nasal — depends on the patient's level of consciousness and the presence or absence of intact laryngeal reflexes.
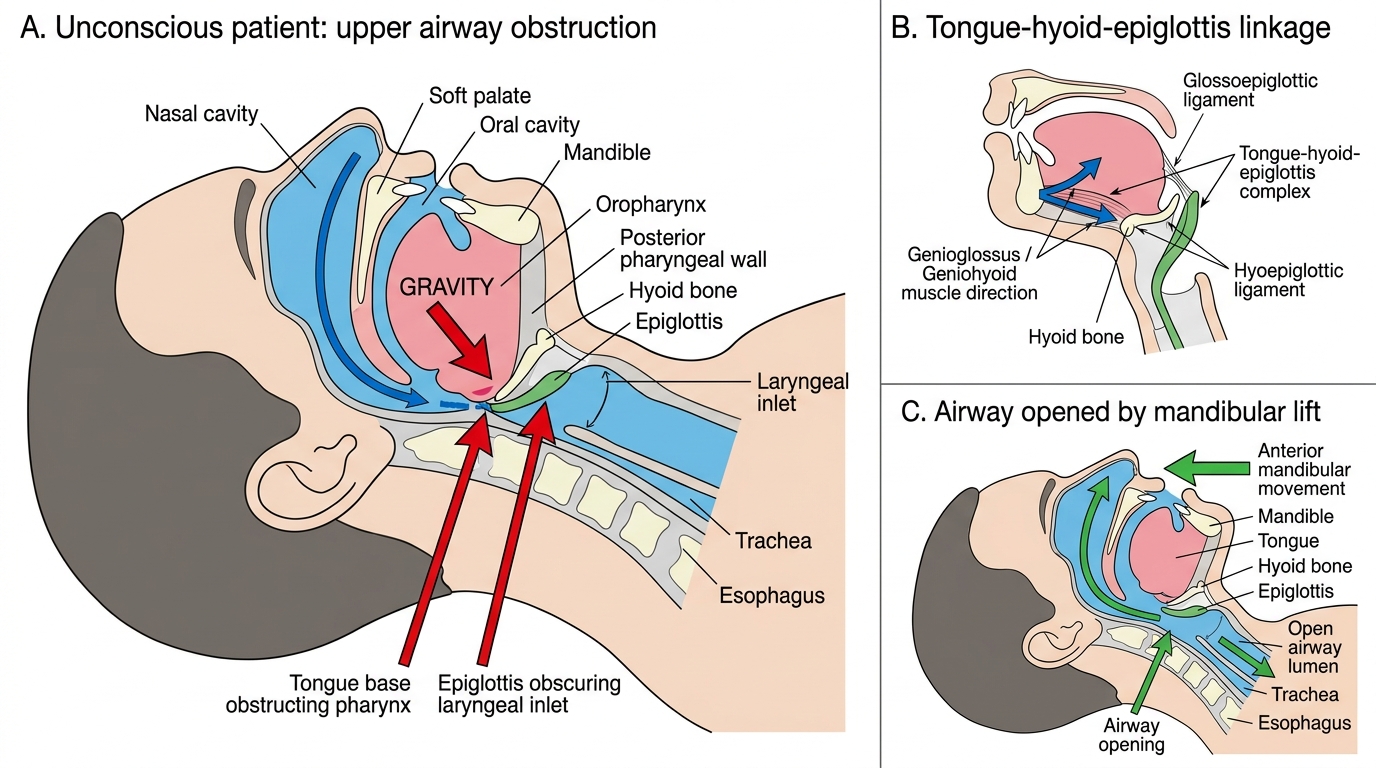
Mechanism of Upper Airway Obstruction in an Unconscious Patient
Anatomy of the Upper Airway Relevant to Airway Opening
A precise understanding of the relevant anatomy makes each basic airway manoeuvre logical rather than mechanical. The tongue is a large muscular organ attached at its base to the hyoid bone and the mandible (via the genioglossus and geniohyoid muscles). In the unconscious patient, these muscles lose tone, and the tongue falls posteriorly under gravity to rest against the posterior pharyngeal wall. Because the tongue is tethered to the mandible, any manoeuvre that moves the mandible anteriorly — chin lift or jaw thrust — necessarily lifts the tongue away from the pharynx and opens the airway.
The hyoid bone is a U-shaped bone in the anterior neck at the level of C3, suspended by muscles from the mandible above and the thyroid cartilage below. It acts as a mechanical fulcrum: anterior displacement of the mandible tensions the floor of the mouth and lifts the hyoid-tongue-epiglottis complex, creating a clear airway channel from the nares to the glottis.
The epiglottis is attached to the base of the tongue by the glossoepiglottic ligament and to the hyoid bone by the hyoepiglottic ligament. When the tongue base falls back, the epiglottis also falls over the laryngeal inlet (the triangular opening between the arytenoids and the posterior aspect of the epiglottis). Anterior tongue traction lifts the epiglottis simultaneously with the tongue, clearing the laryngeal inlet.
The nasopharyngeal airway passes from the nare through the nasal passage, around the posterior pharyngeal wall, and its tip rests in the hypopharynx behind the tongue. Its anatomical pathway traverses the inferior nasal turbinate, the choanae (posterior nasal aperture), and terminates just above the epiglottis. This explains its effectiveness in maintaining an airway without breaching the laryngeal reflex, and why it is preferred over the oropharyngeal airway in patients with preserved consciousness or incomplete anaesthesia.
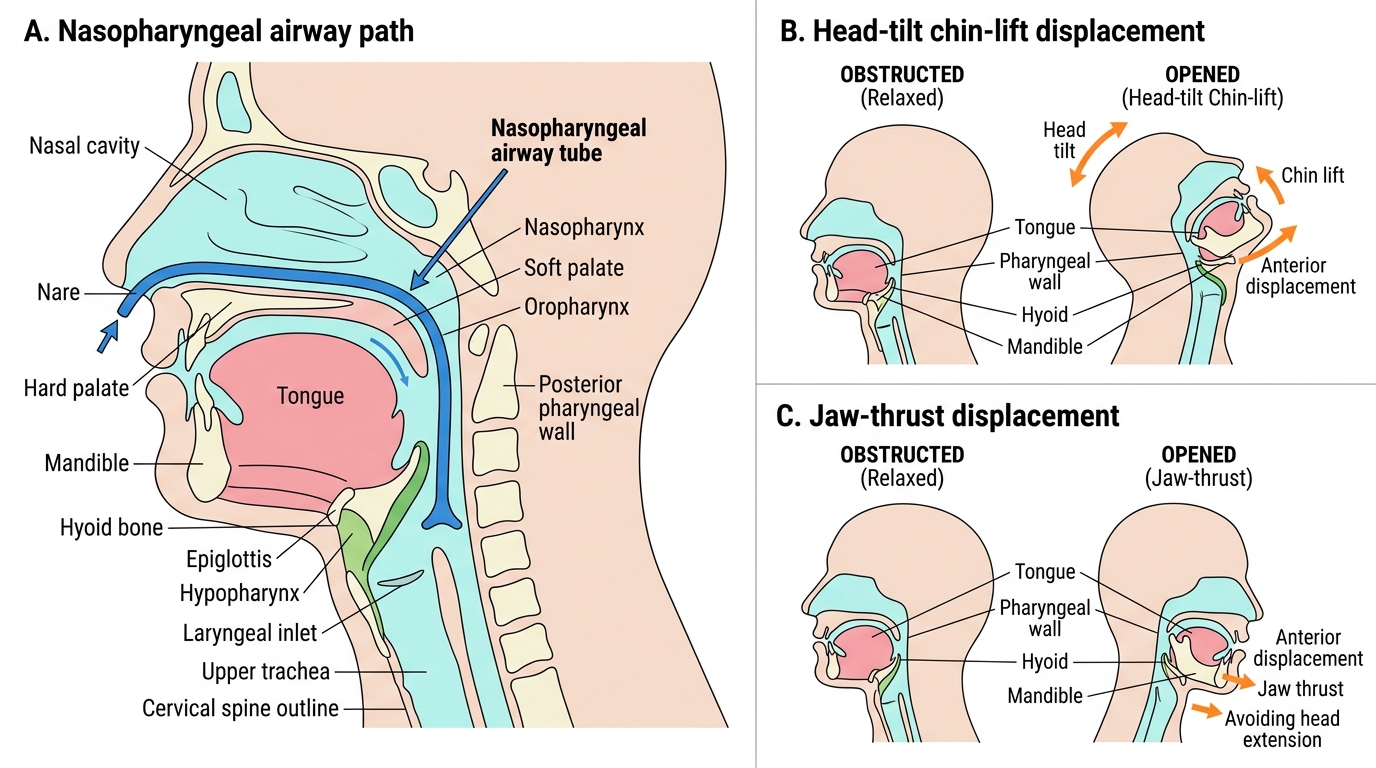
Nasopharyngeal Airway Path and Airway-Opening Manoeuvres
Head-Tilt Chin-Lift and Jaw Thrust: Technique
The head-tilt chin-lift is the standard primary airway opening manoeuvre for any unconscious patient without suspected cervical spine injury. The technique proceeds as follows: position yourself at the patient's side; place one hand on the forehead and apply firm but gentle downward pressure to tilt the head backwards (extending the atlanto-occipital joint); simultaneously place the fingertips — not the thumb — of the other hand under the bony part of the chin (the mandibular symphysis) and lift the chin upward and forward. The combined motion extends the neck and lifts the tongue and hyoid anteriorly, straightening the pharyngeal axis and opening the airway. The degree of head extension required is until the airway is patent — in adults this is typically moderate extension; in infants and young children, neutral or only minimal extension is used because the large occiput and the soft cartilaginous airway make excessive extension counterproductive and potentially obstructing.
Common errors in head-tilt chin-lift:
• Placing fingers on the soft tissue under the chin (compresses the floor of the mouth, worsening obstruction rather than relieving it — use bony chin only)
• Insufficient head tilt (partial relief only)
• Excessive head tilt in infants (can kink the trachea)
• Failure to maintain the position continuously (operator releases too early)
The jaw thrust is used when cervical spine injury is suspected (trauma, diving injuries, fall from height) because it opens the airway without extending the neck. The technique: position yourself behind the patient's head; place the tips of the index and middle fingers of both hands under the angle of the mandible (at the ramus, just anterior to the mastoid process); apply firm upward and forward pressure to lift the mandible, bringing it anterior to the maxilla; and use the thumbs to depress the lower lip to open the mouth. The jaw thrust achieves the same mechanical effect as chin-lift (anterior mandibular displacement lifts the tongue) but without neck extension. It is more tiring to maintain and typically requires two hands, making simultaneous bag-valve-mask ventilation challenging without a second rescuer.
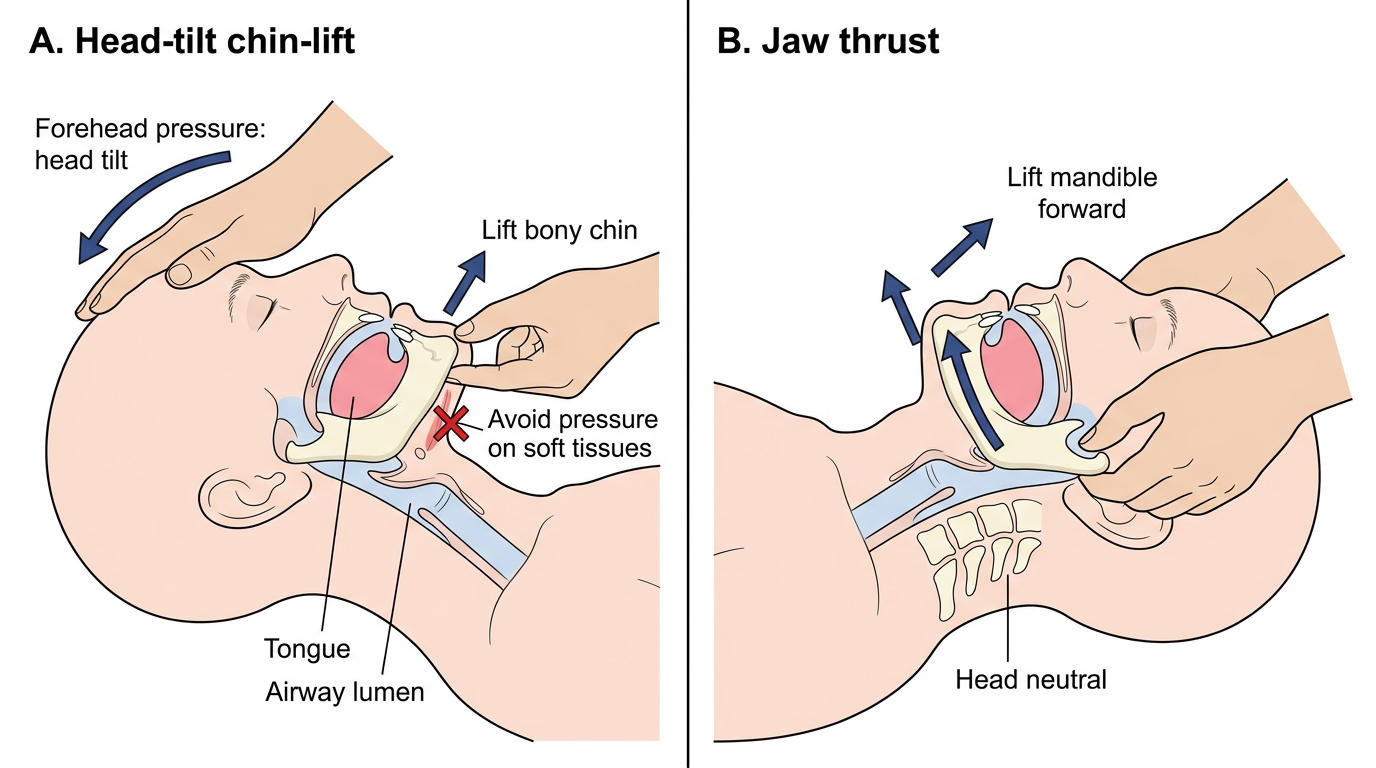
Basic Airway Opening Maneuvers