Page 2 of 9
AN10.1-13 | Axilla, Shoulder and Scapular region — SDL Guide (Part 2)
The Brachial Plexus — A Highway System for the Arm (AN10.3)
Every movement of your arm — from waving to writing to performing surgery — is controlled by nerves that originate from your spinal cord. These nerves don't travel to the arm individually; they first merge, split, and reorganise into a complex network called the brachial plexus.

Figure: The Brachial Plexus — A Highway System for the Arm (AN10.3)
Think of it as a highway interchange system: five entrance ramps (spinal nerve roots) merge into highways (trunks), pass through an interchange (divisions), reorganise into new highways (cords), and finally exit as individual routes (terminal branches) to specific muscles and skin areas.
The brachial plexus has five levels, remembered by the mnemonic "Robert Taylor Drinks Cold Beer":
1. Roots — C5, C6, C7, C8, T1 (five spinal nerve ventral rami)
2. Trunks — three: upper (C5+C6), middle (C7 alone), lower (C8+T1)
3. Divisions — each trunk splits into anterior and posterior divisions (6 total)
4. Cords — three, named by their position around the axillary artery:
- Lateral cord — anterior divisions of upper + middle trunks (C5,6,7)
- Posterior cord — all three posterior divisions (C5,6,7,8,T1)
- Medial cord — anterior division of lower trunk (C8,T1)
5. Branches — terminal nerves that supply the arm
The key terminal branches are:
• Musculocutaneous nerve (C5,6,7) — from the lateral cord → supplies anterior arm muscles (biceps)
• Median nerve (C5–T1) — from lateral + medial cords → supplies forearm flexors and hand
• Ulnar nerve (C8,T1) — from the medial cord → the 'funny bone' nerve
• Radial nerve (C5–T1) — from the posterior cord → supplies all extensors
• Axillary nerve (C5,6) — from the posterior cord → supplies deltoid and teres minor
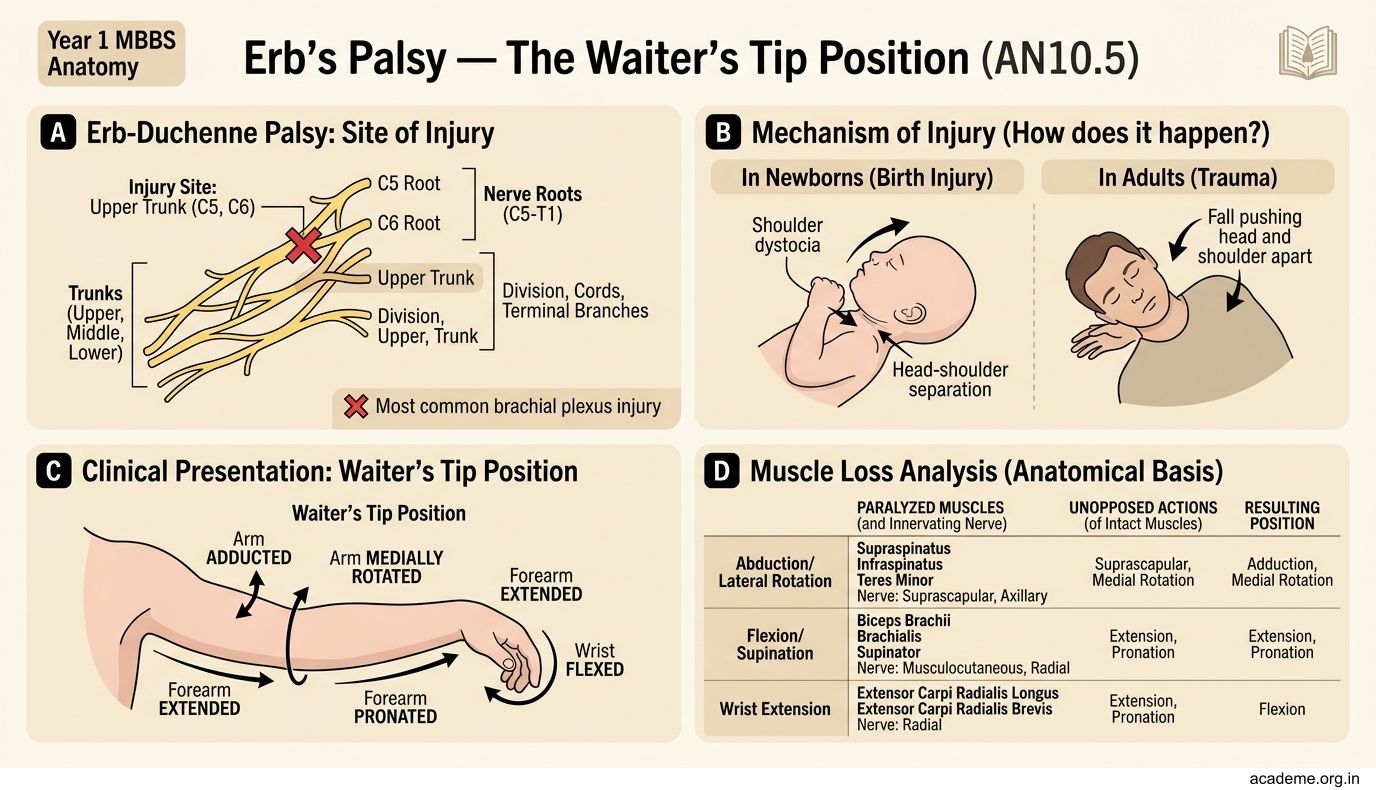
Erb's Palsy — The Waiter's Tip Position (AN10.5)
When the upper trunk of the brachial plexus (C5, C6) is injured, it's called Erb-Duchenne palsy (commonly just Erb's palsy). This is the most common brachial plexus injury.
How does it happen?
• In newborns: during a difficult delivery when the baby's head is pulled to one side while the shoulder is stuck (shoulder dystocia)
• In adults: a fall onto the shoulder with the head pushed to the opposite side, or a motorcycle accident
The injury damages nerves that supply the shoulder abductors (deltoid), external rotators (infraspinatus), elbow flexors (biceps, brachialis), and supinators (supinator, biceps).
The result — the "waiter's tip" position:
• The arm hangs limply at the side (adducted — deltoid paralysed)
• The arm is medially rotated (external rotators paralysed, internal rotators unopposed)
• The elbow is extended (biceps paralysed)
• The forearm is pronated (supinators paralysed)
The hand looks like the person is waiting for a tip — palm facing backward and outward. The hand grip is preserved because the lower roots (C8, T1) are intact.
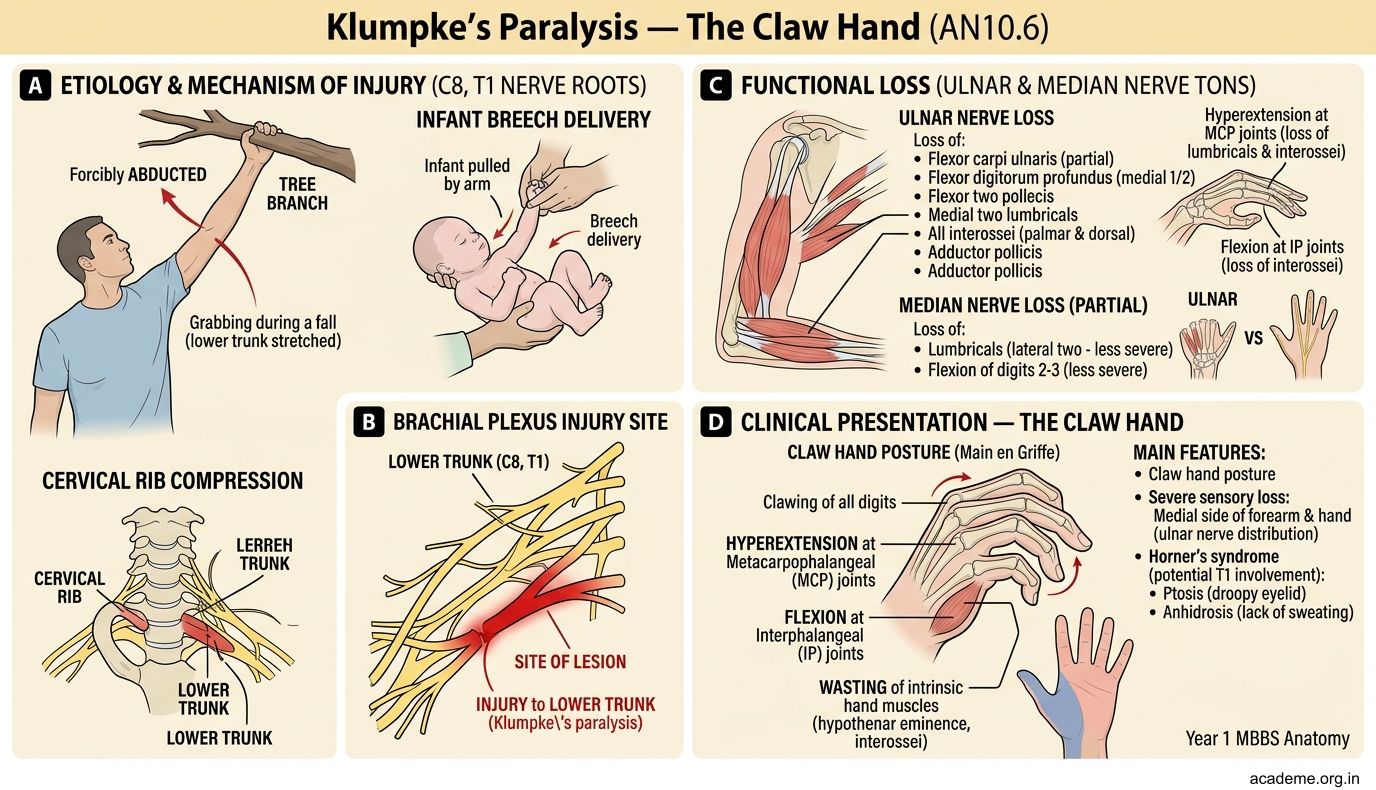
Klumpke's Paralysis — The Claw Hand (AN10.6)
When the lower trunk of the brachial plexus (C8, T1) is injured, it's called Klumpke's paralysis. This is less common than Erb's palsy.
How does it happen?
• Grabbing a tree branch or railing during a fall (the arm is forcibly abducted and the lower trunk is stretched)
• In newborns: a breech delivery where the arm is pulled upward
• Cervical rib compressing the lower trunk
The injury damages nerves that supply the small muscles of the hand (intrinsic hand muscles via T1) and the long flexors of the fingers (via C8).
The result — the "claw hand":
• The hand has a clawed appearance — hyperextension at the metacarpophalangeal joints with flexion at the interphalangeal joints (because the lumbricals and interossei are paralysed)
• Loss of grip strength
• Sensory loss over the medial side of the hand and forearm
• If T1 is involved: Horner's syndrome may occur (because T1 carries sympathetic fibres to the eye) — ptosis (drooping eyelid), miosis (constricted pupil), and anhidrosis (loss of sweating on that side of the face)
Compare and contrast:
• Erb's palsy = upper trunk (C5,C6) = shoulder/elbow affected, hand spared
• Klumpke's paralysis = lower trunk (C8,T1) = hand affected, shoulder spared
SELF-CHECK
A newborn delivered after shoulder dystocia presents with the right arm adducted, medially rotated, elbow extended, and forearm pronated. The hand grip is preserved. Which part of the brachial plexus is most likely injured?
A. Lower trunk (C8, T1)
B. Upper trunk (C5, C6)
C. Posterior cord
D. All five roots
Reveal Answer
Answer: B. Upper trunk (C5, C6)
This is the classic 'waiter's tip' position of Erb's palsy — injury to the upper trunk (C5, C6). The shoulder and elbow are affected but the hand is spared. Key clue: hand grip is preserved (C8, T1 intact). Shoulder dystocia causes traction on the upper trunk as the head is pulled away from the trapped shoulder.
CLINICAL PEARL
Birth injuries to the brachial plexus occur in approximately 1–2 per 1000 births. Risk factors include macrosomia (large baby, >4 kg), shoulder dystocia, prolonged labour, and instrumental delivery. In India, where home deliveries and delayed referrals still occur in rural areas, brachial plexus injuries are an important cause of disability. Most neonatal Erb's palsy (80–90%) recovers spontaneously within 3–6 months. If there's no recovery by 3 months, nerve surgery (nerve grafting or nerve transfer) should be considered. Klumpke's paralysis has a poorer prognosis because the small hand muscles, once denervated, don't recover as well.