Page 14 of 20
AS4.6-7 | Day Care Anaesthesia and Anaesthesia Outside the Operating Room — SDL Guide (Part 2)
Management and Conduct of Day Surgery Anaesthesia
The conduct of anaesthesia for day surgery follows the same fundamental principles as inpatient anaesthesia but is optimised at every step for rapid, smooth recovery without residual sedation, nausea, or pain. The anaesthetic plan must be explicitly written around the day-surgery constraint from the outset — not simply a routine anaesthetic with the hope that the patient will happen to be well enough for discharge.
Provided image
Pre-operatively: EMLA or topical anaesthetic cream at cannulation site (reduces needle pain, particularly in children); oral premedication with anxiolytics is generally avoided (residual sedation delays discharge) unless the patient has severe preoperative anxiety (low-dose midazolam in carefully selected patients). Pre-emptive analgesia: paracetamol 1 g oral and celecoxib 200–400 mg or ibuprofen 400 mg given 1 hour before surgery reduces intraoperative and postoperative opioid requirement significantly.
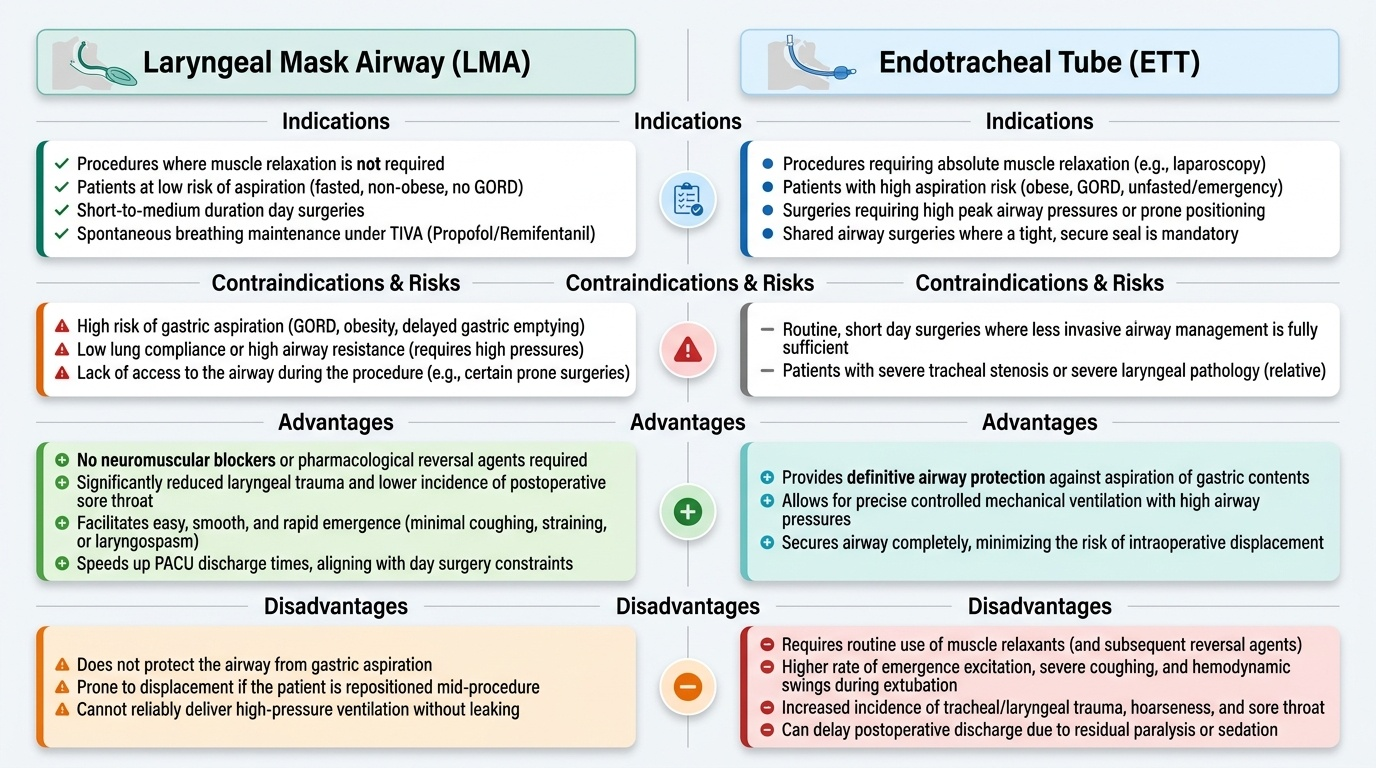
Induction: Propofol TIVA (total intravenous anaesthesia) is the technique of choice for most day surgery — propofol's antiemetic properties directly reduce PONV incidence by 25–30% compared to volatile maintenance. The laryngeal mask airway (LMA — the original Laryngeal Mask Airway or the newer second-generation i-gel) is preferred over endotracheal intubation for procedures not requiring muscle relaxation, as it avoids the need for neuromuscular blocking agents (and their reversal), reduces laryngeal trauma, and facilitates spontaneous breathing. An LMA is appropriate when: the procedure does not require muscle relaxation, the patient is not at high aspiration risk (non-obese, fasted, no GORD), and the procedure is not in a position requiring tight airway seal.
Maintenance: TIVA propofol + remifentanil infusion (TIVA) or sevoflurane/desflurane in oxygen/air. Regional or local anaesthetic techniques (field blocks, peripheral nerve blocks) should be combined wherever possible — they provide excellent postoperative analgesia with opioid sparing, dramatically reducing PONV and sedation. Ondansetron 4 mg + dexamethasone 4–8 mg IV routinely at the end of the procedure.
Emergence: Smooth, rapid; propofol TIVA produces the cleanest emergence with minimal excitation, coughing, or laryngospasm at extubation/LMA removal. Pain assessment before leaving theatre; rescue analgesia (fentanyl 25–50 mcg, morphine 2.5–5 mg) as needed.
SELF-CHECK
A 38-year-old female (BMI 24, ASA I, non-smoker) is listed for laparoscopic tubal ligation under general anaesthesia as a day surgery patient. Which anaesthetic technique best reduces her risk of unanticipated overnight admission due to PONV?
A. Thiopentone induction + isoflurane maintenance + morphine 10 mg for postoperative analgesia
B. Propofol TIVA + remifentanil + multimodal analgesia (paracetamol + ketorolac + local) + ondansetron 4 mg + dexamethasone 4 mg
C. Ketamine induction + sevoflurane maintenance + ondansetron alone
D. Propofol induction + N₂O/sevoflurane maintenance + morphine PCA
Reveal Answer
Answer: B. Propofol TIVA + remifentanil + multimodal analgesia (paracetamol + ketorolac + local) + ondansetron 4 mg + dexamethasone 4 mg
This patient has three Apfel PONV risk factors: female sex, non-smoker, and use of opioids (if prescribed). She does not yet have the fourth (history of PONV/motion sickness — not stated). The best strategy minimises all modifiable risk factors: (1) TIVA with propofol for maintenance — propofol's antiemetic properties reduce PONV by ~25–30% vs volatile agents; (2) remifentanil intraoperatively with multimodal analgesia post-procedure reduces or eliminates systemic opioid requirement; (3) dual antiemetic prophylaxis (ondansetron + dexamethasone) is evidence-based for moderate–high-risk patients. Option A is the worst choice — isoflurane, morphine, and no antiemetic prophylaxis maximise PONV risk. Option C uses ketamine (psychotomimetic emergence reactions, dysphoria) and volatile agent — worse than TIVA. Option D uses N₂O (itself mildly emetogenic in some patients), volatile agent, and systemic opioid PCA — all increase PONV risk.
Anaesthesia Outside the Operating Room (NORA): Principles and Hazards
Non-operating room anaesthesia (NORA) refers to any anaesthetic administered outside the traditional operating suite — in locations such as the radiology department (MRI, CT, interventional radiology), the endoscopy unit, the cardiac catheterisation laboratory, the electrophysiology suite, the radiotherapy suite, and the emergency department. NORA accounts for a rapidly growing proportion of anaesthetic activity — in some institutions exceeding 30% of total cases — and is associated with a disproportionately higher complication rate than equivalent procedures in the operating theatre. Understanding why this disparity exists is essential for safe NORA practice.
The core challenge of NORA is the mismatch between standard operating theatre resources and the remote environment. Remote locations frequently lack: adequate piped anaesthetic gas supply (cylinders run out, regulators fail); suction (particularly critical in endoscopy where a regurgitating patient needs immediate suction); adequately sized recovery space; immediately available trained anaesthesia nurses; anaesthetic machine vs. basic anaesthetic workstation; post-procedure monitoring equivalent to a formal PACU. Additionally, many NORA procedures involve specific environmental hazards: MRI presents the most extreme environment — all ferromagnetic equipment (standard laryngoscopes, oxygen cylinders, infusion pumps) is unsafe within the magnetic field; only MR-conditional or MR-safe equipment may be used; the magnetic field and radiofrequency pulses generate electromagnetic interference that can affect monitoring and pacemakers.
The guiding principle for safe NORA is to bring the operating theatre to the patient — that is, to replicate the safety standards of the operating suite in the remote location as completely as possible. This means: dedicated anaesthetic equipment checked to theatre standard before every case; piped O₂ plus cylinder backup; suction immediately available and tested; monitoring identical to intraoperative standards (SpO₂, ECG, ETCO₂, NIBP); trained personnel; a clearly defined and rehearsed emergency protocol for cardiac arrest and airway crisis in that specific location.
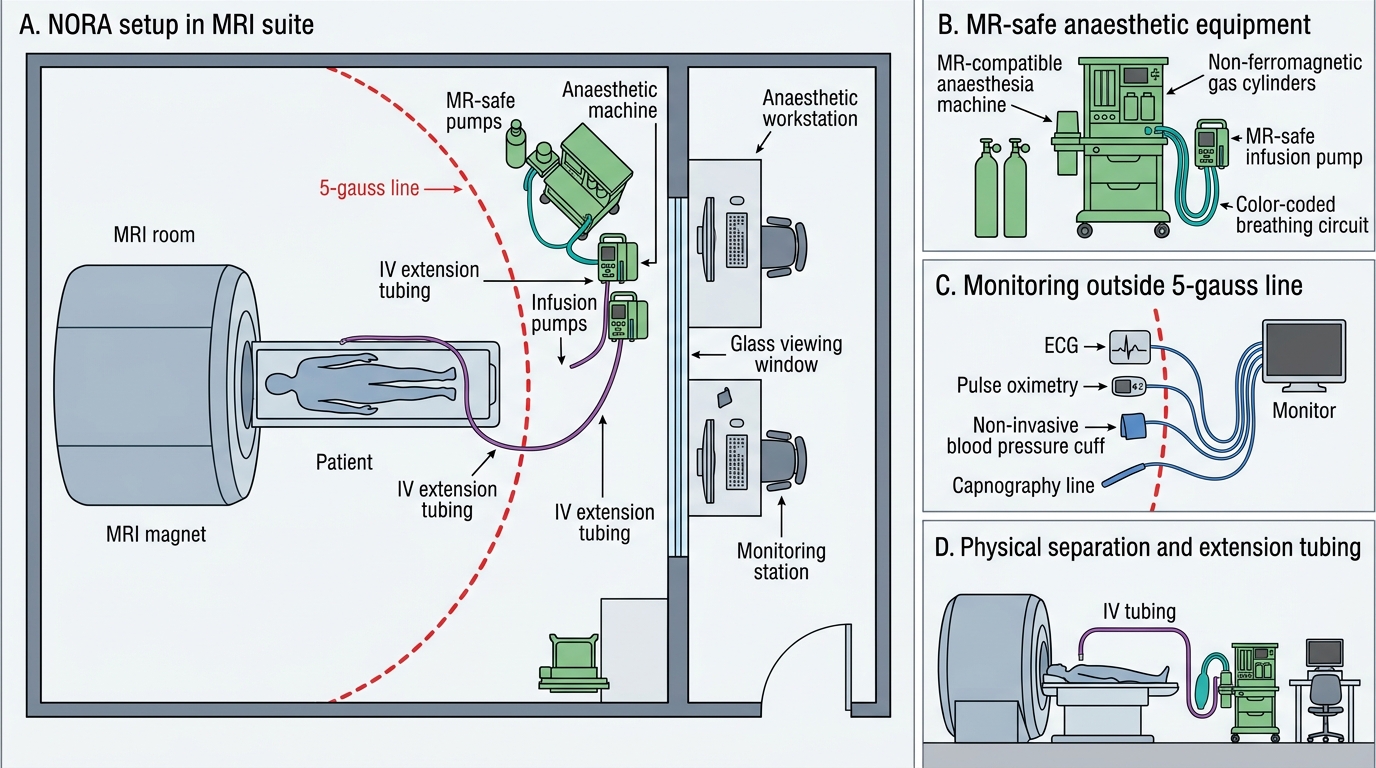
NORA Setup in an MRI Suite
Self-Assessment: Day Surgery and NORA Decision-Making
To confirm your understanding of AS4.6–AS4.7 at the required clinical reasoning level, work through the following scenarios and answer the questions before reviewing the solutions.
Scenario 1 — Day surgery selection: A 58-year-old male with well-controlled type 2 diabetes (HbA1c 7.2%), hypertension (BP 138/84 on enalapril), and a BMI of 32 presents for elective inguinal hernia repair under day surgery. Is he suitable for day surgery? What specific adjustments would you make to his anaesthetic plan and perioperative diabetes management? What discharge criteria must be specifically confirmed before he goes home?
Scenario 2 — Fast-track technique: You are planning anaesthesia for a 26-year-old woman (ASA I, BMI 21) for diagnostic laparoscopy (expected 25 minutes) as a day case. Design a complete anaesthetic: premedication, technique of induction and maintenance, airway management, analgesic plan, antiemetic prophylaxis, and recovery strategy. Justify each choice in terms of its contribution to fast-track discharge.
Scenario 3 — NORA safety: The gastroenterology team asks you to provide propofol sedation for a 70-year-old man (BMI 38, known GORD, snores heavily) for a colonoscopy in the endoscopy unit. The unit has SpO₂ monitoring and a simple facemask oxygen source but no suction machine or capnography. What are the specific risks in this patient and this environment? Would you agree to perform the sedation under these conditions? If not, what minimum requirements must be met before you agree to proceed?
Reflect on each answer: what specific pharmacological, physiological, or environmental principle does each scenario test? This pattern of 'principle behind the decision' is the level of reasoning expected in your anaesthesia portfolio entries and professional assessments.
CLINICAL PEARL
PONV is the dominant failure mode of day surgery. Postoperative nausea and vomiting accounts for the largest share of unanticipated admissions after planned day surgery — more than pain, more than bleeding, more than urinary retention. The Apfel simplified risk score assigns 1 point each for: female sex, non-smoker, history of PONV or motion sickness, and planned postoperative opioid use. A score of 3–4 warrants triple therapy (propofol TIVA + ondansetron + dexamethasone). Understanding the Apfel score and applying multimodal PONV prophylaxis proactively — not reactively — is one of the highest-impact interventions in day surgery anaesthesia.