Page 5 of 11
AS9.3-4 | Perioperative Fluid Therapy and Blood Product Use — SDL Guide (Part 2)
Blood Products: Components, Indications, and Administration
Blood component therapy is the administration of specific fractions of donated whole blood — each processed, stored, and prescribed separately — to replace only the deficit component in a patient. This component approach maximises efficient use of donated blood and minimises transfusion-related adverse effects from unnecessary components. The four main blood products used perioperatively are packed red blood cells (PRBCs), fresh frozen plasma (FFP), platelets, and cryoprecipitate. Each has precise indications, a specific storage temperature and shelf life, a recommended dose, and a distinct adverse-effect profile. The shift from whole-blood transfusion to component therapy over the past four decades has been one of the most significant advances in transfusion medicine: it allows one donated unit to benefit up to four patients, it enables targeted correction of specific deficits, and it reduces the risk of volume overload and unnecessary antigen exposure. Knowing the properties of each component in detail — not just the name — is what enables rational, evidence-based prescribing in the perioperative setting.
Packed red blood cells (PRBCs):
- Content: concentrated red cells suspended in additive solution; haematocrit ~55–70%; one unit raises Hb by approximately 1 g/dL in a 70 kg adult.
- Storage: 2–6°C, shelf life 35–42 days (citrate-phosphate-dextrose-adenine [CPDA] or SAG-M additive).
- Indications: Hb <7 g/dL in haemodynamically stable patients (restrictive transfusion threshold, TRICC trial); Hb <8 g/dL in patients with known ischaemic heart disease or poor cardiopulmonary reserve; acute haemorrhage causing haemodynamic instability regardless of Hb level. The maximum allowable blood loss (MABL) calculation (see arc step 3) guides the trigger point.
- Administration: through a blood administration set (170–200 µm filter); must be ABO and Rh compatible; each unit over 1–2 hours (faster if haemodynamically unstable); must be completed within 4 hours of issue.
Fresh frozen plasma (FFP):
- Content: all clotting factors including labile V and VIII, and fibrinogen; separated from whole blood and frozen within 8 hours of donation. One unit = ~250 mL.
- Storage: −25°C, shelf life 12 months; thawed at 37°C and must be transfused within 24 hours of thawing.
- Indications: (1) active bleeding with documented coagulopathy (PT or APTT >1.5 × normal); (2) massive transfusion protocol — typically FFP:PRBC ratio 1:1 or 1:2 in damage-control resuscitation; (3) reversal of warfarin in life-threatening haemorrhage (combined with Vitamin K and prothrombin complex concentrate); (4) rare single-factor deficiencies where specific concentrate is unavailable. NOT indicated for routine preoperative coagulopathy correction without bleeding, nor as a volume expander.
- Dose: 10–15 mL/kg (typically 2–4 units in adults).
Platelets:
- Content: platelet concentrate from whole blood (one unit = ~50 mL) or apheresis (one unit = therapeutic dose equivalent to 4–6 whole-blood-derived units). Each unit raises platelet count by approximately 20,000–30,000/µL.
- Storage: 20–24°C with continuous agitation, shelf life 5 days (highest infection risk of all blood products).
- Indications: (1) platelet count <50,000/µL with active surgical bleeding; (2) <100,000/µL in neurosurgical or ophthalmic procedures; (3) platelet count <10,000/µL prophylactically (severe thrombocytopaenia); (4) platelet dysfunction (uraemia, post-aspirin) with ongoing haemorrhage regardless of count.
- Administration: ABO compatible preferred; transfuse rapidly (over 30 minutes); never administer through a giving set with a standard 170 µm filter (use a platelet/blood administration set).
Cryoprecipitate:
- Content: concentrated preparation of fibrinogen (150–300 mg/unit), Factor VIII, von Willebrand factor, Factor XIII, and fibronectin; derived by slow thawing of FFP. One pool = 5 units combined.
- Storage: −25°C, shelf life 12 months; once thawed, transfuse within 4 hours.
- Indications: (1) fibrinogen deficiency (plasma fibrinogen <1.5 g/L) with active bleeding — fibrinogen is the first clotting factor to become critically low in massive haemorrhage; (2) haemophilia A (Factor VIII deficiency) when specific concentrate unavailable; (3) von Willebrand disease (when DDAVP is insufficient); (4) Factor XIII deficiency.
- Dose: 1 pool (5 units) typically raises fibrinogen by 0.5–1 g/L.
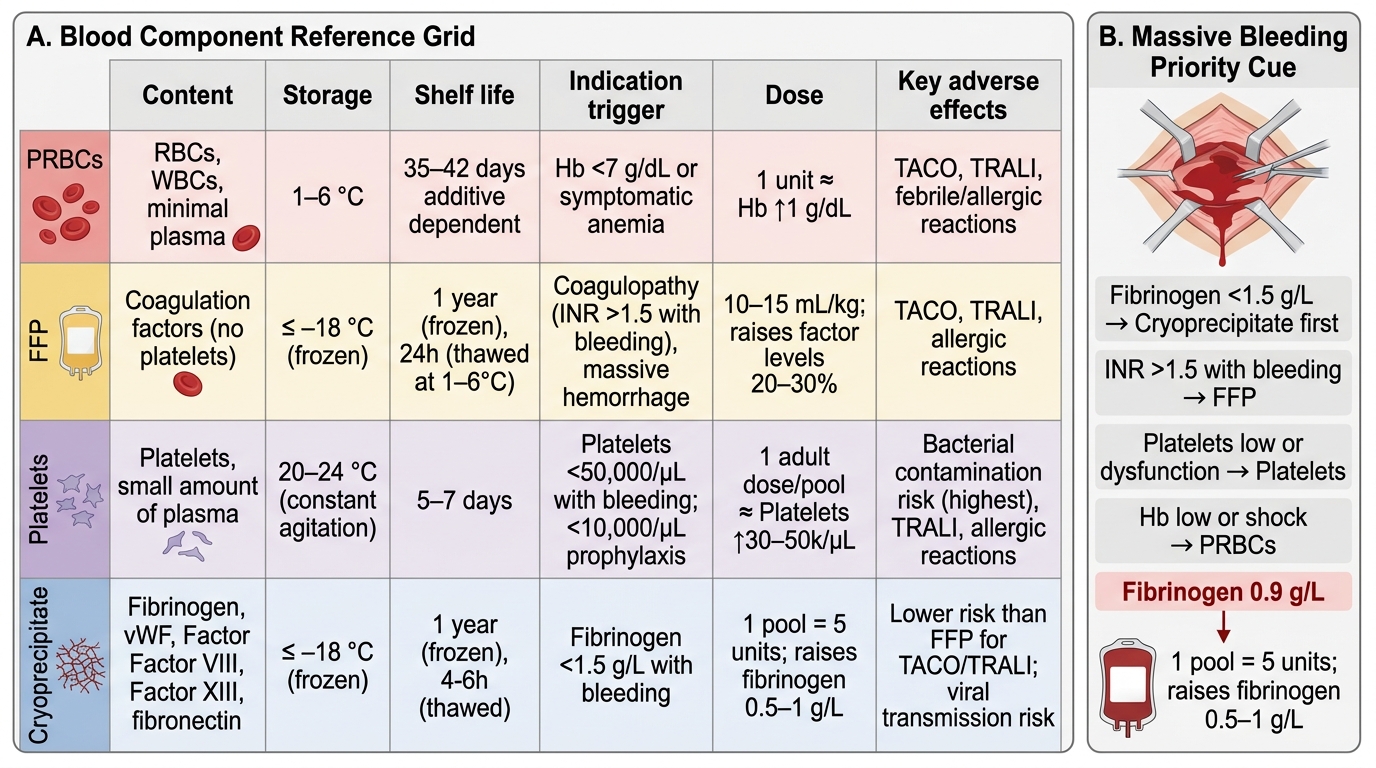
Blood Components Reference Grid
SELF-CHECK
A 65-year-old man undergoing an open aortic aneurysm repair has received 8 units of PRBCs over 90 minutes. His INR is now 2.8 and his fibrinogen level is 0.9 g/L. He continues to bleed from the anastomotic line. Which blood product should be prioritised NEXT?
A. Cryoprecipitate — to correct the critically low fibrinogen
B. FFP — to correct the elevated INR
C. Platelets — because platelet count is likely low in massive transfusion
D. Another 4 units of PRBCs — the haemoglobin is the primary concern
Reveal Answer
Answer: A. Cryoprecipitate — to correct the critically low fibrinogen
Fibrinogen is the first clotting factor to become critically depleted in massive haemorrhage and dilutional coagulopathy. A fibrinogen level of 0.9 g/L (critically low; threshold for action is <1.5 g/L) is the most immediately correctable coagulopathy and the principal driver of ongoing surgical bleeding in this context. Cryoprecipitate (1 pool = 5 units) will rapidly raise fibrinogen by 0.5–1 g/L. While FFP should also be given (INR >1.5 with active bleeding is an indication), fibrinogen replacement takes precedence because cryoprecipitate's concentrated fibrinogen corrects the most rate-limiting coagulation failure. Platelets and further PRBCs should be assessed after fibrinogen is corrected.
Clinical and Applied Significance: Adverse Effects and Safe Transfusion Practice
Administering blood products carries clinically significant risks that every anaesthesiologist must recognise, anticipate, and manage. Transfusion medicine is a discipline that rewards vigilance: the majority of serious transfusion reactions are preventable with correct patient identification, compatibility checking, and bedside monitoring. Understanding the mechanism behind each adverse effect also guides rational selection of blood products — minimising unnecessary exposure is itself a patient safety intervention. Transfusion reactions are classified by their timing (acute: during or within 24 hours; delayed: more than 24 hours post-transfusion) and their mechanism (immunological: caused by antibody-antigen reactions; non-immunological: caused by the physical or chemical properties of stored blood or volume overload). In the operating theatre, the anaesthetised patient cannot report symptoms such as back pain, chest tightness, or urticaria — meaning the anaesthesiologist must maintain a heightened index of suspicion and actively monitor vital signs throughout every transfusion. An unexplained fall in blood pressure, a rise in temperature, or haemoglobinuria in a ventilated patient must prompt immediate assessment for a transfusion reaction, even when the clinical picture could be attributed to surgical causes.
Acute transfusion reactions (occurring during or within 24 hours of transfusion):
- Acute haemolytic transfusion reaction (AHTR): the most immediately life-threatening reaction; caused by ABO-incompatible transfusion (usually clerical error). Mechanism: pre-formed IgM antibodies activate complement, causing intravascular haemolysis → free haemoglobin release → renal tubular obstruction, disseminated intravascular coagulation (DIC), hypotension, and shock. Features in the anaesthetised patient: unexplained hypotension, haemoglobinuria (dark red urine), generalised bleeding (DIC), fever. Action: stop transfusion immediately, check identity and blood unit labels, maintain urine output with IV fluids and mannitol, treat DIC.
- Febrile non-haemolytic transfusion reaction (FNHTR): most common reaction; caused by recipient antibodies against donor leukocyte antigens or cytokines in stored blood. Fever, rigors, headache — usually self-limiting. Treated with antipyretics; transfusion may continue cautiously.
- Allergic / anaphylactic reaction: IgE-mediated hypersensitivity to donor plasma proteins. Urticaria (mild) to bronchospasm and cardiovascular collapse (anaphylaxis). Treat with antihistamines, corticosteroids, and adrenaline as per severity.
- Transfusion-related acute lung injury (TRALI): the leading cause of transfusion-related mortality. Occurs within 6 hours of FFP, platelets, or whole blood administration. Mechanism: donor anti-HLA or anti-neutrophil antibodies activate recipient neutrophils in pulmonary vasculature → non-cardiogenic pulmonary oedema. Features: acute hypoxia, bilateral infiltrates on CXR, normal PAWP. Treatment: supportive (oxygen, ventilation); no diuretics.
- Transfusion-associated circulatory overload (TACO): hydrostatic pulmonary oedema from fluid overload; distinguished from TRALI by high PAWP, BNP elevation, and response to diuretics.
Delayed transfusion reactions (>24 hours):
- Delayed haemolytic transfusion reaction: due to anamnestic antibody response to minor blood group antigens (Kidd, Duffy, Kell); Hb drops 5–10 days post-transfusion; usually mild.
- Post-transfusion purpura: rare immune destruction of patient's own platelets ~10 days post-transfusion.
- Transfusion-transmitted infections: HIV, HCV, HBV — risk now very low with nucleic acid testing; malaria, CMV, and variant CJD remain concerns in specific populations.
- Iron overload: in chronically transfused patients (haemoglobinopathies, MDS); managed with chelation therapy.
Safe transfusion checklist (mandatory steps before every unit):
1. Confirm patient identity against the blood unit label at the bedside (two identifiers).
2. Check ABO and Rh compatibility on the label.
3. Check expiry date and inspect for haemolysis or discolouration.
4. Take baseline observations (temperature, pulse, BP, SpO₂).
5. Monitor at 15 minutes after starting each unit (when most acute reactions manifest).
6. Complete transfusion documentation.
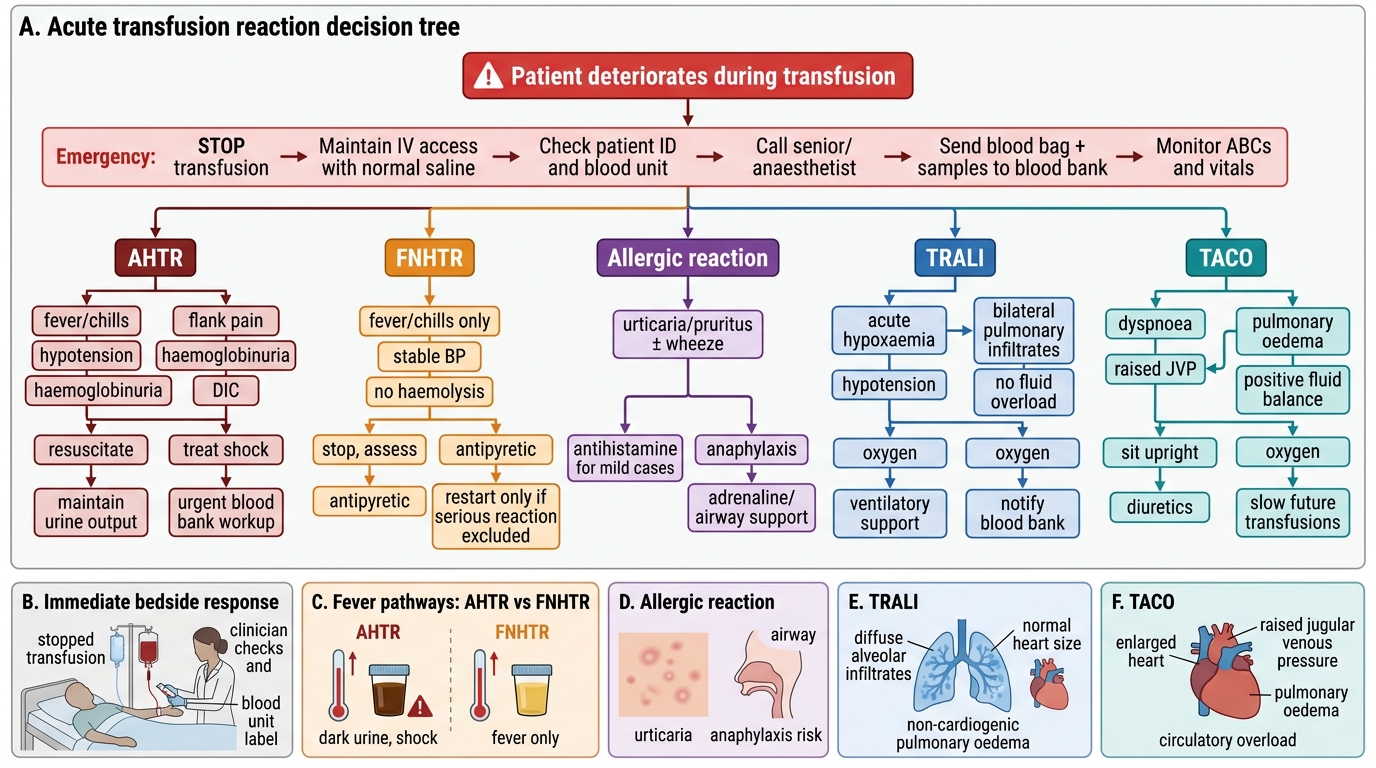
Acute Transfusion Reaction Decision Tree
Self-Assessment: Fluids and Blood Products
Competence in perioperative fluid and blood product management requires not only factual recall but the ability to apply principles dynamically in time-pressured clinical situations. Self-assessment in this domain must therefore address both the knowledge layer (classification, indications, mechanisms) and the clinical reasoning layer (when to give, when to stop, what to monitor). The questions below are designed to expose gaps at both levels. Answer them honestly before checking any reference, then revisit any question you cannot answer confidently with a focused review of the relevant arc section above. Research on clinical expertise consistently shows that learners who generate their own answers to application questions — even imperfectly — before receiving correct answers retain the material far better than those who passively re-read a summary. Treat these questions as a retrieval practice exercise, not a test of readiness.
Knowledge-level questions:
- What electrolyte disturbance distinguishes large-volume normal saline infusion from Hartmann's solution infusion, and what is the mechanism?
- State the four blood components, their storage temperatures, and shelf lives.
- What is the fibrinogen threshold that mandates cryoprecipitate administration in a bleeding patient?
- Explain the difference between TRALI and TACO in terms of mechanism, CXR appearance, and management.
Clinical reasoning questions:
- A 70 kg woman undergoing colonic resection has a preoperative Hb of 10.5 g/dL. Estimated blood loss is 800 mL. Would you transfuse PRBCs? Calculate her MABL (assume minimum acceptable haematocrit 21%, average haematocrit 34%).
- During a major liver resection, SVV on the arterial line reads 18%. You give a 250 mL Hartmann's bolus — SVV falls to 9%. What does this tell you, and what do you do next?
- A patient receiving their third unit of FFP develops acute hypoxia and a temperature of 38.8°C 90 minutes into the transfusion. The CXR shows bilateral pulmonary infiltrates. BP is maintained at 105/70. What is the diagnosis and immediate management?
Students who complete this self-assessment honestly and discuss their answers with a supervisor will be better prepared for the DOPS-style assessments and oral examinations that form the summative assessment of AS9.3 and AS9.4 competencies.
CLINICAL PEARL
'One size fits all' fluid prescribing is obsolete: the traditional practice of writing '1 litre Hartmann's over 8 hours' as a standing postoperative order ignores the enormous inter-patient variability in fluid needs. A fit 30-year-old after a laparoscopic appendicectomy and an 80-year-old with heart failure after a bowel resection have almost nothing in common in terms of fluid balance requirements. Every fluid prescription should specify the type, volume, rate, and the haemodynamic or biochemical trigger for reassessment. Likewise, in massive haemorrhage, do not wait for laboratory results before giving FFP and cryoprecipitate — in a patient bleeding at a rate that will cause death before coagulation results return, empirical damage-control ratios (PRBC:FFP:platelets = 1:1:1) should begin immediately, with results used to refine ongoing administration.