Page 10 of 17
AS5.5 | Caudal Epidural Technique in Adults and Children — SDL Guide (Part 2)
Technique: Caudal Epidural Block in Adults
The adult caudal technique differs from the paediatric approach in several important respects driven by anatomical differences: greater body mass, more variable sacral hiatus anatomy, deeper subcutaneous fat obscuring the sacral cornua, higher incidence of fusion or stenosis of the hiatus, and the dural sac ending higher (at S2) — giving more margin before dural puncture, but a greater technical challenge in landmark identification.
Positioning: Prone is preferred in adults for caudal injection in the pain clinic or theatres (e.g., for haemorrhoidectomy anaesthesia), with a pillow under the lower abdomen/pelvis to reduce lumbar lordosis and open the sacral cleft. Left lateral decubitus is used when the patient cannot tolerate prone (e.g., pregnancy, severe respiratory disease).
Landmark identification: The sacral cornua are the definitive landmarks. In adults, palpate the coccyx first (midline, most inferior structure), then move superiorly to feel the slight depression of the hiatus flanked by the cornua. In obese patients, the cornua may not be palpable. Ultrasound guidance is increasingly used in adults to identify the hiatus, confirm correct needle placement in the sacral canal, and visualise LA spread — a practice strongly recommended in training settings and in patients with abnormal anatomy.
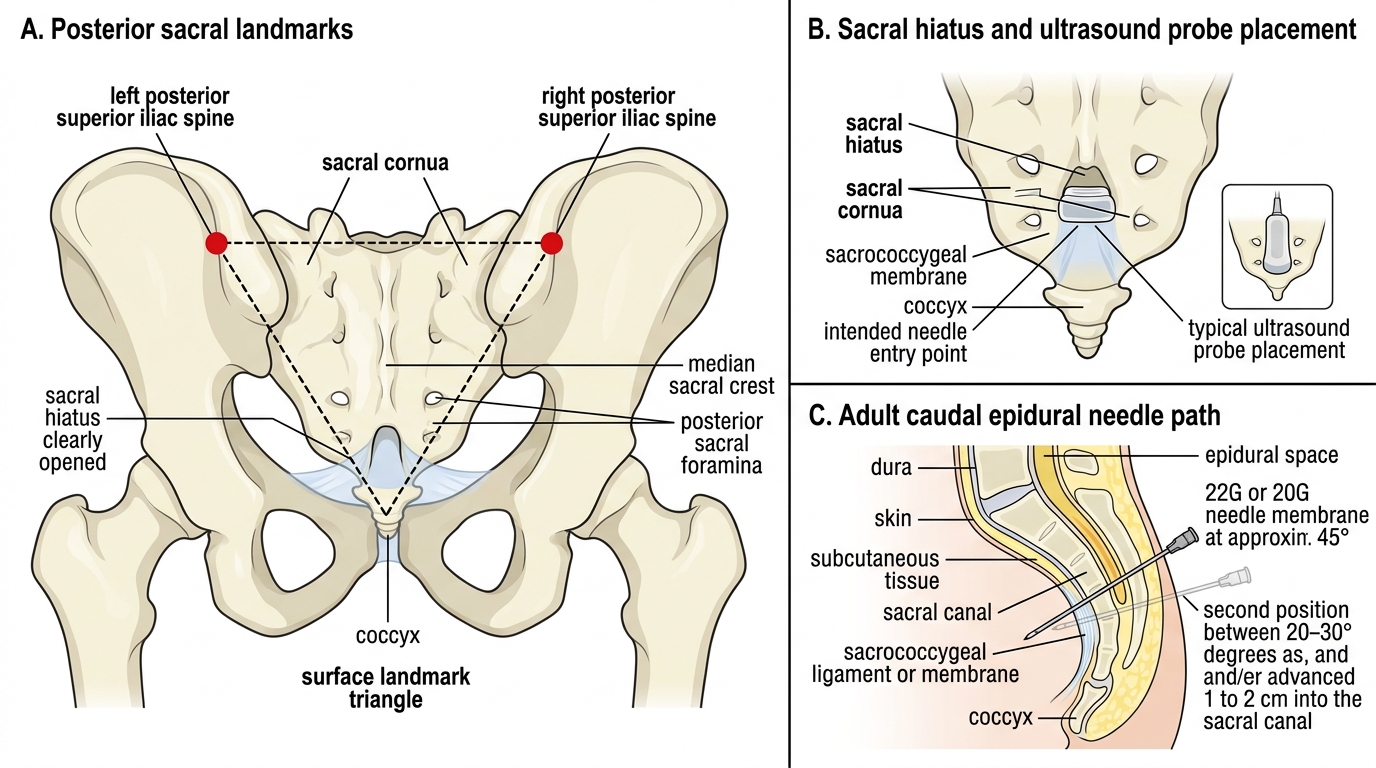
Adult Caudal Epidural Landmarks
Needle insertion: A 22G or 20G needle is inserted at approximately 45° through the sacrococcygeal membrane, felt as a loss of resistance or pop. The needle is then lowered to 20–30° and advanced 1–2 cm into the sacral canal. In adults, the standard aspiration protocol (no blood, no CSF) is essential before injection. A test dose (3 mL of LA with 1:200,000 adrenaline) can identify intravascular placement (tachycardia ≥ 20 bpm within 60 seconds) or subarachnoid injection (dense sacral motor block within 2 minutes).
Drug dosing in adults: Unlike paediatric practice, adult dosing is site-dependent rather than weight-dependent. For sacral/perineal surgery: 15–20 mL of 1.5–2% lignocaine with 1:200,000 adrenaline, or 10–15 mL of 0.5% bupivacaine. The larger volume (compared to lumbar epidural) is needed because the sacral epidural space has a large capacity and LA spreads caudally before travelling cephalad, requiring greater volume for consistent segmental coverage. Note the maximum dose: 0.5% bupivacaine × 20 mL = 100 mg; in a 60 kg adult this is 1.67 mg/kg — within the 2 mg/kg limit. For lignocaine with adrenaline: 2% × 20 mL = 400 mg in a 60 kg adult = 6.7 mg/kg, close to the 7 mg/kg limit — acceptable but at the upper margin.
Monitoring and Interpretation of Caudal Block
Post-caudal monitoring combines the assessment principles used for all neuraxial blocks with the specific features of sacral nerve distribution. The approach differs between paediatric (where the patient is under GA and communication is absent) and adult (where verbal feedback guides assessment).
In children under GA: Direct assessment of block adequacy is impossible while anaesthesia is maintained. Indirect indicators during surgery include the absence of haemodynamic response (no tachycardia or hypertension) to surgical stimulation — in a properly blocked child, the heart rate and blood pressure remain stable even during wound incision and traction. If the heart rate rises during surgery, the anaesthetist should consider whether the block level is insufficient for the procedure (e.g., the herniotomy involves peritoneal traction above the block level — peritoneal innervation from T10 is not reliably covered by a lumbo-sacral caudal). The primary assessment occurs in the recovery room and postoperatively: a successfully blocked child wakes with no pain, minimal crying, and age-appropriate orientation. Motor block in the legs — the child cannot move their lower limbs immediately post-block — is expected and should be clearly communicated to recovery nurses to avoid alarm.
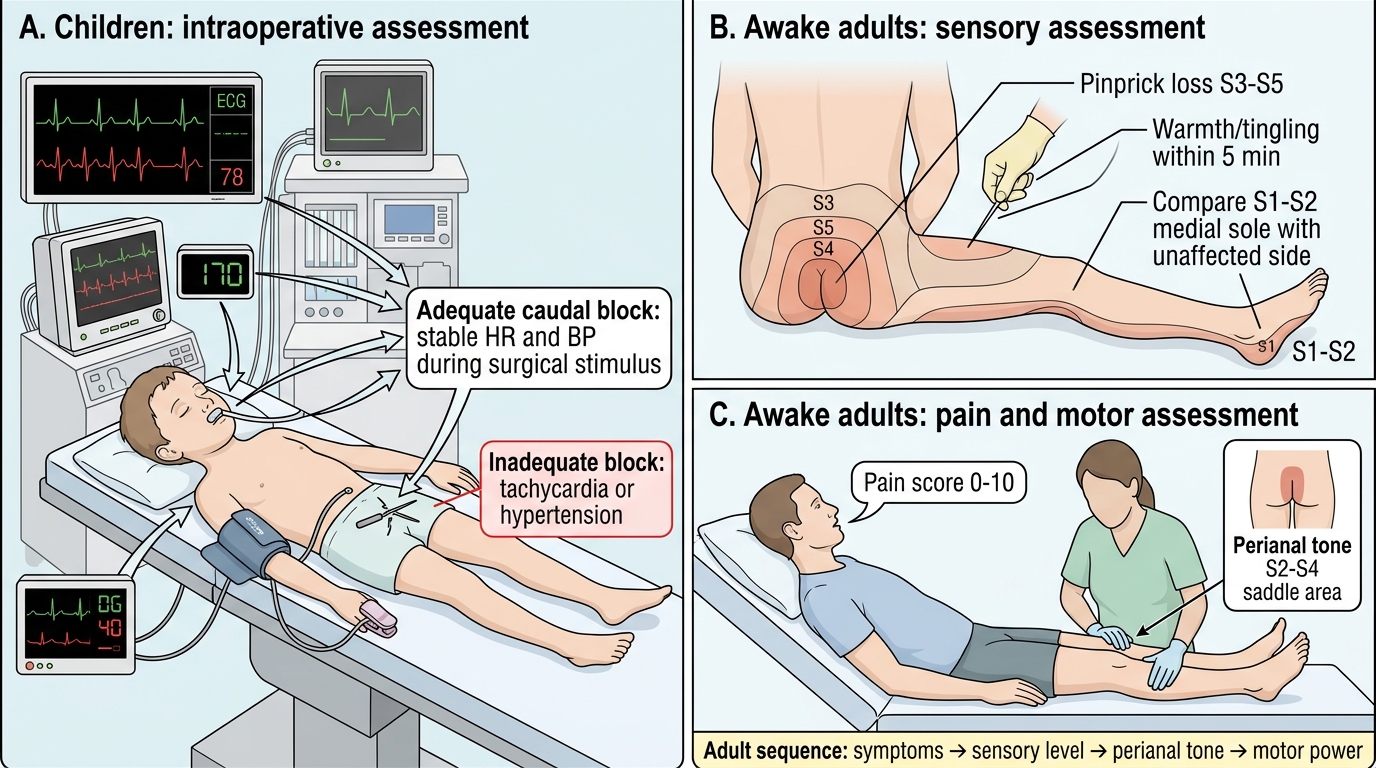
Assessment of Caudal Block in Children and Adults
In awake adults: Assessment follows the standard neuraxial sequence: (1) warmth and tingling in the sacral dermatomes (perianal region, posterior thigh) within 5 minutes; (2) loss of pinprick sensation in S3–S5 distribution (perineum, posterior thigh) within 10–15 minutes; (3) loss of perianal tone (S2–S4 — the "saddle area"). The block level can be verified by testing the S1–S2 dermatome on the medial sole of the foot and comparing with the unaffected side. For adult patients undergoing caudal steroid injection for coccydynia, relief of pain with the injection (diagnostic component) is itself an indicator of correct placement.
Detecting complications: The key early complications are intravascular injection (tachycardia from the adrenaline test dose, followed by LAST symptoms if injection continues), dural puncture (CSF aspiration; produces a total spinal if the full epidural dose is injected), and subcutaneous injection (swelling and oedema over the sacrum without any block — the injection has gone superficial to the sacrococcygeal membrane). Subcutaneous injection is the most common failure mode, especially in obese adults. If the block fails and a sacral swelling appears, do not re-attempt immediately: a subcutaneous bolus raises total body LA levels and narrows the safe retreatment window.
SELF-CHECK
During a paediatric caudal block in a 6-month-old infant, aspiration yields no blood or CSF. The anaesthetist injects 0.5 mL/kg of 0.25% bupivacaine and notices a swelling appearing over the sacrum. What has occurred and what should be done?
A. The block has been placed correctly; sacral swelling is normal as the LA distends the epidural space
B. Subcutaneous injection has occurred — the needle was superficial to the sacrococcygeal membrane; do not re-inject immediately as LA levels are now elevated
C. Intravascular injection has occurred — the swelling is from haematoma; give 20% intralipid
D. The dural sac has been punctured — the CSF is leaking under pressure into the sacral tissues
Reveal Answer
Answer: B. Subcutaneous injection has occurred — the needle was superficial to the sacrococcygeal membrane; do not re-inject immediately as LA levels are now elevated
A visible swelling over the sacrum immediately during or after injection is the classic sign of subcutaneous injection — the needle has failed to penetrate the sacrococcygeal membrane and the LA is depositing in the subcutaneous tissue. No epidural space entry has occurred, so no block will develop. The critical safety implication: the body has absorbed a dose of LA subcutaneously, which has a slower but non-negligible absorption profile. Re-attempting immediately would risk cumulative dosing approaching or exceeding the maximum safe dose (2 mg/kg bupivacaine). The anaesthetist must calculate the residual allowable dose before any retreatment — or wait and manage pain with systemic analgesia if the total dose absorbed is close to the maximum.
Applied and Supervised Practice: Observing Caudal Block
Competency AS5.5 specifies "observe and describe" — meaning that by the end of your clinical exposure to caudal blocks, you should be able to narrate what you observed in enough clinical and anatomical detail to demonstrate genuine understanding. This section provides a structured framework for active observation.
Before entering the theatre: Review the anatomy one more time — draw the equilateral triangle formed by the two posterior superior iliac spines and the sacral hiatus on paper, estimate where the sacral cornua would be palpable, and recall the Armitage formula for the intended block level. Review the planned LA, its concentration, and calculate the mg/kg dose for the patient's weight before the anaesthetist does — compare your calculation with theirs.
During the block: Observe the patient's positioning (lateral vs prone — why was this chosen?). Watch the anaesthetist's palpation technique — can you see them identifying the cornua? Watch the needle entry angle (approximately 45°) and the change in angle (flattened to 20° after membrane penetration). Listen for whether they describe a "pop" or loss of resistance. Observe the confirmation manoeuvre (aspiration, test dose, or ultrasound). Watch the injection — is it smooth and low-resistance, or does the anaesthetist meet resistance (which would indicate incorrect placement or blocked needle)? Note the total volume and time to injection completion.
After the block: In children — observe the intraoperative haemodynamic trace; compare heart rate and blood pressure during incision and dissection to the pre-incision baseline. In the recovery room, observe whether the child is calm or crying; note whether motor block in the legs is present and how long it persists. In adults — participate in sensory testing (with permission and supervision): test temperature and pinprick in the perineal and posterior thigh dermatomes; document the block level.
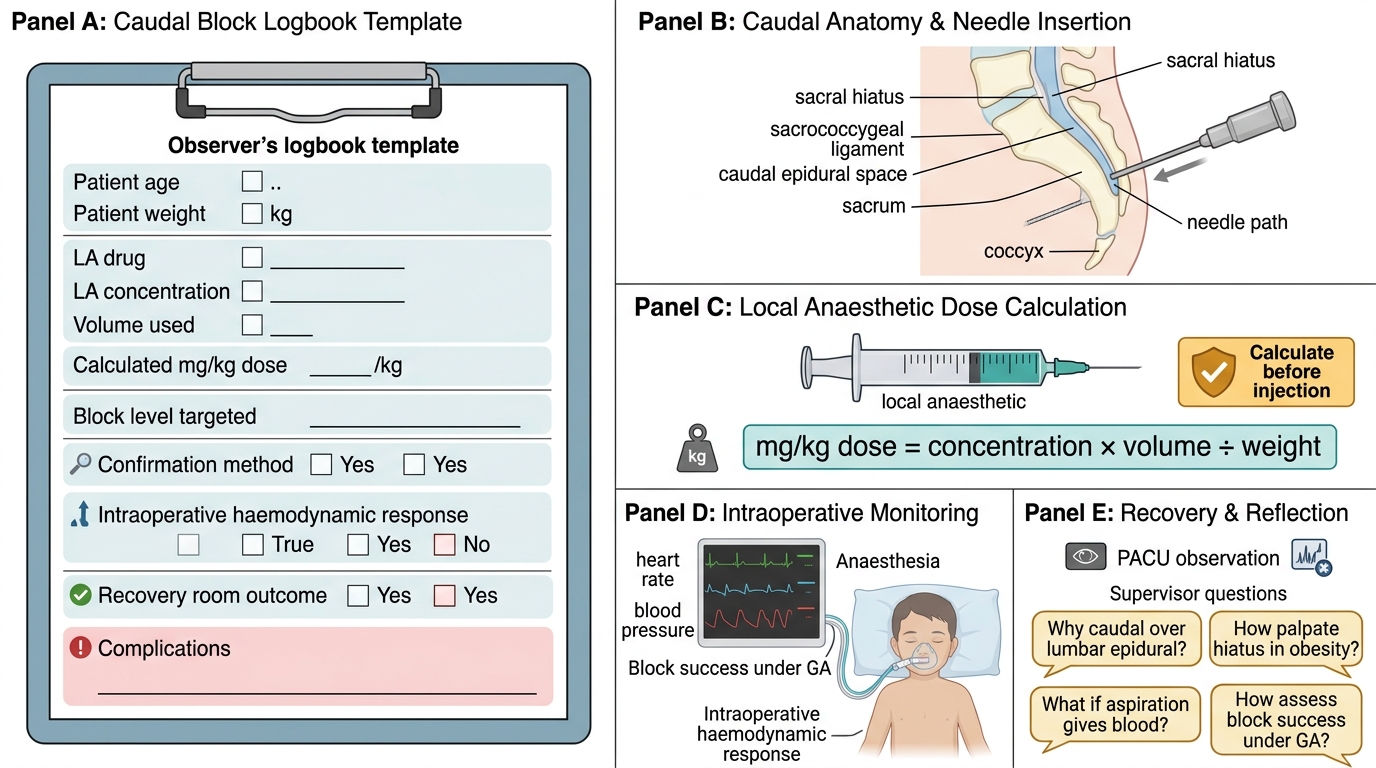
Observer Logbook for Caudal Block
Key questions to ask your supervising anaesthetist: Why did you choose caudal over a lumbar epidural for this patient? How do you palpate the hiatus in an obese patient? What would you do if aspiration gave a flash of blood? How do you assess block success in a child under GA? These questions demonstrate engaged observation and accelerate clinical learning beyond what passive watching achieves.