Page 1 of 17
AS5.1-2 | Principles, Indications and Anatomy for Regional Anaesthesia — SDL Guide
CLINICAL SCENARIO
A 68-year-old patient with severe COPD and ischaemic heart disease is listed for a total knee replacement. General anaesthesia with a supraglottic airway carries real risk: difficult extubation, postoperative respiratory failure, and prolonged ICU stay. The anaesthetist instead selects a subarachnoid block. Forty minutes later, the patient is awake, pain-free, breathing room air, and her knee is being replaced. She will eat lunch the same afternoon. This is the power of regional anaesthesia — precision analgesia and motor block delivered exactly where surgery occurs, with the rest of the body left undisturbed. For a generation of anaesthesiologists, mastering regional techniques is not optional; it is central to safe, patient-centred perioperative care.
WHY THIS MATTERS
Regional anaesthesia is an entire philosophical approach to surgical care, not merely a technique. It reduces systemic drug exposure, blunts the stress response, shortens recovery times, and enables day-care surgery for patients who once required inpatient admission. In India, where ischaemic heart disease, COPD, and diabetes are epidemic, regional techniques allow surgical access to populations previously considered too high risk for general anaesthesia. Understanding the principles, indications, contraindications, and relevant anatomy covered in this SDL (AS5.1, AS5.2) is the obligatory foundation before you observe or perform any block — spinal, epidural, combined, or peripheral.
RECALL
Before proceeding, refresh the following:
- Somatic and autonomic nervous system anatomy: the relationship between sensory dermatomes, motor myotomes, and sympathetic outflow levels.
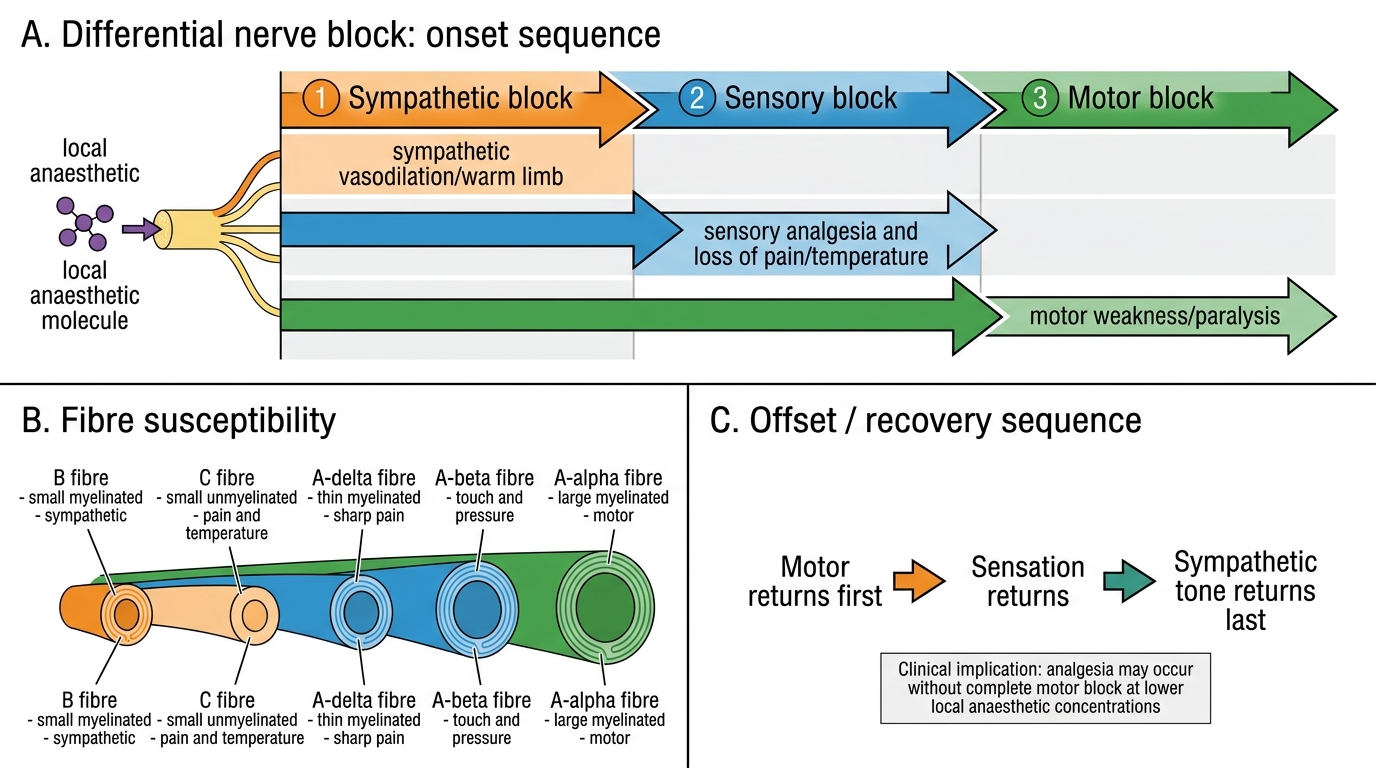
- Pharmacology of local anaesthetics (LAs): mechanism of sodium-channel blockade, differential block (autonomic > sensory > motor sequence of onset), and the importance of pKa in speed of onset.
- Vasovagal physiology: why sudden hypotension and bradycardia occur together when sympathetic tone is abruptly removed.
- Lumbar spine anatomy: interspinous spaces, ligaments (supraspinous, interspinous, ligamentum flavum), epidural space, dura, and subarachnoid space with cerebrospinal fluid.
Principles of Regional Anaesthesia
Regional anaesthesia (RA) is the reversible interruption of nerve conduction in a defined anatomical region, achieved by depositing a local anaesthetic (LA) solution near a nerve or nerve plexus, within the epidural space, or within the subarachnoid space. The fundamental principle is selectivity — only the nerves targeted by the LA are blocked, leaving the rest of the neuraxis and the airway reflexes intact. This distinguishes RA from general anaesthesia (GA) in its risk profile, recovery characteristics, and suitability for high-risk patients.
Differential nerve block is a core physiological concept. Sympathetic fibres (B-fibres, smallest, unmyelinated) are blocked first, producing vasodilation and warmth. Sensory fibres (A-delta for sharp/cold, C-fibres for dull pain) are blocked next. Large myelinated motor fibres (A-alpha) are blocked last and recover first. This gradient explains the clinical sequence: the patient feels warmth and tingling before losing sensation, and sensation recovers before full motor strength returns.
The density and duration of block are governed by the specific LA used, its concentration, the volume deposited, and additives such as opioids or adrenaline. Adrenaline (epinephrine) prolongs block duration by causing local vasoconstriction that slows LA absorption into the bloodstream. This also raises the safe maximum dose for infiltration techniques.
Differential Nerve Block in Regional Anaesthesia
Classification of regional techniques:
- Neuraxial blocks: subarachnoid (spinal) block, epidural block (lumbar, thoracic, caudal), combined spinal-epidural (CSE).
- Peripheral nerve blocks (PNBs): brachial plexus (interscalene, supraclavicular, infraclavicular, axillary), femoral, sciatic, popliteal, ankle block, and many others.
- Field blocks and infiltration: surgical site infiltration, wound infiltration, tumescent techniques.
The choice among these is guided by the surgical site, duration of surgery, need for postoperative analgesia, and patient factors.
Indications for Regional Anaesthesia
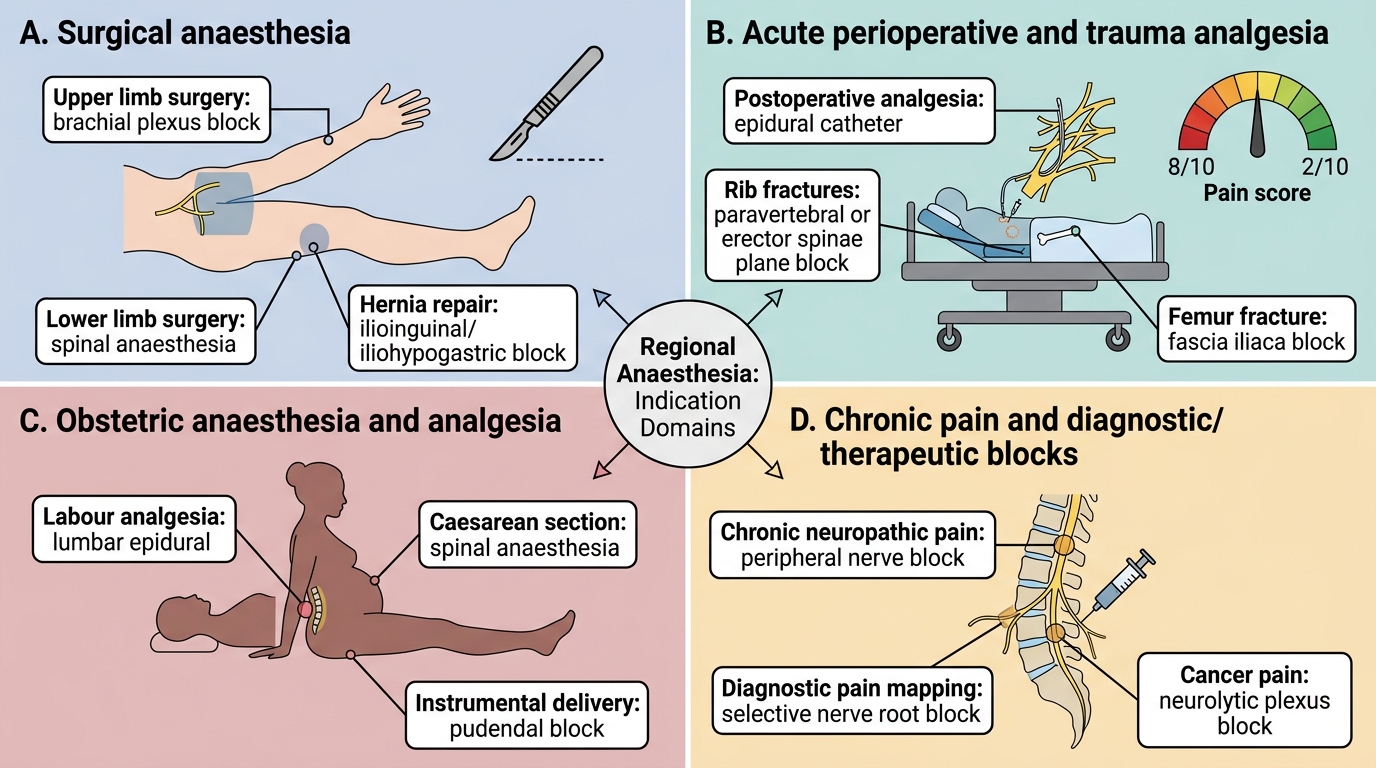
The indications for RA span four broad domains, reflecting its versatility as both a primary anaesthetic and an analgesic adjunct.
1. Surgery as the sole anaesthetic technique: RA is preferred for lower-limb orthopaedic surgery (knee arthroplasty, hip fracture repair, ankle surgery), lower abdominal surgery (caesarean section, inguinal hernia repair, transurethral resection of the prostate), and upper-limb surgery (hand, forearm, shoulder — via brachial plexus blocks). The patient remains awake or lightly sedated, allowing immediate feedback and reducing airway risks.
2. High-risk patients for whom GA carries disproportionate risk: elderly patients with multiple comorbidities, patients with severe COPD or OSA, those with anticipated difficult airways, patients with full stomachs (aspiration risk), morbidly obese patients. RA can circumvent the need for tracheal intubation entirely.
3. Postoperative pain management (as adjunct to GA): thoracic epidurals for major abdominal and thoracic surgery dramatically reduce opioid requirements and improve respiratory outcomes. Peripheral nerve catheters (e.g., femoral nerve catheter post-TKR) enable early physiotherapy and discharge.
4. Labour analgesia: epidural analgesia during labour is the gold standard for maternal pain relief, allowing conversion to surgical block for emergency caesarean section without a second anaesthetic.
Indication Domains of Regional Anaesthesia
Contraindications are either absolute or relative. Absolute contraindications include patient refusal, bleeding diathesis or therapeutic anticoagulation (for neuraxial blocks — check ASRA guidelines for specific drug-specific intervals), infection at the proposed needle-insertion site, and raised intracranial pressure (for subarachnoid block — lumbar puncture risks brainstem herniation). Relative contraindications include systemic sepsis, hypovolaemia (because sympathectomy will worsen hypotension), pre-existing neurological deficit (medico-legal risk), and uncooperative or confused patients.
Correlative Anatomy: The Subarachnoid and Epidural Spaces
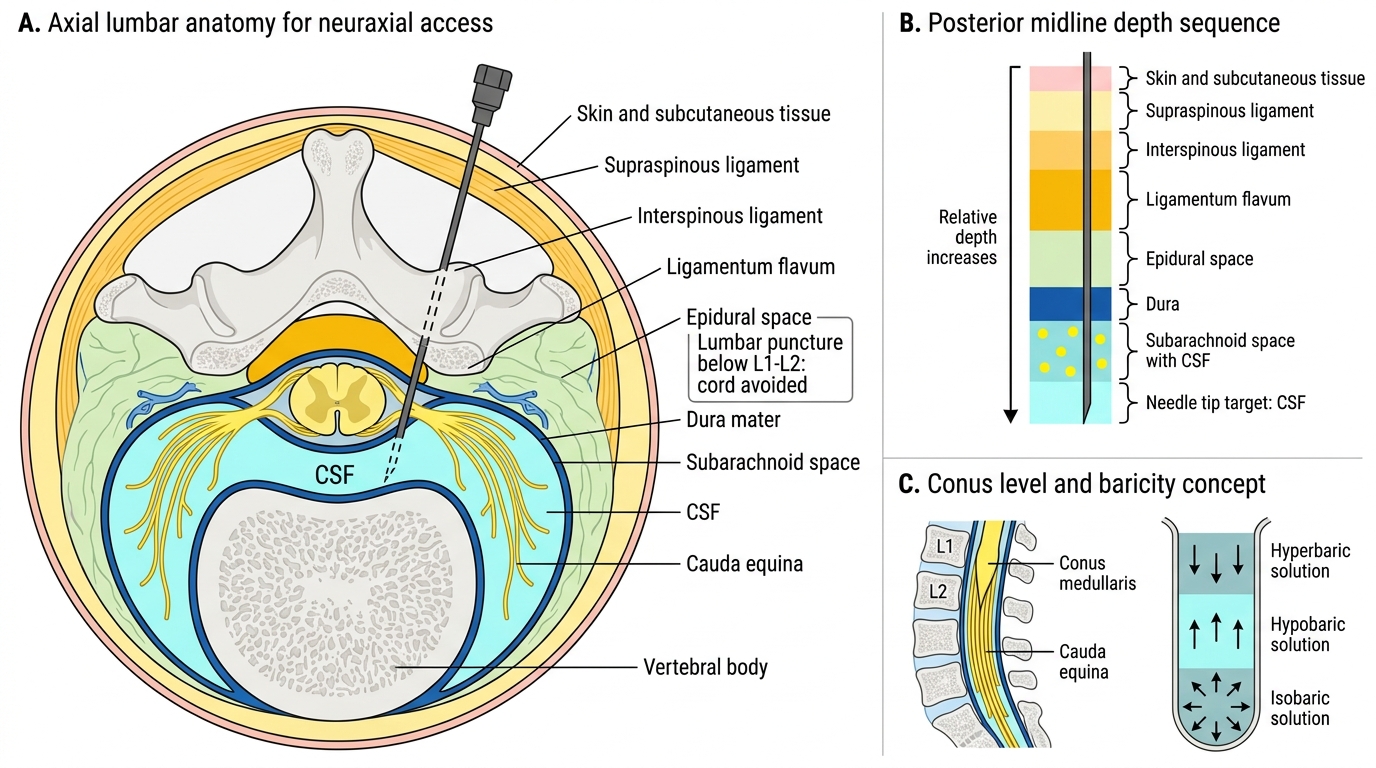
A precise anatomical understanding of the layers traversed by a spinal or epidural needle is essential for safe technique. Moving from skin inward in the lumbar region, the needle passes through skin, subcutaneous fat, supraspinous ligament, interspinous ligament, ligamentum flavum, and then into the epidural space — a potential space containing epidural fat, the epidural venous plexus, and lymphatics. Beyond the epidural space lies the dura mater, then the subdural space (a potential space of no clinical relevance for intended blocks), then the arachnoid mater, and finally the subarachnoid space filled with cerebrospinal fluid (CSF).
The epidural space extends from the foramen magnum to the sacral hiatus. Its depth from skin is approximately 4–6 cm in most adults but varies greatly with obesity and anatomy. It communicates laterally with the paravertebral space through the intervertebral foramina, which is why epidural LAs can produce bilateral block and paravertebral blocks can produce unilateral spread. The ligamentum flavum is the landmark for loss-of-resistance (LOR) technique: its dense elastin-rich texture resists the syringe plunger, and entry into the epidural space is signalled by sudden LOR as this resistance disappears.
Lumbar Neuraxial Anatomy and CSF Space
The subarachnoid space contains the cauda equina below L1 in adults (the spinal cord ends at L1–L2, so lumbar puncture below this level avoids cord injury). CSF is continuously produced by the choroid plexus at approximately 0.35 mL/min and has a total volume of about 120–150 mL. The specific gravity of CSF (1.003–1.008) is central to the concept of baricity — the relative density of the LA solution compared to CSF — which determines the direction of spread of a spinal block.
Baricity and posture: hyperbaric solutions (heavier than CSF — typically prepared with glucose) sink with gravity, so sitting a patient upright after injection produces a perineal/saddle block, while the supine Trendelenburg position drives the block cephalad. Hypobaric solutions (lighter than CSF) do the opposite. Isobaric solutions are largely posture-independent, spreading uniformly. Anaesthesiologists must account for baricity when choosing the LA preparation and patient position for spinal anaesthesia.