Page 2 of 20
AS4.1 | Pharmacology of Drugs Used in General Anaesthesia — SDL Guide (Part 2)
Muscle Relaxants: Depolarising Agents
Neuromuscular blocking agents (NMBAs) facilitate endotracheal intubation by relaxing the jaw and laryngeal muscles, improve surgical access, and prevent patient movement during delicate procedures. They are classified by mechanism of action at the neuromuscular junction (NMJ) into depolarising and non-depolarising types — a distinction with profound clinical consequences for monitoring, reversal, and adverse-effect management.
Suxamethonium (succinylcholine) is the sole clinically used depolarising NMBA. It is structurally two acetylcholine molecules joined end-to-end. At the NMJ, suxamethonium binds nicotinic receptors and, like acetylcholine, produces sustained depolarisation of the motor end-plate. However, because it is not hydrolysed by acetylcholinesterase (it is hydrolysed by plasma cholinesterase, also called pseudocholinesterase), depolarisation is prolonged, preventing repolarisation and rendering the muscle temporarily refractory to further stimulation — this constitutes the neuromuscular block (called Phase I block, depolarising block, characterised by fasciculations followed by flaccid paralysis).
The clinical dose is 1–1.5 mg/kg IV, producing complete neuromuscular blockade within 60 seconds — the fastest-onset NMBA available. This rapid, reliable onset makes suxamethonium the drug of choice for rapid-sequence induction (RSI) in patients at risk of aspiration. Duration is short (8–12 minutes) because plasma cholinesterase rapidly hydrolyses it.
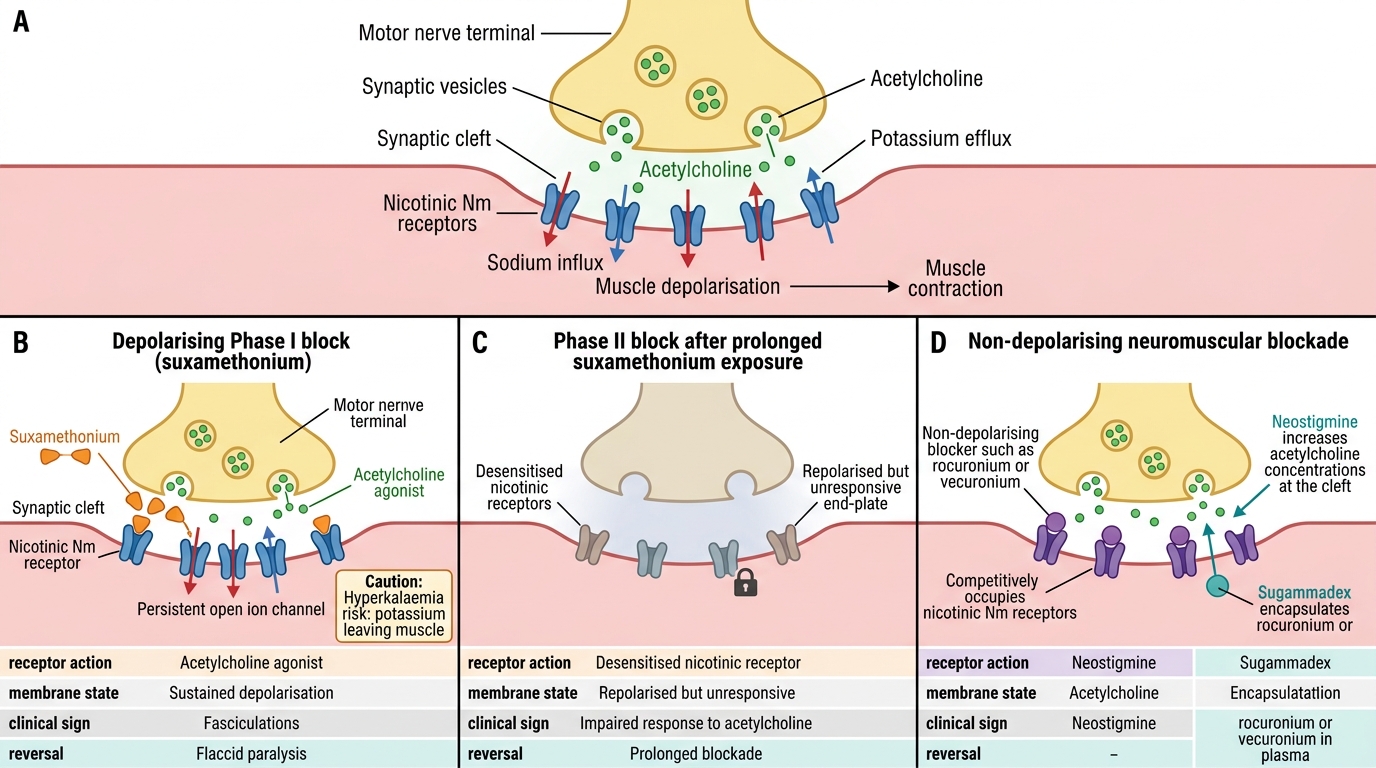
Depolarising vs Non-Depolarising Neuromuscular Blockade
Critical adverse effects of suxamethonium:
- Hyperkalaemia: depolarisation causes potassium efflux from muscle; in healthy patients serum K rises ~0.5 mEq/L (harmless). However, in patients with burns, massive trauma, prolonged immobilisation, denervation injuries (e.g., spinal cord injury ≥24 hours old), neuromuscular diseases, or crush injuries, up-regulation of extrajunctional acetylcholine receptors leads to massive, potentially fatal hyperkalaemia — suxamethonium is absolutely contraindicated in these conditions.
- Malignant hyperthermia (MH): suxamethonium (along with potent inhalational agents) is a known MH trigger. MH is an autosomal dominant pharmacogenetic disorder of the ryanodine receptor (RYR1), causing uncontrolled calcium release from the sarcoplasmic reticulum, leading to explosive skeletal muscle hypermetabolism with hyperthermia (temperature rising >1°C every 5 minutes), muscle rigidity, acidosis, hypercapnia, rhabdomyolysis, and coagulopathy. It is immediately life-threatening. Treatment: dantrolene (2.5 mg/kg IV, repeated as needed), cooling, correct acidosis. Suxamethonium must be avoided in any patient with personal/family history of MH.
- Bradycardia / asystole: suxamethonium stimulates all cholinergic receptors; children are especially susceptible to profound bradycardia with the second dose (hence atropine premedication is recommended in paediatric patients).
- Raised intraocular pressure: avoid in open-eye injury (risking extrusion of intraocular contents).
- Raised intragastric pressure: simultaneously raises the lower oesophageal sphincter tone, so net regurgitation risk is not necessarily increased — but this is a contextual judgment.
- Prolonged block: in patients with congenital or acquired plasma cholinesterase deficiency (including those on organophosphates), block may last hours; management is supportive ventilation.
- Postoperative muscle pains: fasciculations cause myalgia, especially in ambulatory patients.
Muscle Relaxants: Non-Depolarising Agents and Their Reversal
Non-depolarising NMBAs act as competitive antagonists at the nicotinic acetylcholine receptor on the motor end-plate, occupying the receptor without activating it and thereby preventing acetylcholine from triggering depolarisation. Unlike suxamethonium, non-depolarising agents do not cause initial fasciculations, and their block can be reversed pharmacologically once the surgical requirement for relaxation has passed. The key clinical variables across this drug class are: speed of onset (how quickly the block is established), duration of action (short, intermediate, or long), route of elimination (hepatic, renal, or spontaneous), and cardiovascular side-effect profile (particularly histamine release and autonomic ganglionic effects). Choosing the right non-depolarising NMBA requires matching these pharmacokinetic and pharmacodynamic characteristics to the surgical procedure, the patient's organ function, and the intended reversal strategy.
Non-depolarising NMBAs are classified by onset and duration:
- Short-acting: mivacurium (metabolised by plasma cholinesterase; spontaneous recovery in 15–20 min; avoid in cholinesterase deficiency)
- Intermediate-acting: vecuronium (steroidal; minimal cardiovascular effects; hepatic elimination; widely used), rocuronium (rapid onset among non-depolarisers — at 1.2 mg/kg it approaches suxamethonium onset for RSI; steroidal; primary choice when suxamethonium is contraindicated), atracurium (benzylisoquinolinium; Hofmann elimination — degraded spontaneously at physiological temperature and pH, independent of renal/hepatic function — ideal in organ failure; releases histamine at high doses; laudanosine metabolite causes CNS excitation in very high levels)
- Long-acting: pancuronium (steroidal; vagolytic → tachycardia and hypertension; renal elimination → prolonged effect in renal failure), d-tubocurarine (the original curare alkaloid; large histamine release; largely historical now)
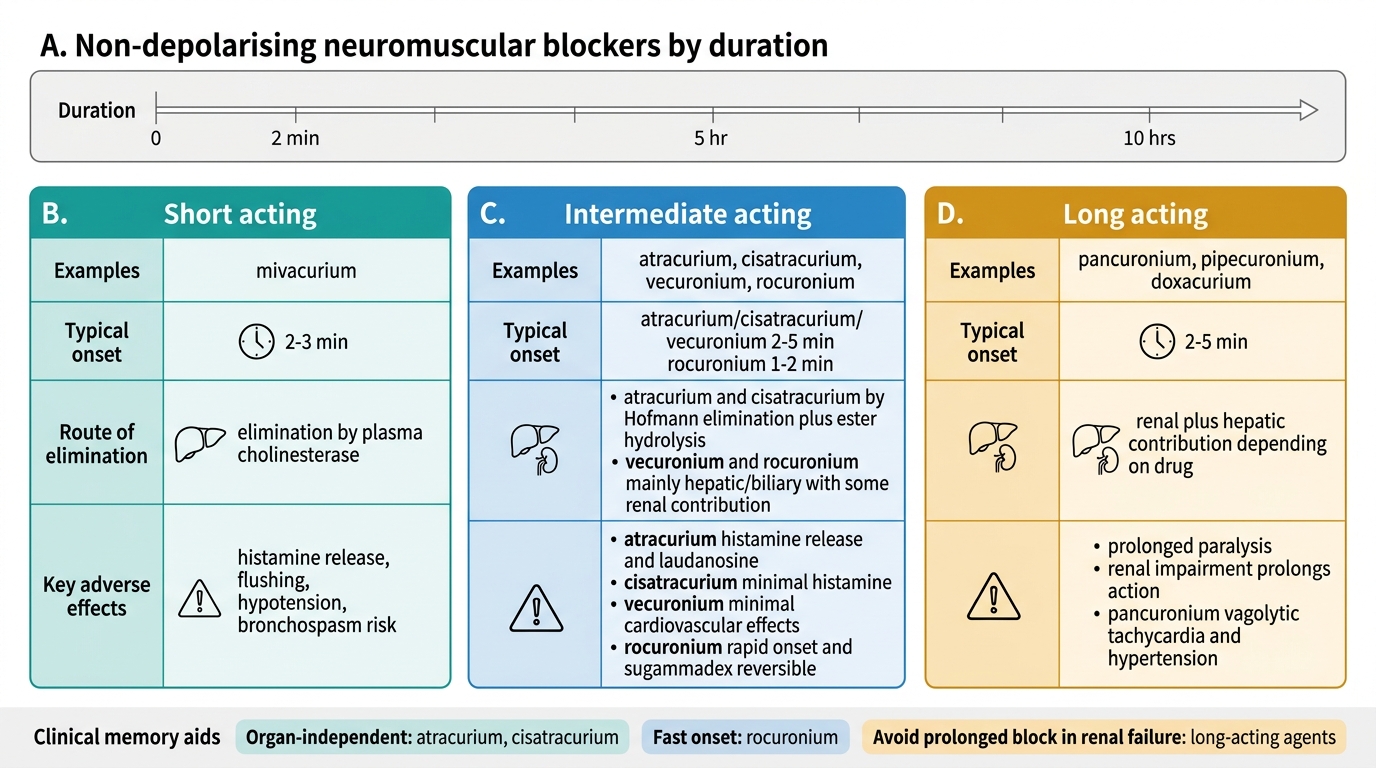
Classification of Non-Depolarising Neuromuscular Blockers
Reversal of non-depolarising block is accomplished by raising acetylcholine concentration at the NMJ to compete with (and displace) the blocking agent. Anticholinesterases inhibit the enzyme acetylcholinesterase, preventing acetylcholine breakdown and allowing it to accumulate at the end-plate. The three agents used are neostigmine (most common; dose 0.05–0.07 mg/kg, max ~5 mg), edrophonium (short-acting, largely replaced), and pyridostigmine (longer-acting; less used intraoperatively).
A critical practical rule: anticholinesterases are quaternary ammonium compounds that cannot cross the blood-brain barrier — they inhibit peripheral but not central cholinesterase. However, they simultaneously inhibit muscarinic acetylcholine receptors throughout the body, causing bradycardia, bronchospasm, hypersalivation, increased GI motility, and miosis. These muscarinic side effects are counteracted by co-administering an anticholinergic drug — glycopyrrolate (the preferred partner; does not cross BBB; 0.2 mg per 1 mg neostigmine) or atropine (crosses BBB; causes tachycardia and pupillary dilation; less preferred). The combination must always be administered together — giving neostigmine without an anticholinergic risks severe bradycardia and bronchospasm.
Sugammadex represents a paradigm shift in reversal: it is a modified gamma-cyclodextrin that directly encapsulates steroidal NMBAs (rocuronium > vecuronium) in a 1:1 complex, rapidly removing them from the NMJ without muscarinic side effects, and requiring no anticholinergic co-administration. Dose for reversal of rocuronium at various degrees of block: 2 mg/kg (moderate block, 2+ PTC), 4 mg/kg (deep block), 16 mg/kg (immediate reversal post-RSI dose). Sugammadex is the reversal agent of choice where available and is the only agent capable of reliably reversing deep rocuronium block — a potential life-saving option in cannot-intubate-cannot-oxygenate scenarios where a 1.2 mg/kg rocuronium RSI has been used.
SELF-CHECK
A 35-year-old male with a 3-day-old spinal cord injury at C6 level requires emergency surgery. Which induction agent should be avoided and why?
A. Propofol — because it causes severe cardiovascular depression in spinal cord injury
B. Ketamine — because it raises ICP in all spinal injuries
C. Suxamethonium — because denervation causes up-regulation of extrajunctional receptors leading to massive hyperkalaemia on depolarisation
D. Etomidate — because it causes severe adrenal suppression in neurological injury
Reveal Answer
Answer: C. Suxamethonium — because denervation causes up-regulation of extrajunctional receptors leading to massive hyperkalaemia on depolarisation
After the first 24 hours following denervation or immobilisation injury, acetylcholine receptors up-regulate across the entire muscle membrane surface (not just at the NMJ). Suxamethonium depolarises all of these receptors simultaneously, releasing a massive amount of potassium into the circulation — potentially causing fatal hyperkalaemia and cardiac arrest. This risk persists for months to years after the injury. The correct answer is C. Propofol is indeed used cautiously for cardiovascular depression, but is not 'avoided' — it can be titrated carefully. Etomidate causes adrenal suppression but is not specifically contraindicated in spinal cord injury. Ketamine raises ICP but only caution (not absolute avoidance) applies unless concurrent head injury is present.
Clinical Context: Selecting and Combining Agents for Balanced Anaesthesia
Modern general anaesthesia is based on the concept of balanced anaesthesia — the deliberate use of multiple drugs, each at a lower dose, to achieve the four components of anaesthesia (unconsciousness, analgesia, amnesia, muscle relaxation) while minimising the dose-related adverse effects of any single agent. A typical balanced anaesthetic for elective adult surgery is structured as follows:
Premedication: An anxiolytic (e.g., oral midazolam or lorazepam) may reduce patient anxiety and provide anterograde amnesia. Preoperative fasting must be confirmed — ASA guidelines recommend: clear fluids up to 2 hours before anaesthesia; breast milk 4 hours; formula/light meal 6 hours; fatty/fried/full meal 8 hours (the "2-4-6-8 rule"). Blanket "nil by mouth from midnight" is no longer accepted practice.
Preoxygenation: 3–5 minutes of 100% oxygen by tight-fitting mask denitrogenates the functional residual capacity, extending the safe apnoeic period before intubation from ~1 min (on room air) to ≥3–5 minutes (on oxygen).
Induction: IV access confirmed, monitoring applied (ECG, SpO₂, NIBP). Fentanyl 1–2 mcg/kg IV (or equivalent opioid) is given first to blunt the laryngoscopy stimulus. Propofol 1.5–2.5 mg/kg IV is titrated to effect (loss of response to verbal command, apnoea). In haemodynamically unstable patients, ketamine 1–2 mg/kg or etomidate 0.2–0.3 mg/kg is used instead.
Airway and relaxation: For intubation — a non-depolarising agent (vecuronium 0.1 mg/kg, rocuronium 0.6 mg/kg; or in RSI, rocuronium 1.2 mg/kg or suxamethonium 1.5 mg/kg) is given after induction. The timing of muscle relaxant relative to intubation is critical.
Maintenance: Typically sevoflurane or isoflurane in oxygen/air or oxygen/N₂O, titrated to clinical signs and end-tidal concentration (monitored as multiples of MAC). Additional opioid boluses or infusion (fentanyl/remifentanil) as required. Depth of anaesthesia monitoring (BIS, Entropy) is increasingly used to avoid awareness under anaesthesia while minimising over-dosing.
Emergence: Inhalational agent discontinued, reversal given (neostigmine + glycopyrrolate, or sugammadex), spontaneous ventilation confirmed before extubation. Adequate reversal confirmed by train-of-four (TOF) monitoring — TOF ratio ≥0.9 indicates clinically adequate recovery of neuromuscular function.
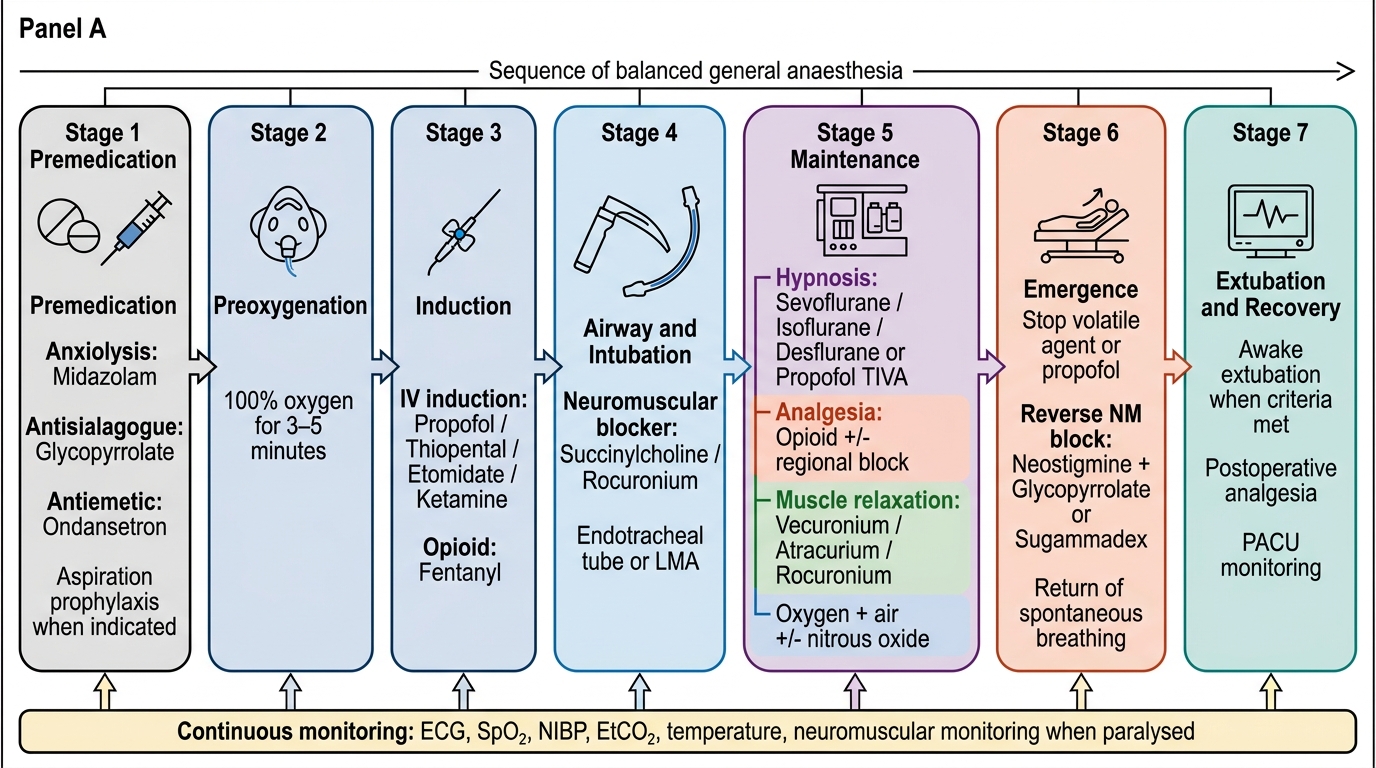
Balanced General Anaesthesia Sequence