Page 2 of 15
AS3.{1,4-5} | Principles, Testing and Fitness Decisions in Preoperative Evaluation — SDL Guide (Part 2)
Preoperative Investigations: Selection and Interpretation
Preoperative investigations should be chosen on the basis of what the history and examination reveal, not as a routine checklist. Indiscriminate ordering of tests wastes resources, generates false positives that trigger further unnecessary workup, and delays surgery without improving patient safety. The governing principle is that clinical indication drives investigation selection.
The investigation-ordering framework has three layers. Start with the planned procedure: major abdominal, thoracic, or vascular surgery inherently requires a wider investigation panel than a day-case laparoscopic procedure. Layer in patient age and sex: a healthy 25-year-old woman having a breast biopsy under local anaesthesia needs no routine investigations; a 72-year-old man with three comorbidities having a colectomy needs a comprehensive panel. Add comorbidity-driven tests: each active medical condition generates specific investigation needs.
Blood tests and their indications:
• Full blood count (FBC): suspected anaemia, major anticipated blood loss, patients ≥60 years. Preoperative haemoglobin below 80-100 g/L may warrant iron therapy or transfusion for elective cases.
• Urea, electrolytes, creatinine (U&E/Cr): renal disease, diabetes, hypertension, cardiac failure, diuretics or ACE inhibitors, all patients ≥60 years or before major surgery. Hypokalaemia predisposes to arrhythmias; elevated creatinine affects drug dosing.
• Blood glucose and HbA1c: all known diabetics. HbA1c above 69 mmol/mol (>8.5%) suggests poor control warranting optimisation before elective surgery.
• Coagulation screen (PT/aPTT/INR): liver disease, suspected coagulopathy, patients on anticoagulants, major surgery. Not indicated routinely in healthy patients.
• Liver function tests: liver disease, jaundice, alcohol excess, hepatotoxic drugs.
• Serum albumin: nutritional status predictor; low albumin (<35 g/L) is associated with increased surgical morbidity.
• Group and crossmatch: all surgery with anticipated major blood loss.
• Cardiac biomarkers (troponin, BNP): suspected active cardiac ischaemia or decompensated heart failure only — NOT routine.
ECG: indicated in cardiovascular disease (hypertension, IHD, CCF, arrhythmia), diabetes (risk of silent MI), and patients ≥40-50 years before major surgery. Key findings: rhythm, rate, axis, QRS morphology, ST changes, and QTc interval. Prolonged QTc (>450 ms in men, >460 ms in women) increases risk of torsades de pointes with QT-prolonging anaesthetic drugs.
Chest X-ray (CXR): indicated in suspected cardiac failure (cardiomegaly, pulmonary oedema), significant respiratory disease, or recent respiratory infection. NOT indicated routinely.
Echocardiography: indicated when a new murmur is detected, in decompensated heart failure, or when ejection fraction measurement is needed for risk stratification. A recent echocardiogram within 12 months is generally acceptable if clinical status is unchanged.
Pulmonary function tests (spirometry): indicated in suspected obstructive or restrictive lung disease, before major thoracic surgery, or for risk stratification of postoperative pulmonary complications.
The NICE (2016) and ASA guidelines explicitly advise against routine preoperative testing panels not guided by clinical findings.
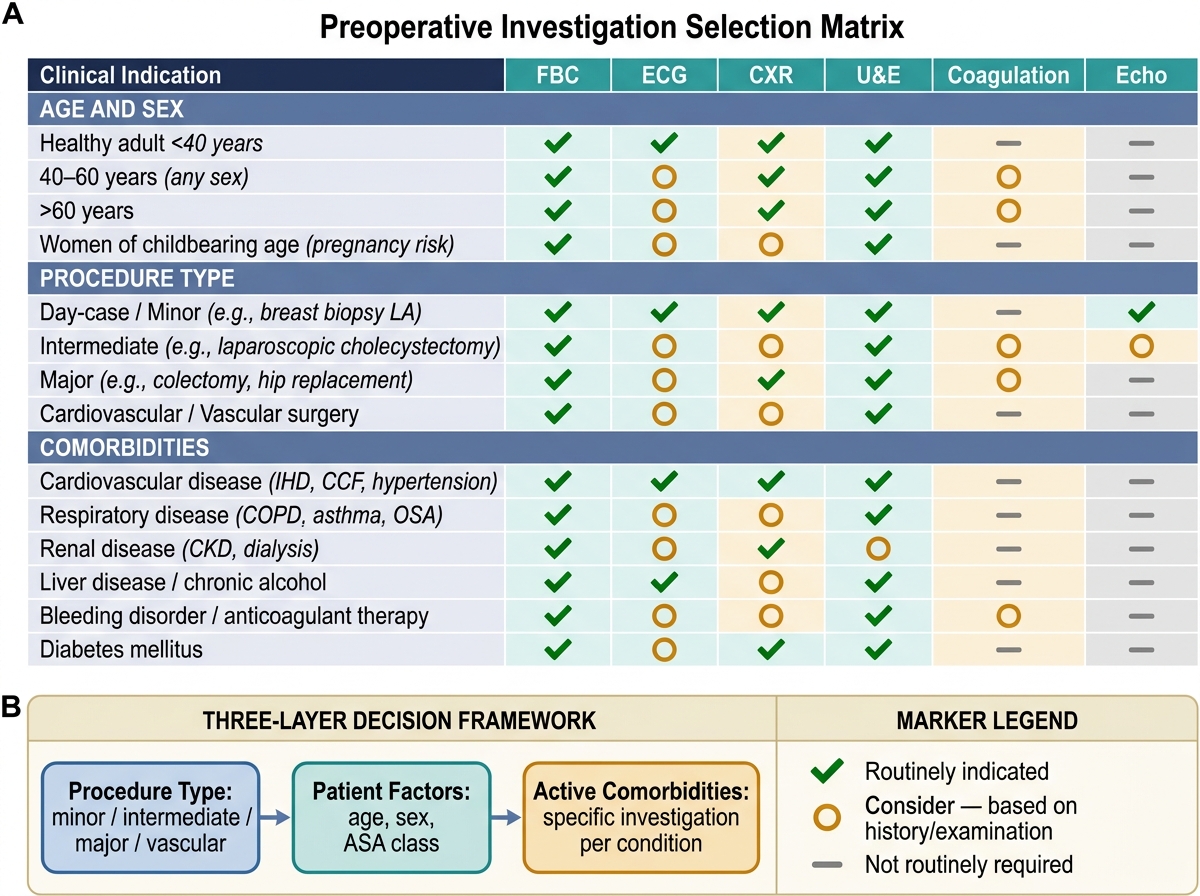
Preoperative Investigation Selection Matrix: Indication-Driven Framework
Determining Fitness for Surgery: Decision-Making and Communication
The culmination of the preoperative evaluation is a documented clinical decision about the patient's fitness for the planned anaesthetic and surgical procedure. This decision integrates all the information gathered — history, examination, investigations, risk scores — into a coherent plan communicated to the patient, the surgical team, and the postoperative care team.
Fitness for surgery is not a binary concept. It is a risk-benefit calculation in which the anaesthesiologist weighs the procedural benefit against the patient's perioperative risk, taking into account the urgency of surgery, the available optimisation time, and the patient's own values and preferences. A patient with an RCRI of 3 and an ejection fraction of 35% may be considered appropriate for an emergency life-saving laparotomy (where the alternative is death) while being deemed not optimised for an elective cholecystectomy that can wait for cardiology review.
The decision-making framework has three steps. First, identify modifiable risk factors and optimise them: hypertension (gradual control over days to weeks — acute antihypertensive loading immediately before surgery can cause hypotension); anaemia (iron therapy for iron-deficiency, erythropoietin for other causes); poorly controlled diabetes (insulin adjustment); severe valvular disease (may warrant intervention before major elective surgery); active respiratory infection (defer elective surgery by at least 4-6 weeks). Second, identify non-modifiable risk factors — age, fixed anatomy, end-stage organ disease — and factor them into technique selection (e.g., choosing spinal over general anaesthesia in severe COPD). Third, communicate the decision explicitly in the anaesthetic record: ASA class, identified risks, optimisation steps taken or recommended, and proposed anaesthetic technique with rationale. If surgery must proceed despite unoptimised risk, document the discussion with the surgical team and the patient.
Key perioperative medication management decisions:
• Antihypertensives: generally continue; ACE inhibitors/ARBs are debated — some centres hold them on the morning of surgery to prevent intraoperative hypotension
• Beta-blockers: always continue — abrupt withdrawal risks perioperative tachycardia and ischaemia
• Anticoagulants: warfarin bridging with LMWH per protocol; DOACs held 24-48 h (apixaban, rivaroxaban) or 48-96 h (dabigatran, renally adjusted)
• Antiplatelet agents: aspirin usually continued for non-cardiac surgery; P2Y12 inhibitors (clopidogrel, ticagrelor) held 5-7 days
• Diabetes medications: oral hypoglycaemics withheld on morning of surgery; insulin reduced per protocol; metformin traditionally held 24-48 h in high-risk patients due to lactic acidosis risk if perioperative renal impairment occurs
• Statins: continue — perioperative withdrawal is associated with increased cardiac events
• MAO inhibitors: traditionally stopped 2 weeks before surgery (risk of hypertensive crisis and serotonin syndrome); increasingly contested — consult prescribing psychiatrist
Consent for anaesthesia must include: the type of anaesthesia planned and why; significant common and rare risks relevant to the patient's situation; the fasting requirement; medication instructions for the day of surgery; and the planned postoperative pain management approach.
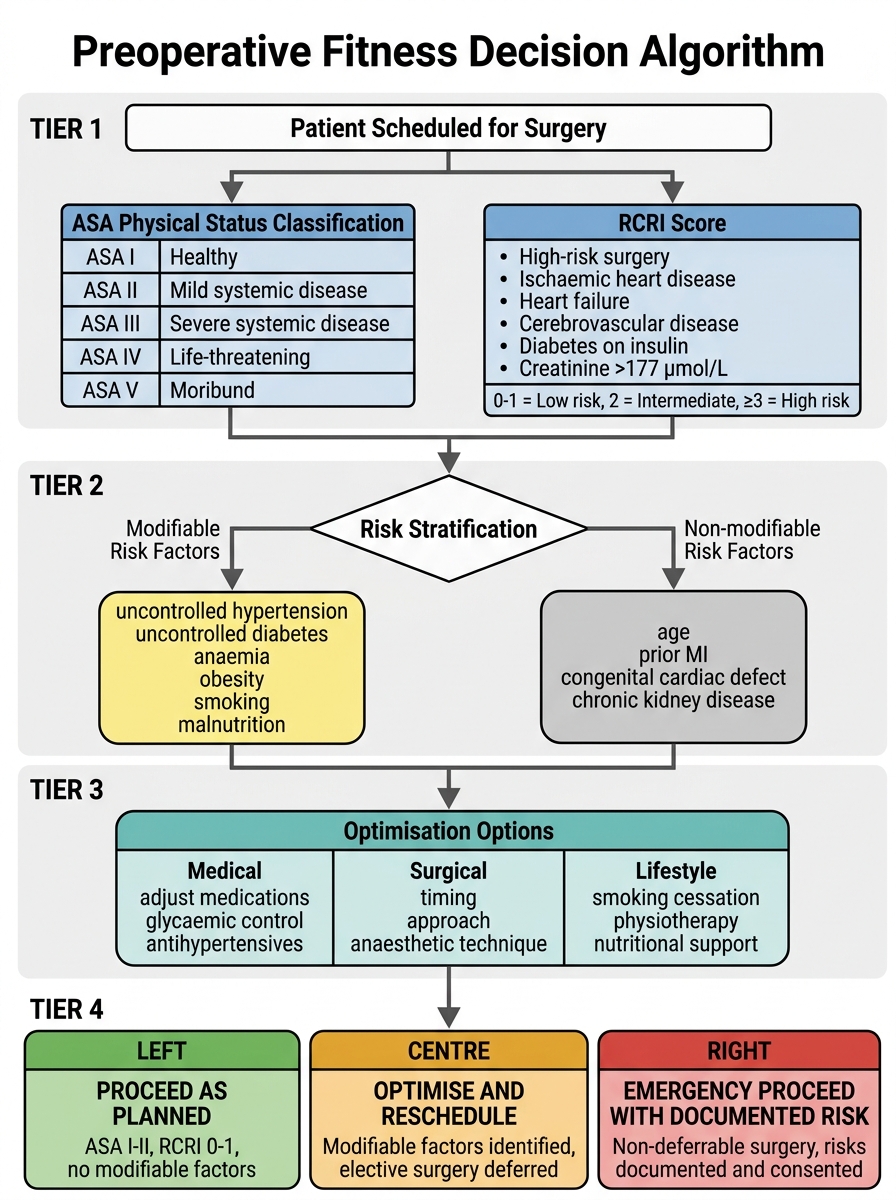
Preoperative Fitness Decision Algorithm: ASA Classification, RCRI Scoring, and Risk-Stratified Outcomes
SELF-CHECK
A 65-year-old man with well-controlled hypertension on amlodipine and atorvastatin is scheduled for an elective total knee replacement. He can climb one flight of stairs without stopping. He has no other comorbidities. What is his most likely ASA Physical Status classification?
A. A. ASA I — no systemic disease
B. B. ASA II — mild systemic disease
C. C. ASA III — severe systemic disease
D. D. ASA IV — constant threat to life
Reveal Answer
Answer: B. B. ASA II — mild systemic disease
Well-controlled hypertension on medication with no end-organ damage constitutes mild systemic disease — ASA II. ASA I is reserved for completely healthy patients with no systemic disease. ASA III would apply if his hypertension were poorly controlled (consistently 160/100 mmHg or above) or if he had significant end-organ damage. ASA IV is for conditions that are a constant threat to life (recent MI within 3 months, severe aortic stenosis, sepsis). The ability to climb stairs reflects 4 METs or more of functional capacity, which is reassuring regardless of ASA class.
Perioperative Risk Communication and Self-Assessment
Effective preoperative evaluation is not complete until the risk assessment has been communicated clearly to all stakeholders: the patient, the surgical team, and — for high-risk patients — relevant specialists such as the cardiologist or pulmonologist. This communication is both a professional obligation and a patient safety measure.
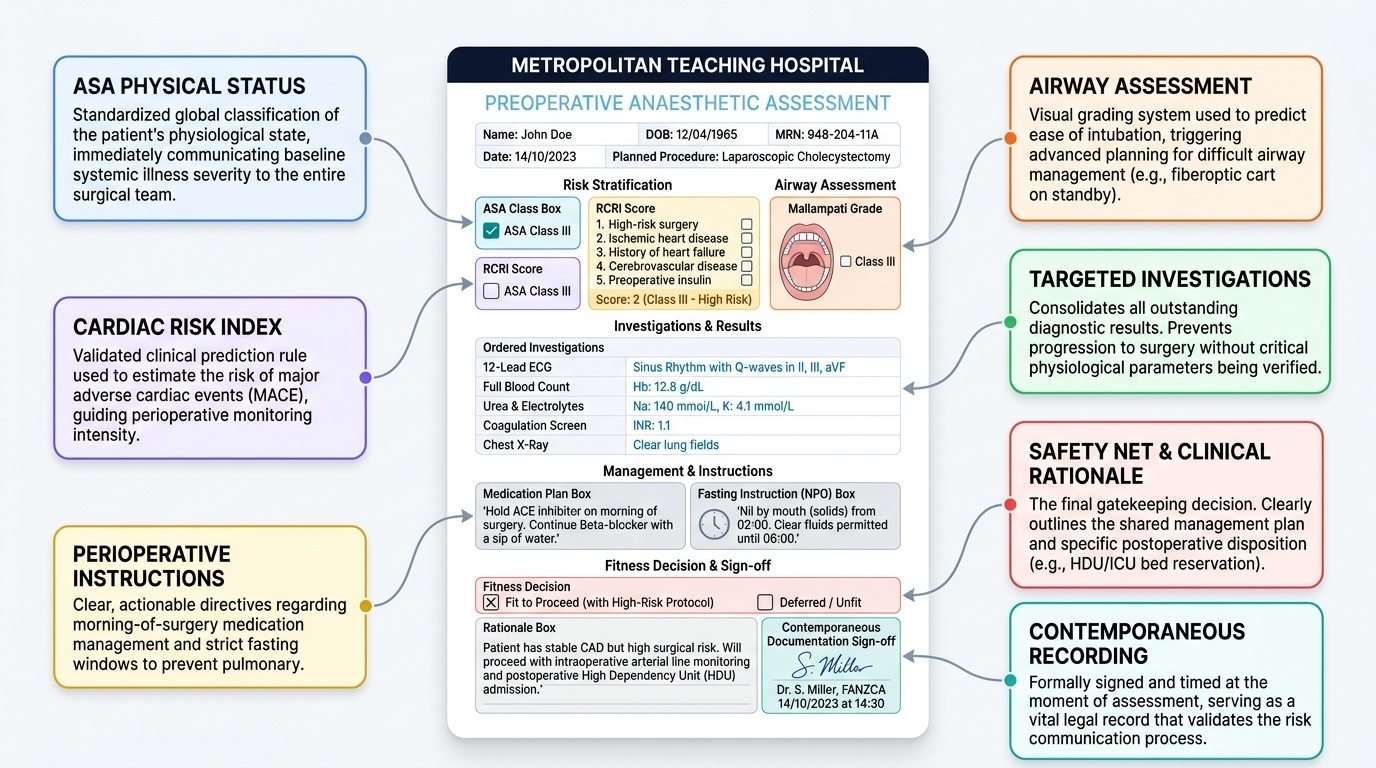
Provided image
When communicating risk to the patient, use plain language that avoids statistical abstraction. Rather than citing a percentage MACE risk figure directly, explain what the risk means practically — for example, 'your heart condition means there is a small but real risk of a heart event during or after surgery, which is why we want to ensure your medications are optimised and we will monitor your heart closely in the hours after the operation.' Involve the patient in decisions about timing, technique, and monitoring intensity wherever possible.
When communicating to the surgical team, the anaesthesiologist's written preoperative note should include: the ASA classification, the RCRI score if cardiac risk is relevant, specific concerns identified with the planned management response (for example, 'anticipated difficult airway — awake fibreoptic intubation planned; senior anaesthesiologist must be present'), any outstanding investigations and the action required before surgery proceeds, and all medication management instructions for the day of surgery.
For high-risk cases, multidisciplinary discussion before the operative list is best practice. The preoperative visit is the safety net that catches unfit patients before the point of no return. Documentation must be contemporaneous — written at the time of assessment, not reconstructed later. In medicolegal terms, an undocumented assessment did not happen.
In summary, the preoperative evaluation combines structured history, focused examination, targeted investigations, validated risk tools, and a documented risk-benefit decision into a single clinical encounter that determines the safety of the entire anaesthetic-surgical episode.
SELF-CHECK
According to the ASA preoperative fasting guidelines ('2-4-6-8 rule'), how long should a child be fasted before elective general anaesthesia if they had formula milk 5 hours ago?
A. A. The child is not adequately fasted — formula requires 6 hours
B. B. The child is adequately fasted — formula requires 4 hours
C. C. The child is adequately fasted — all milk requires 2 hours
D. D. The child needs 8 hours for any milk product
Reveal Answer
Answer: A. A. The child is not adequately fasted — formula requires 6 hours
Formula milk and non-human milk require 6 hours of fasting before elective anaesthesia, because their gastric emptying time resembles that of a light meal rather than breast milk. Breast milk (human milk) requires only 4 hours. Clear fluids (water, apple juice, black tea, black coffee) require only 2 hours. Fatty or fried food and meat require 8 hours. A child who had formula milk 5 hours ago has not yet met the 6-hour requirement and should wait at least one more hour before proceeding.
CLINICAL PEARL
The Mallampati classification and the ASA Physical Status classification are two of the most commonly confused tools in anaesthesia, yet they measure entirely different things. Mallampati grades the oropharyngeal view (airway difficulty predictor): mouth open, tongue out, no phonation — Class I (full view of uvula and tonsillar pillars) to Class IV (only hard palate visible). ASA grades systemic disease severity: Class I (healthy) to Class VI (brain-dead). A patient can simultaneously be Mallampati IV (difficult airway) and ASA I (no systemic disease) — for example, a young healthy man with a thick neck and limited mouth opening. Confusing these scales in clinical documentation or in examinations is a reliable marker of conceptual misunderstanding. Keep them separate by remembering: Mallampati is assessed in the awake patient before any sedation; ASA classification is assigned from the medical history and examination.