Page 9 of 15
AS3.6 | Premedication Selection and Prescription for Surgical Patients — SDL Guide (Part 2)
Monitoring and Interpretation After Premedication Administration
Once a premedication has been prescribed and administered, the patient requires monitoring until anaesthesia is induced and the anaesthetic team takes over clinical care. Monitoring after premedication is particularly important because sedative and analgesic premedications can cause respiratory depression, hypotension, or unexpected deep sedation in susceptible patients — especially the elderly, the obese, those with respiratory disease, and those with hepatic impairment (which prolongs benzodiazepine elimination).
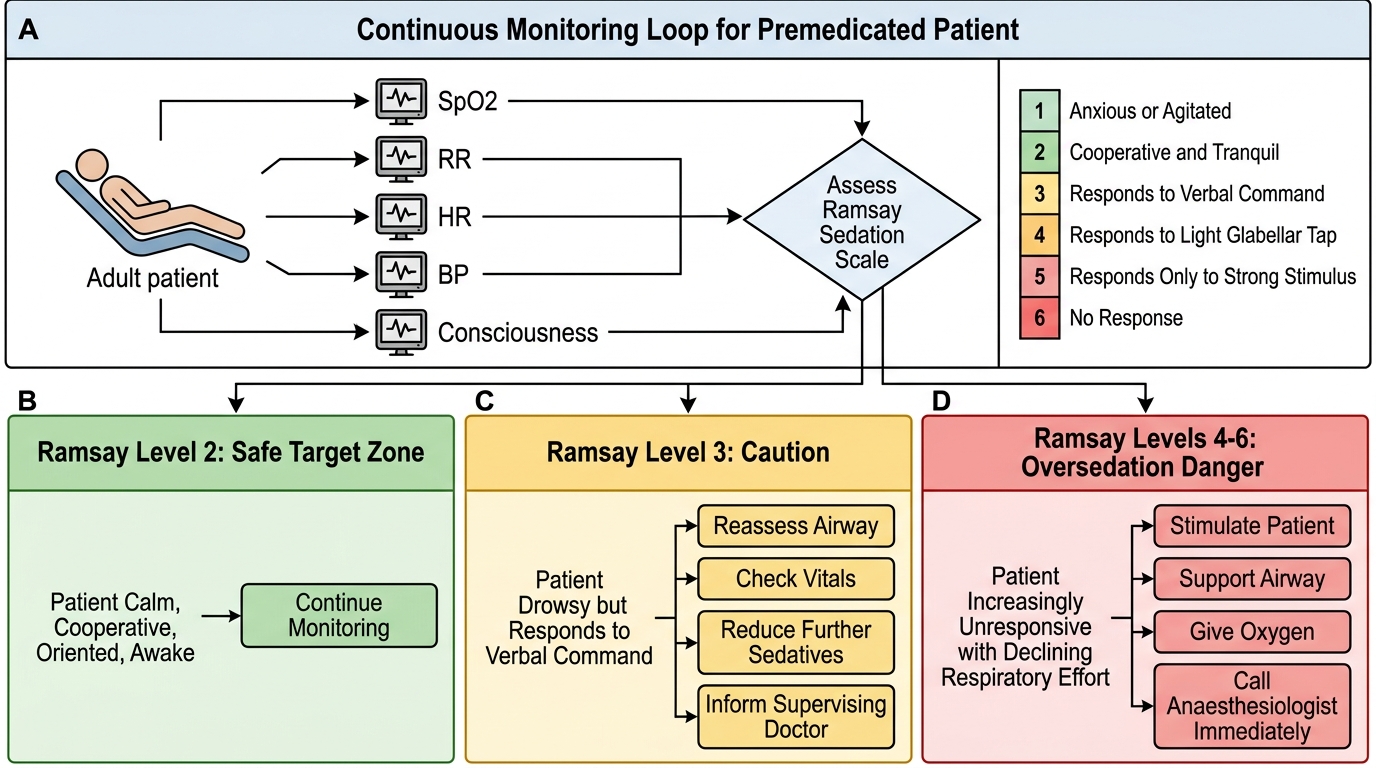
The minimum monitoring standard after any sedative premedication administered on the ward or in a preoperative holding area includes: continuous pulse oximetry (SpO2), heart rate (from the pulse oximeter), and observed respiratory rate and level of consciousness documented every 15 minutes. Supplemental oxygen should be readily available. For intravenous sedative premedications given in the anaesthetic room, the full anaesthetic monitoring setup (ECG, non-invasive blood pressure, pulse oximetry, and capnography if the patient is sedated beyond verbal communication) is mandatory.
The Ramsay Sedation Scale provides a standardised description of sedation depth: (1) anxious, agitated, or restless; (2) cooperative, oriented, and tranquil — the target level for premedication; (3) responds to commands only; (4) brisk response to glabellar tap or loud stimulus; (5) sluggish response to glabellar tap or loud stimulus; (6) no response. A patient at Ramsay level 3 or above after ward-administered premedication requires immediate review and should not be transferred to the operating theatre without anaesthetic team presence.
Interpreting the response to premedication also guides the intraoperative plan. A patient who becomes deeply sedated on a standard dose of midazolam likely has reduced drug metabolism (old age, hepatic disease) and will require lower doses of induction agent and reduced volatile agent requirements — the anaesthesiologist must be informed. A patient who remains anxious and unsedated on a standard dose may have high benzodiazepine tolerance (chronic alcohol or benzodiazepine use) and will need higher induction doses.
Specific drug effects to monitor after each premedication class:
- Midazolam: monitor for excessive sedation (Ramsay >2), respiratory depression, paradoxical agitation (especially in children and elderly — causes confusion and combativeness rather than sedation; treat with flumazenil)
- Opioids: monitor respiratory rate (should be ≥10/min), SpO2, and level of consciousness; naloxone should be available for reversal of opioid-induced respiratory depression
- Glycopyrrolate/atropine: monitor heart rate (anticholinergics cause tachycardia); check for urinary retention in elderly males (benign prostatic hyperplasia patients)
- Metoclopramide: rare but important — extrapyramidal reactions (acute dystonia, oculogyric crisis) can occur, particularly in young women; treat with procyclidine or benztropine IV
Monitoring a Premedicated Patient Using the Ramsay Sedation Scale
Applied Practice: Case-Based Premedication Decisions
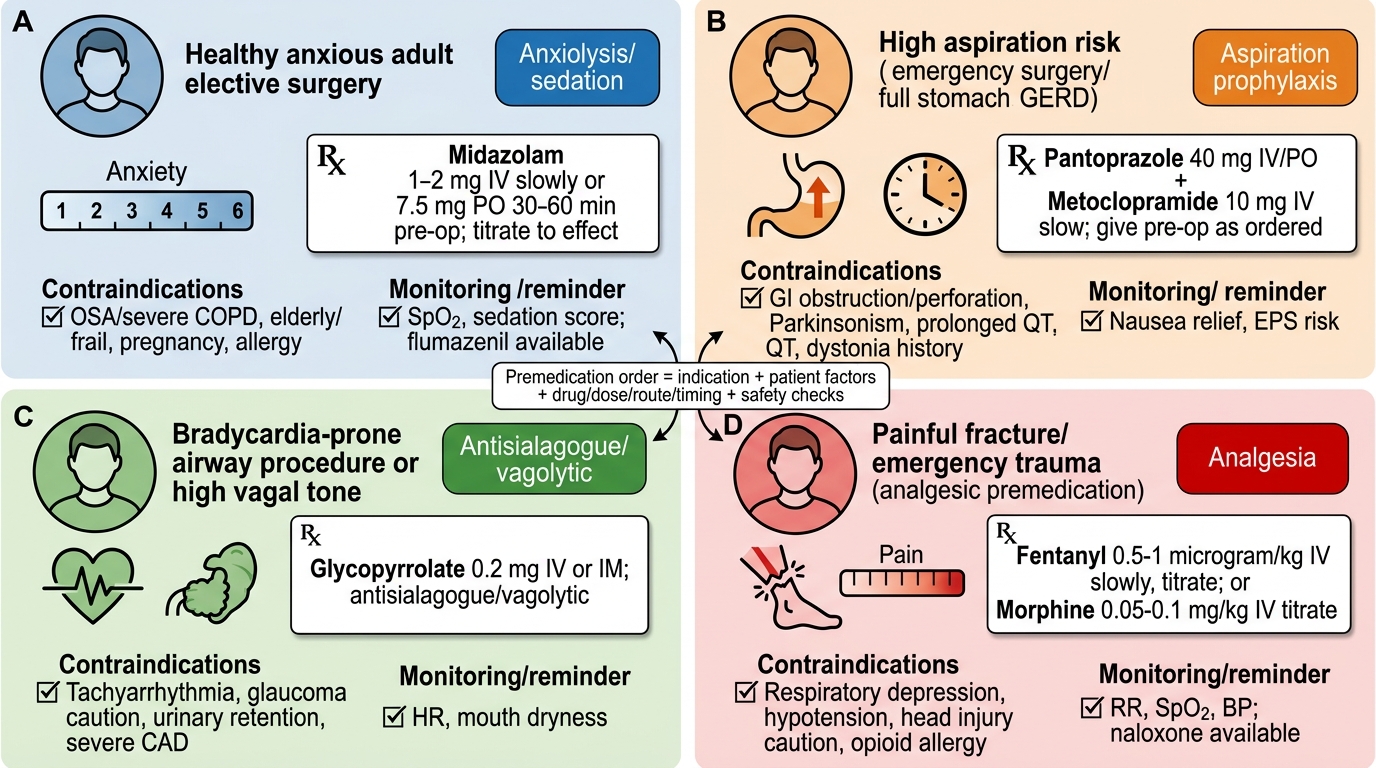
Applied prescribing skill is developed through deliberate practice with realistic clinical cases. This section presents four premedication scenarios that span the range of clinical presentations encountered in general surgical practice. For each case, the student should identify the indication, select the appropriate drug(s), determine the dose, route, and timing, identify any contraindications to first-choice agents, and write a complete prescription.
Case A: The anxious elective patient. A 28-year-old woman, ASA I, undergoing laparoscopic appendicectomy (now elective, resolved conservatively). No comorbidities, no medications, no allergies. She reports severe dental anxiety and is afraid of needles. She has never had a general anaesthetic. Functional capacity excellent (METs >8). Plan: she is an ideal candidate for oral midazolam premedication — healthy, no respiratory concerns, good functional capacity, clear indication (severe anxiety). Prescription: midazolam 5-7.5 mg orally, 30-45 minutes before anaesthesia induction. No aspiration prophylaxis needed (elective, no GORD, fasting compliant). PONV prophylaxis: moderate risk (young female, elective surgery, likely volatile agent used) — ondansetron 4 mg IV at induction.
Case B: The high-aspiration-risk patient. A 52-year-old man, ASA III, undergoing emergency laparotomy for bowel obstruction. He has not eaten for 8 hours but has been vomiting. His last meal was 6 hours ago. Diabetes mellitus with gastroparesis. Full stomach is assumed — he cannot be considered adequately fasted. Plan: aspiration prophylaxis is the primary premedication goal. Prescription: sodium citrate 0.3 M, 30 mL orally immediately before transfer to the anaesthetic room (non-particulate antacid, raises gastric pH rapidly); ranitidine 50 mg IV (over 30 minutes, if time permits — reduces ongoing acid production); metoclopramide 10 mg IV (prokinetic — accelerates gastric emptying, but partial obstruction may limit effectiveness). Midazolam is avoided (emergency, likely reduced conscious level from abdominal sepsis; benzodiazepine would worsen sedation and aspiration risk). Rapid sequence induction (RSI) is mandated.
Case C: The high-PONV-risk patient. A 35-year-old woman undergoing a 3-hour laparoscopic gynaecological procedure (myomectomy). She is a non-smoker. She had severe PONV with her last general anaesthetic 2 years ago and required admission for 24 hours of antiemetic therapy. Apfel score: 4/4 (female, non-smoker, PONV history, postoperative opioids expected). Plan: aggressive multimodal PONV prophylaxis is the priority. Prescriptions: ondansetron 8 mg IV at induction; dexamethasone 8 mg IV at induction (avoid in diabetics due to hyperglycaemia); consider scopolamine (hyoscine) patch behind the ear applied 2-4 hours before surgery (transdermal, sustained PONV prophylaxis; causes dry mouth and blurred vision — warn the patient). Midazolam 5 mg orally for anxiety — she is healthy, no respiratory concerns. Total intravenous anaesthesia (TIVA) with propofol should be strongly considered to reduce volatile-agent-related PONV trigger.
Case D: The elderly patient with multiple comorbidities. A 78-year-old man, ASA III, undergoing spinal anaesthesia for right hip replacement. He has mild cognitive impairment, moderate COPD (FEV1 60%), ischaemic heart disease (on aspirin and bisoprolol), and benign prostatic hyperplasia. Plan: most premedication drugs require dose reduction or avoidance in this patient. Benzodiazepines are high-risk (cognitive impairment, COPD — potential respiratory depression, paradoxical agitation). Anticholinergics are high-risk (urinary retention from BPH, central anticholinergic effects in cognitive impairment). Opioids are high-risk (respiratory depression, PONV, urinary retention). Spinal anaesthesia eliminates much of the need for sedative premedication. If reassurance alone is insufficient: low-dose oral midazolam 1-2 mg with close SpO2 monitoring is the most conservative pharmacological option. PONV prophylaxis may still be appropriate if sedation supplements are used. Aspiration prophylaxis: ranitidine 150 mg orally the night before and morning of surgery (standard GORD prophylaxis for elderly patients with high reflux risk).
These cases illustrate the core principle: premedication selection is never formulaic. It requires integrating the patient's goals, comorbidities, planned technique, and the pharmacological properties of available agents into a prescription that is both effective and safe for the individual in front of you.
Premedication Case Summary: Indication to Safe Order
Self-Assessment: Premedication Prescribing Competency
Prescribing competency in premedication requires integrating pharmacological knowledge, clinical assessment findings, and safe prescribing practices into a written order that another clinician can act upon without needing to query the prescriber. Self-assessment of premedication prescribing skill should focus on three dimensions: whether the indication is correctly identified, whether the drug choice and dose are appropriate for the individual patient, and whether the prescription is written in a format that is unambiguous and complete.
A practitioner who has mastered premedication prescribing can answer the following questions without hesitation for any patient on the elective or emergency surgical list: What are the five goals of premedication, and which apply to this patient? Which drug class is indicated for each goal? What are the contraindications to the first-choice agent for this patient, and what is the alternative? What dose is appropriate for this patient's age, weight, and organ function? What route and timing are appropriate? What monitoring is required after administration? What reversal agent is available if the drug causes an adverse effect?
Common prescribing errors in premedication practice that self-assessment should screen for:
1. Prescribing standard adult doses of benzodiazepines to elderly or respiratory-compromised patients without dose reduction
2. Failing to prescribe aspiration prophylaxis for high-risk patients (emergency surgery, GORD, diabetes with gastroparesis, obesity, obstetric patients)
3. Prescribing PONV prophylaxis with dexamethasone in a diabetic patient without a glucose monitoring plan
4. Prescribing metoclopramide without checking for Parkinson's disease (it worsens parkinsonian symptoms by blocking striatal dopamine D2 receptors)
5. Prescribing anticholinergics (atropine) in elderly men with benign prostatic hyperplasia without considering urinary retention risk
6. Writing an incomplete prescription — dose but no route, or route but no timing — that requires the ward nurse to contact the prescriber for clarification before administration
The habit of self-audit after every premedication prescription — asking 'Is this dose appropriate for this patient? Is the timing achievable? Is there a contraindication I have not considered?' — is the foundation of safe prescribing across all domains of medical practice, not just anaesthesia.
SELF-CHECK
A patient with Parkinson's disease on levodopa/carbidopa is scheduled for elective orthopaedic surgery. She is at high aspiration risk due to dysphagia. Which premedication is CONTRAINDICATED in this patient despite its prokinetic and antiemetic properties?
A. A. Ondansetron 4 mg IV
B. B. Sodium citrate 30 mL orally
C. C. Metoclopramide 10 mg orally
D. D. Ranitidine 150 mg orally
Reveal Answer
Answer: C. C. Metoclopramide 10 mg orally
Metoclopramide is a dopamine D2 receptor antagonist that blocks both peripheral (gastric) and central (chemoreceptor trigger zone) dopamine receptors. In patients with Parkinson's disease, dopaminergic pathways are already depleted; blocking residual D2 receptors with metoclopramide worsens parkinsonian symptoms (rigidity, tremor, akinesia) and can precipitate a Parkinsonian crisis. It is specifically contraindicated in Parkinson's disease. Domperidone is the preferred prokinetic in Parkinson's patients because it does not cross the blood-brain barrier and therefore does not worsen central dopamine deficiency. Ondansetron (5-HT3 antagonist), sodium citrate (antacid), and ranitidine (H2 blocker) are all acceptable in Parkinson's disease.
CLINICAL PEARL
Dexamethasone 4-8 mg IV at induction of anaesthesia is one of the most cost-effective and broadly applicable PONV prophylaxis measures available, but it carries two important caveats that every prescriber must know. First, it causes a clinically significant rise in blood glucose for 6-12 hours after administration — in a diabetic patient, this can cause unexpected hyperglycaemia in the postoperative period even if fasting glucose was well controlled before surgery; always alert the surgical team to check glucose at 4 and 8 hours after surgery if dexamethasone was given. Second, some anaesthesiologists give dexamethasone at the START of surgery rather than the end — the timing matters because dexamethasone takes 60-90 minutes to reach full effect; giving it at induction ensures it is active during and immediately after the procedure when PONV risk is highest. Both of these nuances are missed in routine prescribing but are clinically important when caring for diabetic patients or managing PONV in the recovery room.