Page 3 of 17
AS5.1-2 | Principles, Indications and Anatomy for Regional Anaesthesia — SDL Guide (Part 3)
Comparing Spinal and Epidural Anaesthesia
The distinction between spinal (subarachnoid) block and epidural block is one of the most commonly tested concepts in anaesthesia and one of the most clinically consequential. Getting them confused is a dangerous error.
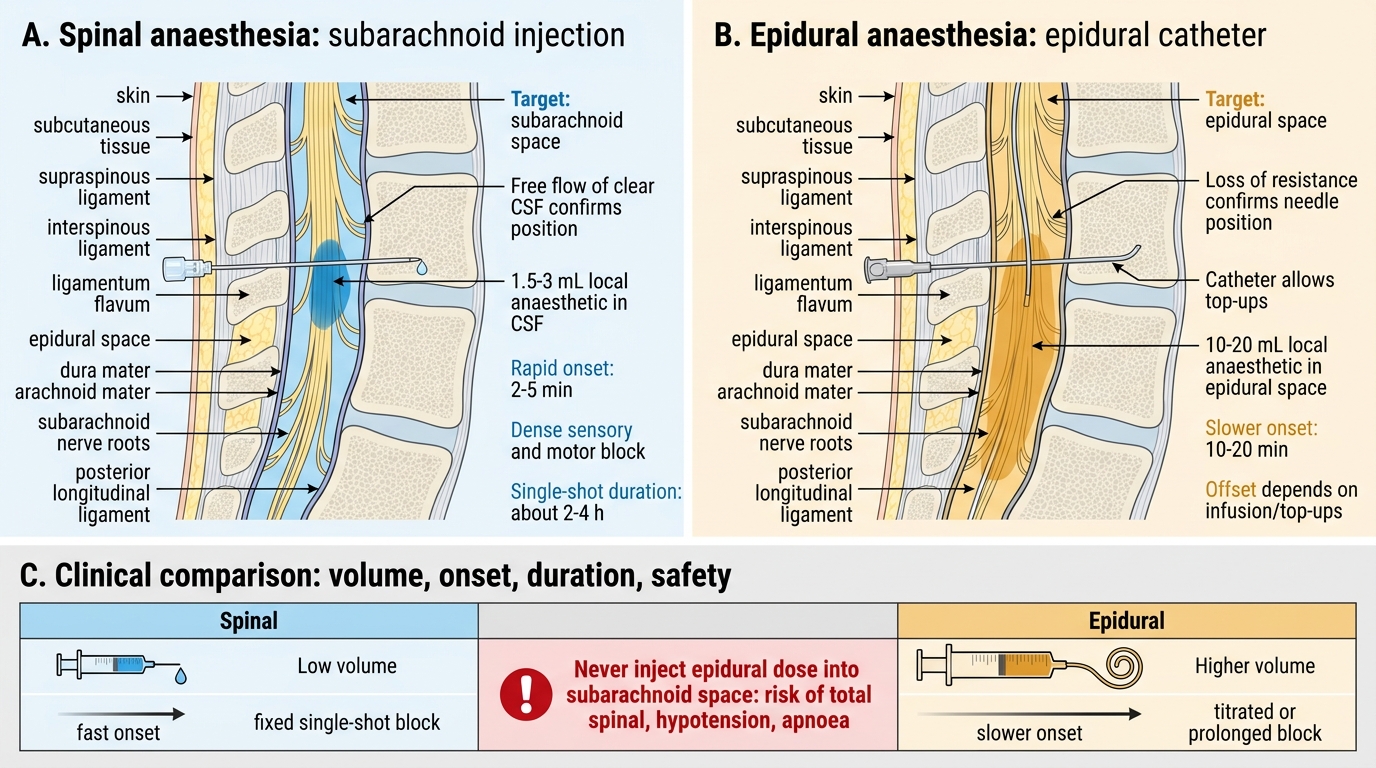
Subarachnoid (spinal) block involves injection of a small volume of LA directly into the cerebrospinal fluid within the subarachnoid space. The drug acts directly on the nerve roots as they traverse the CSF. Characteristics: small dose (e.g., 2–3 mL hyperbaric bupivacaine 0.5%), rapid onset (2–5 minutes to full block), dense, reliable block (complete motor and sensory block for most patients), single-shot (no catheter in standard technique), and limited duration (typically 2–3 hours for bupivacaine). The risks specific to spinal anaesthesia include post-dural puncture headache (PDPH) (from CSF leakage through the dural hole, causing traction on meningeal structures when upright), hypotension (from sympathectomy — the most common side effect, managed with fluids and vasopressors), total spinal (unintended cephalad spread to the brainstem), and cauda equina syndrome (rare, associated with repeated injections of hyperbaric lignocaine — now avoided).
Epidural block involves injection into the epidural space — NOT into the CSF. A catheter is typically placed, enabling titratable, continuous anaesthesia and analgesia. Characteristics: larger volume (10–20 mL to achieve a similar block level as spinal — because the drug must diffuse through the dura), slower onset (15–20 minutes), less dense motor block (making epidural preferred for labour analgesia, where maternal pushing ability is preserved), catheter allows top-ups or infusion for prolonged surgery or postoperative analgesia, and ability to extend for surgical anaesthesia (e.g., augmenting labour epidural for caesarean section). Risks specific to epidural include: accidental dural puncture (ADP) causing severe PDPH, epidural haematoma or abscess (rarer but more serious than for spinal), unilateral block (catheter tip malposition), and epidural catheter migration into a blood vessel (intravascular injection) or subarachnoid space (total spinal).
Spinal vs Epidural Anaesthesia
Combined Spinal-Epidural (CSE) combines the advantages of both: the reliable, rapid-onset density of spinal for surgical anaesthesia with the catheter for top-ups and postoperative analgesia. It is particularly valued for long orthopaedic cases, caesarean section, and major lower-limb surgery.
CLINICAL PEARL
The "single most dangerous swap" in regional anaesthesia: Never confuse the subarachnoid space with the epidural space. The dose of LA intended for the epidural space (e.g., 15 mL of 0.5% bupivacaine = 75 mg) injected into the subarachnoid space will produce a total spinal — immediate cardiovascular collapse and apnoea. This error has caused deaths. Before any neuraxial injection, confirm needle position by: for spinal — free flow of clear CSF through the needle hub; for epidural — loss of resistance to saline/air with a Tuohy needle, then aspiration through catheter (blood → vessel; clear fluid flowing freely → possible inadvertent dural puncture; nothing → correct epidural position). The rule: if in doubt, use a test dose (3 mL of LA with 15 mcg adrenaline — intravascular injection causes a tachycardia of ≥20 bpm within 45–60 seconds; subarachnoid injection causes rapid dense motor block in the legs).
Management of Hypotension During Neuraxial Block
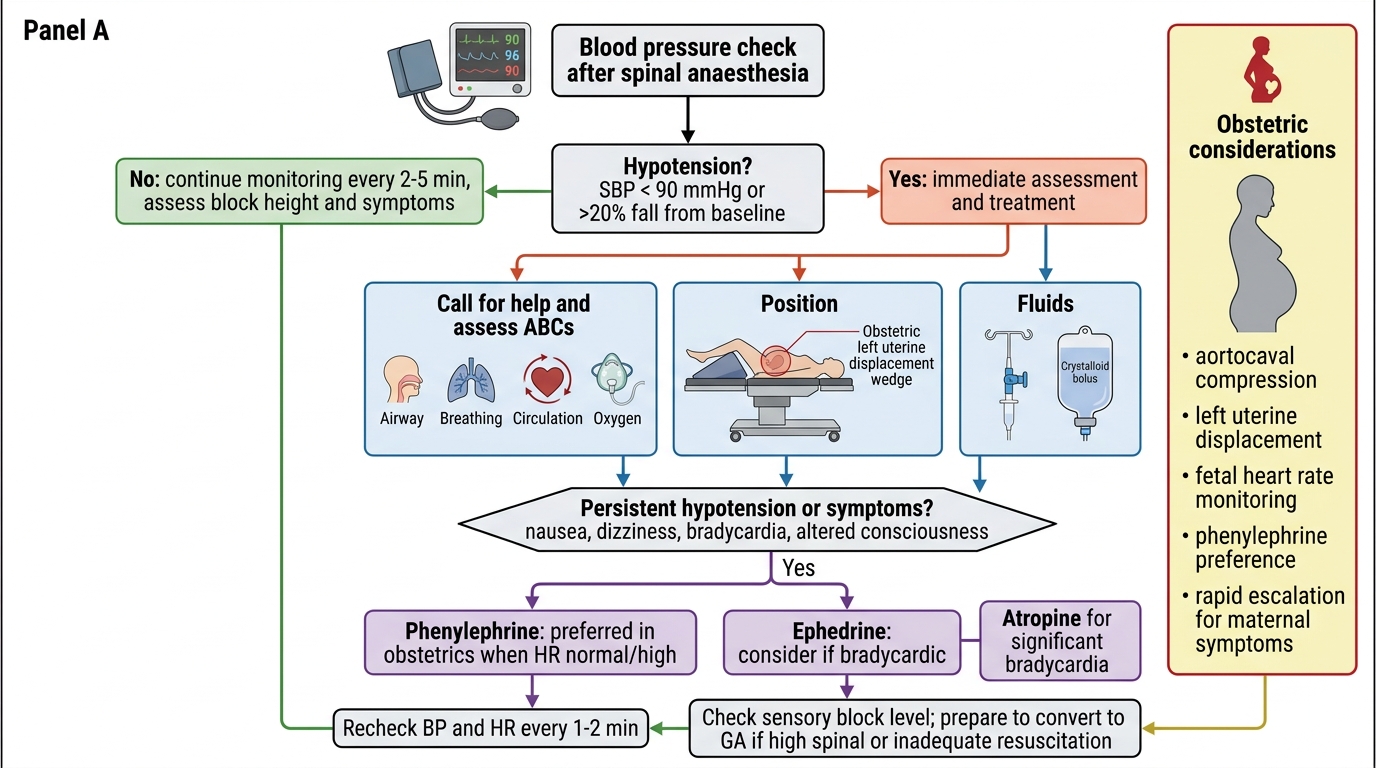
Sympathectomy-induced hypotension is the most frequent complication of neuraxial anaesthesia, occurring in up to 30% of spinal blocks for caesarean section and 20–25% for other procedures. The pathophysiology involves blockade of sympathetic vasoconstrictor fibres (which run in the preganglionic chain from T1–L2), causing arterial and venous dilation. Venous pooling in the lower limbs dramatically reduces venous return, with a resultant fall in cardiac output and blood pressure. In obstetric patients, aortocaval compression by the gravid uterus compounds the hypotension — which is why left lateral tilt is mandatory in all pregnant patients undergoing neuraxial block.
Prevention strategies: coloading (infusion of crystalloid at the time of block, not pre-loading which is washed out rapidly), phenylephrine infusion (first-line vasopressor in obstetrics as it preserves uteroplacental blood flow better than ephedrine in most studies), adequate IV access before block, and having emergency drugs drawn up and ready.
Treatment: position (head down, legs up to increase venous return), IV fluid bolus, and vasopressors. Ephedrine (alpha + beta agonist, 6–12 mg IV boluses) was traditionally first-line; phenylephrine (pure alpha agonist, 50–100 mcg IV boluses) is now preferred in caesarean section as it reduces the risk of fetal acidosis. Severe bradycardia (common with high block affecting cardiac accelerator fibres T1–T4) is treated with atropine 0.6 mg IV or epinephrine for profound bradycardia with cardiovascular collapse (Bezold-Jarisch reflex).
Management of Hypotension During Spinal Anaesthesia
Self-Assessment: Integrating Regional Anaesthesia Knowledge
At the conclusion of this learning unit, you should be able to apply the foundational concepts of regional anaesthesia to clinical decision-making. The self-assessment step does not merely mean answering questions — it means being able to reason through clinical scenarios using the principles and anatomy covered in this SDL, identifying gaps in your understanding, and seeking sources (Morgan & Mikhail, Ajay Yadav's Regional Anaesthesia, the ASRA guidelines) to resolve them.
Test yourself on these integration questions: Can you trace a neuraxial needle from skin to subarachnoid space, naming every layer? Can you recall the maximum dose of bupivacaine without prompting — and know why exceeding it is potentially fatal? Can you describe the brachial plexus from roots to terminal branches, and name which block approach targets which level? Do you understand why the anaesthetist's job does not end at block placement — monitoring of block level, haemodynamic response, patient comfort, and readiness to convert to GA are ongoing responsibilities?
Reflect on the distinction between spinal and epidural that was emphasised in this SDL. If a registrar beside you confused the two and was about to inject 15 mL of 0.5% bupivacaine into what they believed was the epidural space but was actually the subarachnoid space, would you recognise the error before the injection was complete? What signs would alert you? The answer — free-flowing clear CSF through the catheter under aspiration, or an unexpectedly small initial bolus producing bilateral dense block within 2 minutes — reflects the vigilance that regional anaesthesia demands of every practitioner.
SELF-CHECK
Which of the following is a CONTRAINDICATION to the use of adrenaline as an additive to local anaesthetic for a peripheral nerve block?
A. Patient has well-controlled hypertension on an ACE inhibitor
B. Block site is a digital nerve at the base of the finger
C. Patient has mild anxiety about the procedure
D. The anaesthetist wishes to prolong block duration
Reveal Answer
Answer: B. Block site is a digital nerve at the base of the finger
Adrenaline-containing solutions are absolutely contraindicated for digital nerve blocks, penile blocks, and any block in an end-arterial territory. Adrenaline causes intense vasoconstriction; in the digit (an end-artery with no collateral circulation), this can cause ischaemia, gangrene, and digit loss. In contrast, well-controlled hypertension and patient anxiety are not contraindications to the use of adrenaline in nerve blocks (in a proper anatomical site). The anaesthetist who prolongs block duration with adrenaline must do so in sites with adequate collateral circulation.