Page 1 of 6
AN12.1-15 | Forearm & hand — SDL Guide
The forearm and hand are the body's primary tools for interaction with the world. In this module you will learn the muscles, nerves, vessels, compartments, and spaces of the forearm and hand — building the anatomical foundation for diagnosing carpal tunnel syndrome, wrist drop, claw hand, palmar infections, and De Quervain's tenosynovitis.
Learning Objectives
- Describe and demonstrate the muscles of the ventral forearm — their attachments, nerve supply, and actions (AN12.1)
- Identify nerves and vessels of the forearm — their origin, course, relations, branches, and termination (AN12.2)
- Describe the flexor retinaculum with its attachments (AN12.3)
- Explain the anatomical basis of carpal tunnel syndrome (AN12.4)
- Identify and describe small muscles of the hand; describe movements of the thumb and muscles involved (AN12.5, AN12.6)
- Identify and describe the course and branches of blood vessels and nerves in the hand (AN12.7)
- Describe the anatomical basis of claw hand (AN12.8)
- Identify and describe fibrous flexor sheaths, bursae, and digital synovial sheaths (AN12.9)
- Explain fascial space infections of the palm (AN12.10)
- Identify and demonstrate dorsal forearm muscles with attachments, nerve supply, and actions (AN12.11)
- Identify nerves and vessels of the back of the forearm (AN12.12)
- Describe the anatomical basis of wrist drop (AN12.13)
- Identify compartments deep to the extensor retinaculum and describe the anatomical snuffbox (AN12.14)
- Identify and describe extensor expansion (dorsal digital expansion) formation (AN12.15)
INSTRUCTIONS
This module is split into five content sections. Work through them in order — each section builds on the last. Complete the self-check questions at the end of each section before moving on. Have your dissection notes and atlas alongside this guide.
References
- Gray's Anatomy for Students (Drake et al.) — Chapter 7: Upper Limb (Textbook)
- Clinically Oriented Anatomy (Moore et al.) — Forearm, Wrist, Hand (Textbook)
- OpenStax Anatomy and Physiology 2e — Muscles of the Pectoral Girdle and Upper Limbs (CC BY 4.0) (Open Access)
- BD Chaurasia's Human Anatomy, Vol. 1 — Upper Limb (Textbook)
Version 2.0 | Academe Content Engine v2, Faculty Review Pending
CLINICAL SCENARIO
A 35-year-old carpenter presents to a government hospital in Puducherry with a complaint that he cannot grip his tools properly after a deep laceration on the front of his wrist three days ago. On examination, the surgeon notices he cannot flex his index and middle fingers at the distal joints, and sensation is lost on the lateral palm and the first three fingers.
Which nerve was injured? Which muscles are now paralysed? Where exactly was the wound?
By the end of this module, you will be able to answer these questions — and more — with anatomical precision.
WHY THIS MATTERS
The forearm and hand are the body's primary tools for interaction with the world. In Indian healthcare, injuries to these structures are among the most common surgical emergencies — from road traffic accidents and occupational injuries in manual workers, to fractures in elderly patients. As a doctor, you will encounter:
- Carpal tunnel syndrome — one of the most common peripheral nerve entrapment syndromes
- Wrist drop (radial nerve injury) — classic complication of mid-shaft humeral fractures
- Claw hand (ulnar nerve injury) — seen after medial epicondyle fractures or lacerations
- Palmar space infections — serious complications of penetrating injuries in labourers
Understanding the precise anatomy of the forearm and hand is not academic — it is the foundation for every clinical examination, every tendon repair, every nerve block you will perform in your career.
RECALL
Before we begin, recall what you learned about the arm and cubital fossa:
- The brachial artery divides at the neck of the radius into the radial and ulnar arteries
- The median nerve passes through the cubital fossa medial to the brachial artery
- The radial nerve divides at the lateral epicondyle into superficial (sensory) and deep (motor = posterior interosseous) branches
- The ulnar nerve passes posterior to the medial epicondyle (hence vulnerable in "funny bone" injuries)
- The forearm contains two bones: the radius (lateral) and ulna (medial), connected by the interosseous membrane
Part 1: Ventral (Anterior) Forearm — Muscles, Nerves, and Vessels
The front of the forearm contains the anterior (flexor) compartment — 8 muscles arranged in three layers, almost entirely supplied by the median nerve, with one important exception.

Figure: Part 1: Ventral (Anterior) Forearm — Muscles, Nerves, and Vessels
Superficial Layer (4 muscles — origin: medial epicondyle via common flexor origin):
- Pronator teres — pronates the forearm; nerve: median; two heads (humeral + ulnar) with the median nerve passing between them
- Flexor carpi radialis (FCR) — flexes and abducts the wrist; nerve: median; its tendon is the landmark for the radial artery pulse at the wrist
- Palmaris longus — weakly flexes wrist; nerve: median; absent in ~15% of people; its tendon is harvested for tendon grafts
- Flexor carpi ulnaris (FCU) — flexes and adducts the wrist; nerve: ulnar nerve (C8, T1) — the only superficial flexor NOT supplied by the median nerve
Intermediate Layer (1 muscle):
• Flexor digitorum superficialis (FDS) — flexes the middle phalanges of fingers 2–5; nerve: median nerve; tendons split at the proximal phalanx to allow FDP to pass through
Deep Layer (3 muscles):
• Flexor digitorum profundus (FDP) — flexes distal phalanges (fingers 2–5); nerve: medial half (ring + little) by ulnar nerve; lateral half (index + middle) by the anterior interosseous nerve (AIN, a branch of median)
• Flexor pollicis longus (FPL) — flexes the thumb's interphalangeal joint; nerve: AIN (median)
• Pronator quadratus — pronates forearm at the distal radioulnar joint; nerve: AIN; deepest muscle, directly on radius and ulna
The Anterior Interosseous Nerve (AIN): A purely motor branch of the median nerve. It supplies FDP (lateral half), FPL, and pronator quadratus. Injury causes inability to form an "OK" sign — the index finger and thumb cannot form a circle because terminal flexion is lost.
Nerves and Vessels of the Forearm:
| Nerve | Motor in forearm | Sensory |
|---|---|---|
| Median | All flexors except FCU and medial FDP | Lateral 3½ fingers (palm) |
| Ulnar | FCU, medial FDP | Medial 1½ fingers |
| Radial (superficial) | None (purely sensory in forearm) | Dorsal lateral hand |
| Posterior interosseous n. | All posterior compartment muscles | None |
The radial artery pulse is palpable at the wrist between the FCR tendon and the radial styloid. The ulnar artery is accompanied by the ulnar nerve in the distal forearm, passing through Guyon's canal at the wrist.
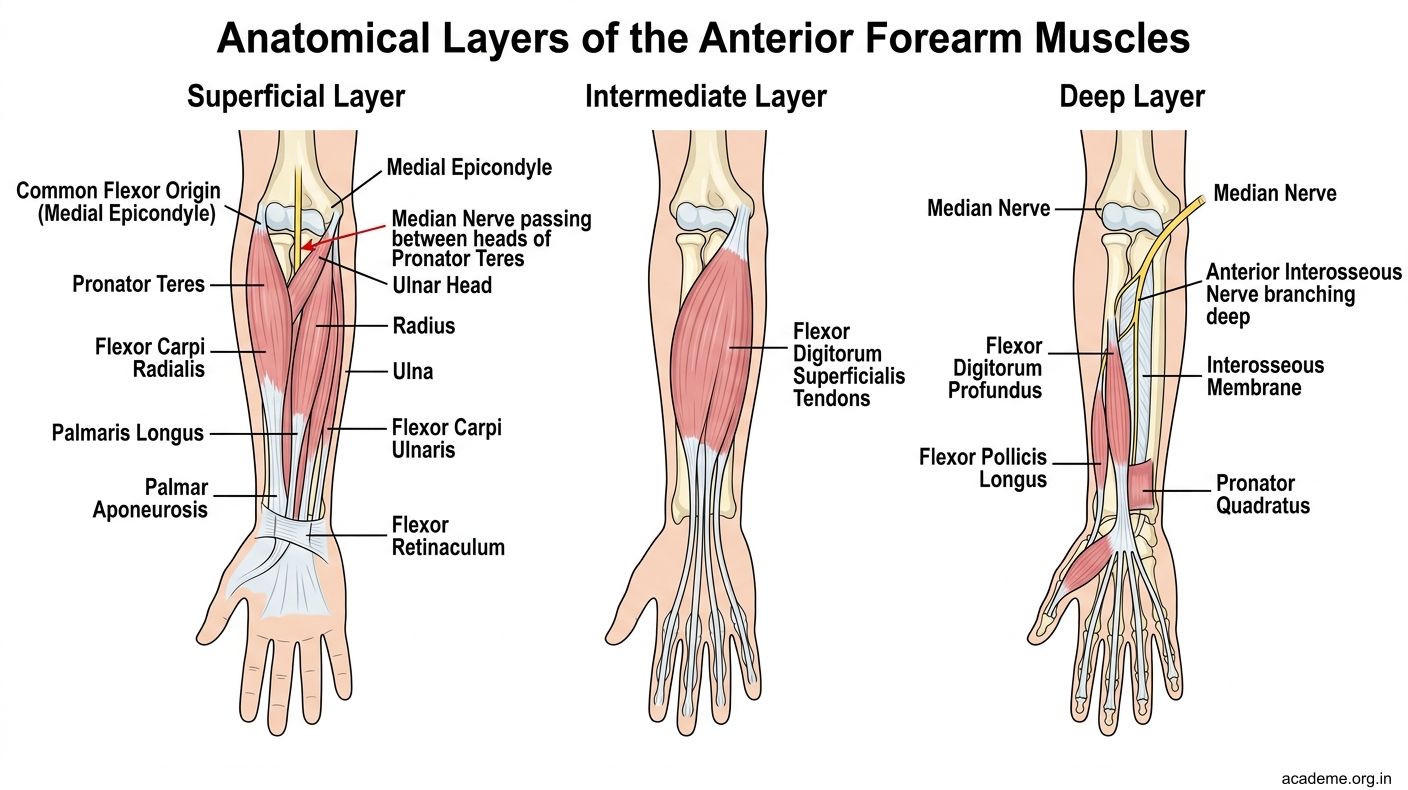
Figure: Part 1: Ventral (Anterior) Forearm — Muscles, Nerves, and Vessels

Figure: Nerves and Vessels of the Forearm:
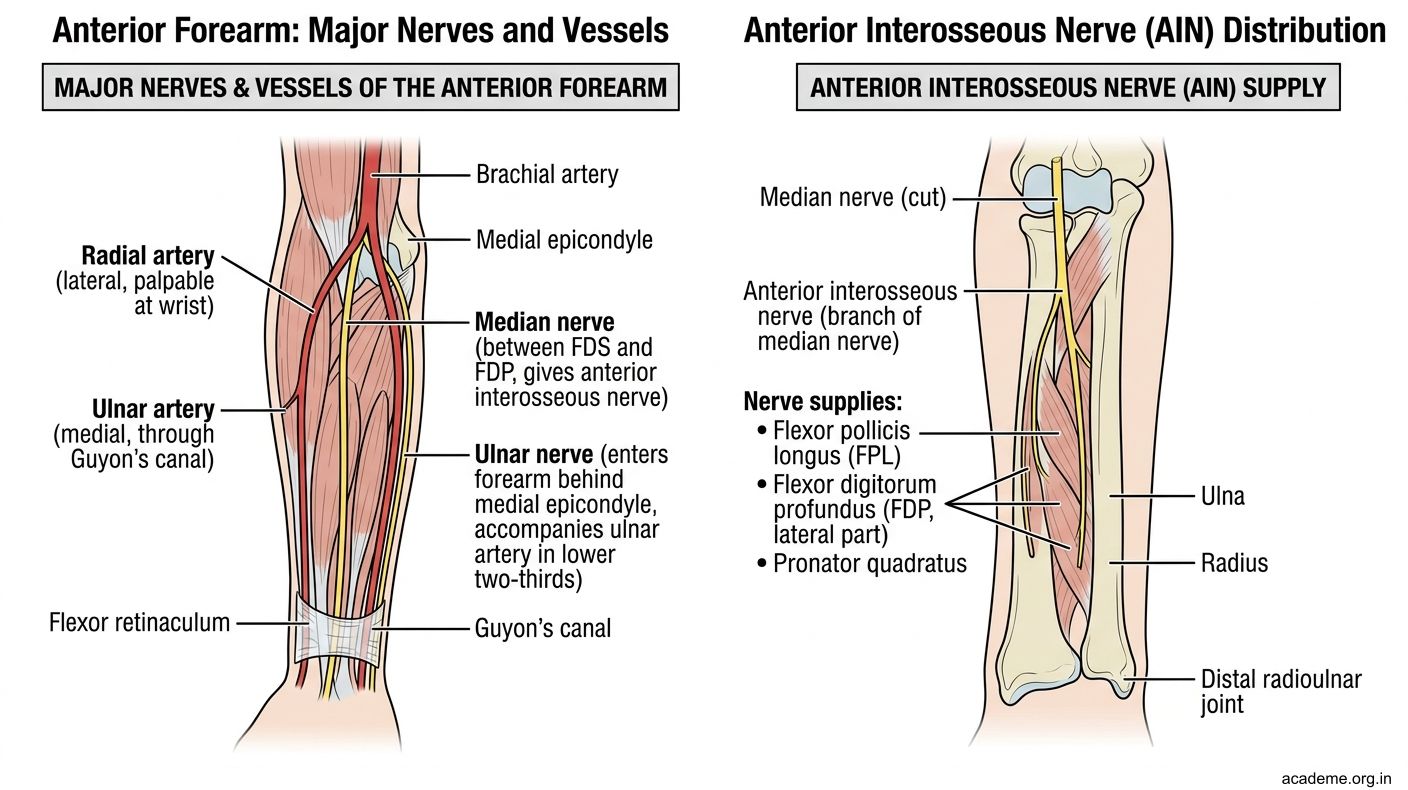
Figure: Nerves and Vessels of the Forearm:
SELF-CHECK — : Ventral Forearm
A patient sustains an injury to the median nerve at the wrist. Which muscle of the anterior forearm will RETAIN its function?
A. Flexor carpi radialis
B. Flexor carpi ulnaris
C. Flexor digitorum superficialis
D. Pronator teres
Reveal Answer
Answer: B. Flexor carpi ulnaris
The Anterior Interosseous Nerve (AIN) is a branch of which nerve?
A. Ulnar nerve
B. Radial nerve
C. Median nerve
D. Musculocutaneous nerve
Reveal Answer
Answer: C. Median nerve
Part 2: Flexor Retinaculum, Carpal Tunnel Syndrome & Muscles of the Hand
The Flexor Retinaculum

Figure: Movements of the Thumb (AN12.6)

Figure: Small Muscles of the Hand (AN12.5)

Figure: Carpal Tunnel Syndrome (AN12.4)

Figure: The Flexor Retinaculum
The flexor retinaculum (transverse carpal ligament) is a thick fibrous band bridging across the concavity of the carpal bones, converting it into the carpal tunnel.
Attachments: Medially — pisiform and hook of hamate. Laterally — scaphoid tubercle and trapezium ridge.
Contents of the carpal tunnel:
1. Flexor digitorum superficialis (4 tendons)
2. Flexor digitorum profundus (4 tendons)
3. Flexor pollicis longus (1 tendon)
4. Median nerve — the ONLY nerve in the carpal tunnel
Note: The ulnar nerve and ulnar artery pass through Guyon's canal (ulnar canal) — superficial and medial to the retinaculum, NOT through the carpal tunnel.
Carpal Tunnel Syndrome (AN12.4)
CTS is compression of the median nerve within the carpal tunnel.
Anatomical basis: Any increase in volume within the fixed space of the carpal tunnel (thickened flexor tendon sheaths, oedema in pregnancy, hypothyroidism) compresses the median nerve.
Symptoms: Pain and tingling in the lateral 3½ fingers; worse at night; weakness and wasting of the thenar eminence (especially abductor pollicis brevis — exclusively supplied by the recurrent branch of median nerve just distal to the retinaculum).
Clinical tests: Tinel's sign (tap over carpal tunnel = reproduces symptoms); Phalen's test (sustained wrist flexion for 60 s).
Small Muscles of the Hand (AN12.5)
Thenar muscles (thumb side): APB (abducts thumb ⊥ palm; median), opponens pollicis (opposes; median), FPB (flexes proximal phalanx; median superficial head + ulnar deep head), adductor pollicis (adducts; ulnar deep branch — NOT a thenar muscle by position).
Hypothenar muscles (little finger side): All supplied by the ulnar nerve (deep branch).
Intermediate muscles:
• Lumbricals (4): Flex MCPJs + extend IPJs; lateral 2 by median, medial 2 by ulnar
• Palmar interossei (3): ADduct fingers (PAD = Palmar ADduct); all ulnar
• Dorsal interossei (4): ABduct fingers (DAB = Dorsal ABduct); all ulnar
Movements of the Thumb (AN12.6)
The carpometacarpal joint (CMCJ) of the thumb is a saddle joint — the most mobile joint in the hand. Opposition (abduction + flexion + medial rotation) is the uniquely human movement that makes tool use possible.
| Movement | Key muscles | Nerve |
|---|---|---|
| Opposition | Opponens pollicis + FPB + APB | Median |
| Adduction | Adductor pollicis | Ulnar |
| Extension | EPL, EPB | Radial |
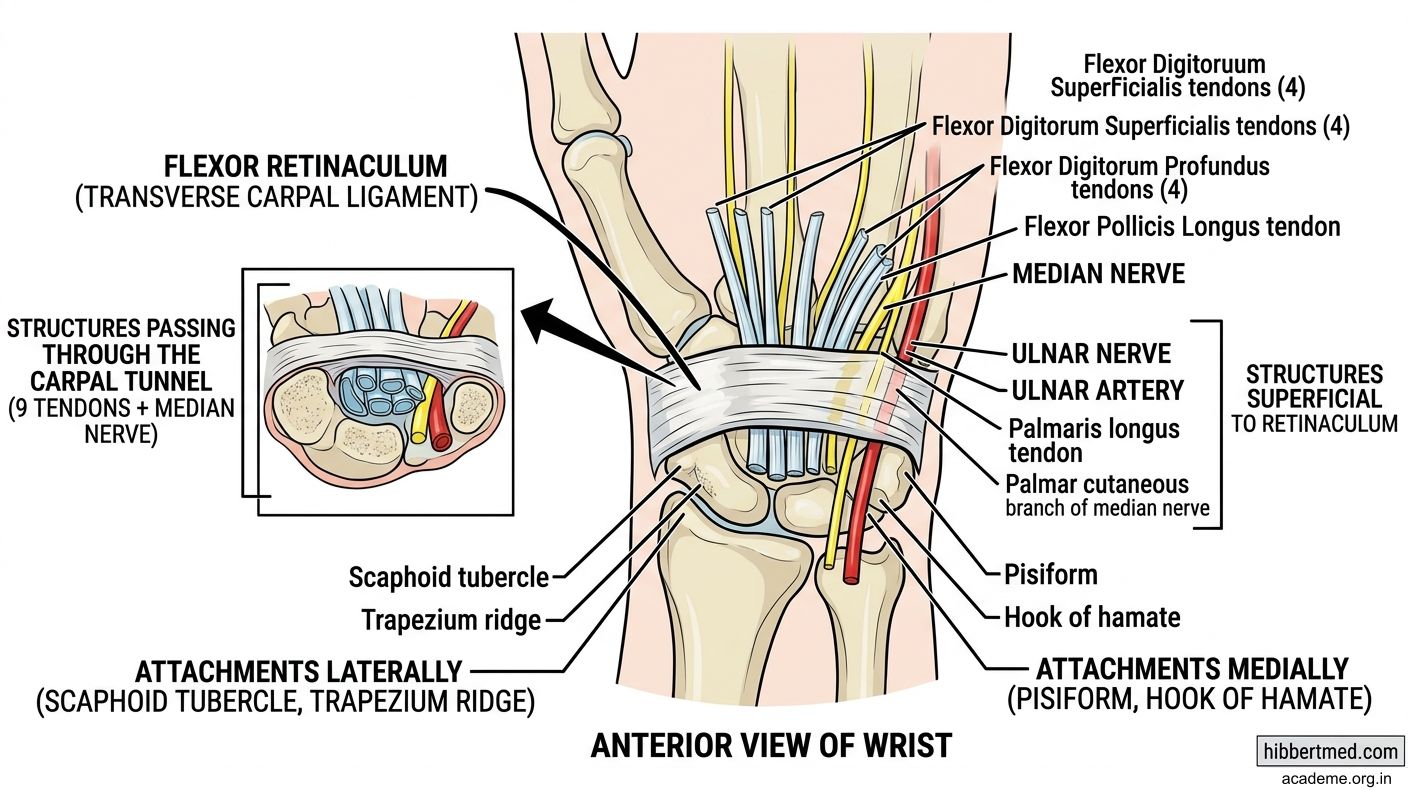
Figure: The Flexor Retinaculum
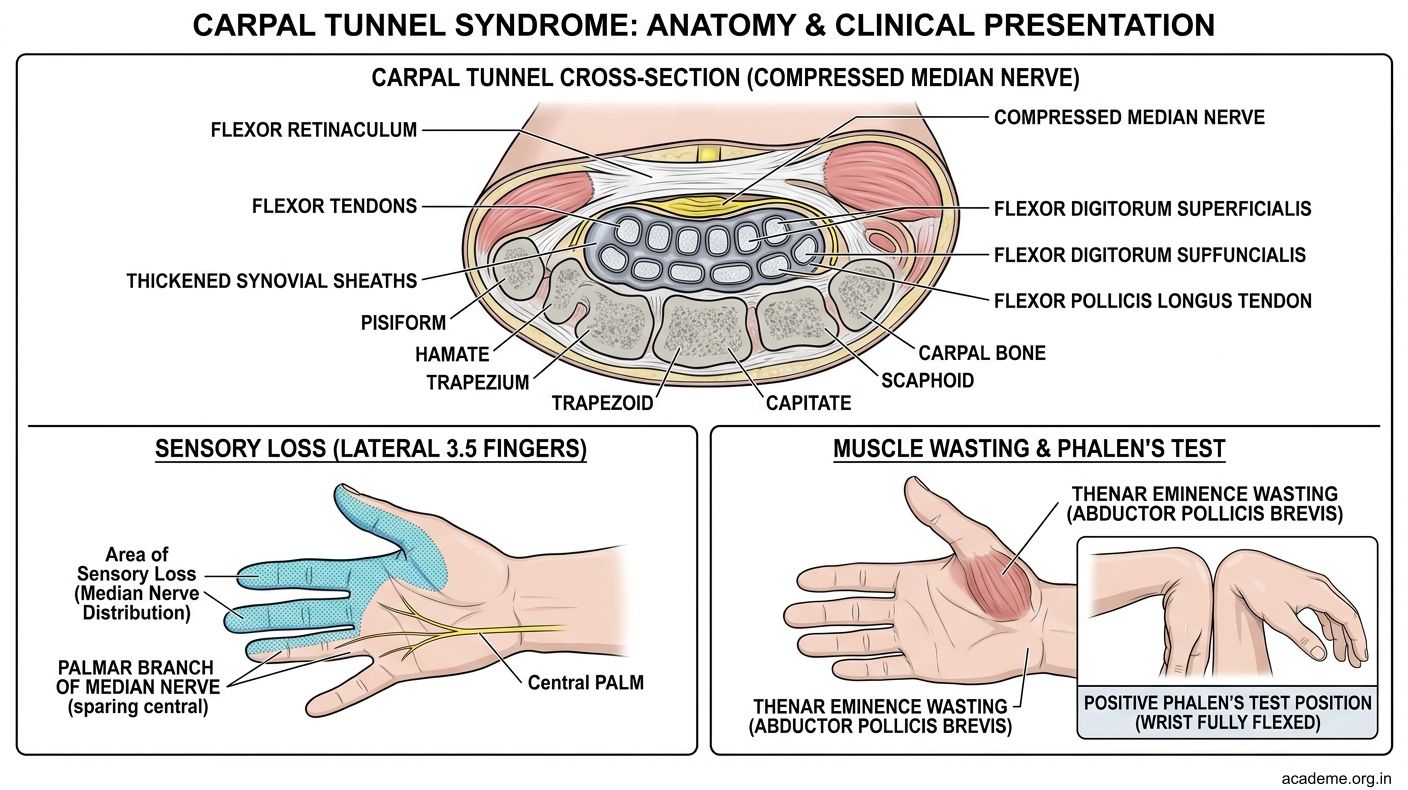
Figure: Carpal Tunnel Syndrome (AN12.4)
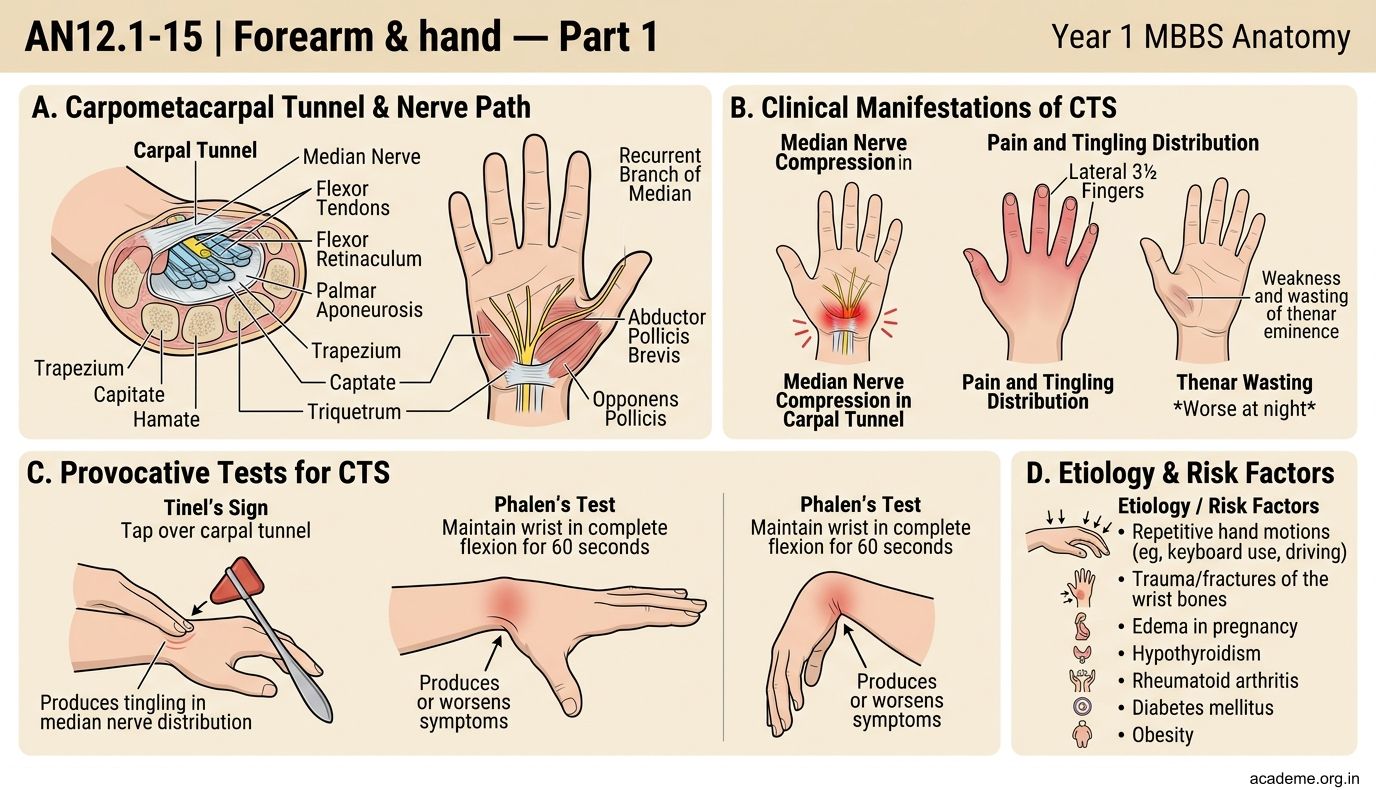
Figure: Small Muscles of the Hand (AN12.5)
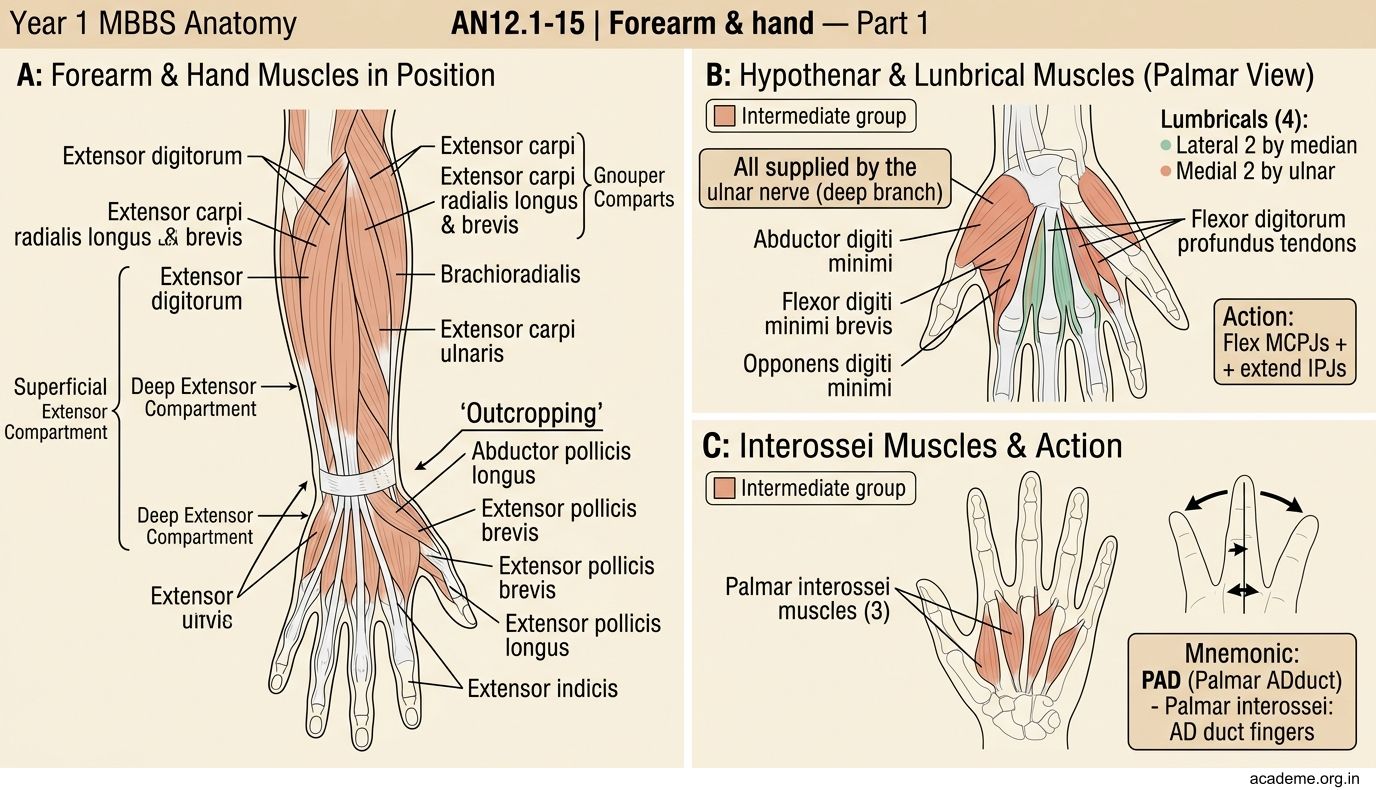
Figure: Movements of the Thumb (AN12.6)
CLINICAL PEARL
Froment's sign tests the adductor pollicis (ulnar nerve). Ask the patient to hold a piece of paper between the thumb and index finger. In ulnar nerve palsy, the adductor pollicis is weak, so the patient compensates by flexing the thumb's interphalangeal joint using flexor pollicis longus (median nerve) — producing the characteristic "Froment's sign" (flexed IPJ of thumb during pinch).
Froment's sign = ulnar nerve palsy. The compensating muscle is FPL (median nerve). Commonly tested in clinical viva examinations.
SELF-CHECK — : Carpal Tunnel & Hand Muscles
A patient with carpal tunnel syndrome has weakness of which specific muscle in the thenar eminence?
A. Adductor pollicis
B. Flexor pollicis longus
C. Abductor pollicis brevis
D. Opponens digiti minimi
Reveal Answer
Answer: C. Abductor pollicis brevis
Which of the following is NOT a content of the carpal tunnel?
A. FDS tendons
B. Median nerve
C. Ulnar nerve
D. FPL tendon
Reveal Answer
Answer: C. Ulnar nerve
Part 3: Vessels and Nerves of the Hand, Claw Hand, and Palmar Infections
Arterial Supply of the Hand (AN12.7)

Figure: Fascial Spaces of the Palm (AN12.10)

Figure: Fibrous Flexor Sheaths and Bursae (AN12.9)

Figure: Claw Hand (AN12.8)

Figure: Part 3: Vessels and Nerves of the Hand, Claw Hand, and Palmar Infections
The hand is supplied by the radial and ulnar arteries, anastomosing to form two arches:
Superficial palmar arch: Formed mainly by the ulnar artery, completed by the superficial branch of the radial artery. Lies deep to the palmar aponeurosis; gives 3 common palmar digital arteries → proper digital arteries for the medial 3½ fingers.
Deep palmar arch: Formed mainly by the radial artery (via the anatomical snuffbox and 1st dorsal interosseous space), completed by the deep branch of ulnar. Gives palmar metacarpal arteries.
Allen's test checks patency of both arteries before radial artery cannulation or harvest.
Nerves of the Hand:
| Nerve | Motor supply | Sensory supply |
|---|---|---|
| Median (recurrent + digital branches) | Thenar (APB, OP, FPB-sup), lateral 2 lumbricals | Lateral 3½ fingers (palm + dorsal tips) |
| Ulnar (deep + superficial) | Hypothenar, medial 2 lumbricals, all interossei, adductor pollicis, FPB-deep | Medial 1½ fingers |
| Radial (superficial branch only) | None in the hand | Dorsal lateral hand only |
Claw Hand (AN12.8)
Claw hand (ulnar nerve injury) results from:
• Lumbricals and interossei (ulnar) paralysed → cannot flex MCPJs or extend IPJs
• Long flexors (FDP, FDS — intact) → flex the IPJs unopposed
• Extensor digitorum (radial, intact) → extends the MCPJs unopposed
• Result: MCPJs extended + IPJs flexed = claw
Why worse in ring and little fingers? The lateral 2 lumbricals (index + middle) are supplied by the median nerve — they partially correct those fingers. Only medial 2 lumbricals (ring + little) are ulnar.
Paradox: Low ulnar lesion (at wrist) → more pronounced claw than high lesion (at elbow), because in high lesions FDP (medial half) is also paralysed, reducing the IPJ flexion.
Fibrous Flexor Sheaths and Bursae (AN12.9)
- Fibrous flexor sheaths: Pulley-like tunnels on the palmar surface of each finger, holding tendons against bone and preventing bowstringing
- Ulnar bursa (common flexor sheath): Encloses all tendons entering the carpal tunnel; extends from proximal to the wrist to mid-palm. The little finger's sheath connects continuously with the ulnar bursa.
- Radial bursa: Encloses FPL tendon; extends to the thumb's terminal phalanx
If the two bursae communicate (in ~50% of people), infection of either can spread → horseshoe abscess.
Fascial Spaces of the Palm (AN12.10)
Two potential spaces deep to the palmar aponeurosis:
• Thenar space (lateral): Infection = swelling of thenar eminence + immobile index finger
• Mid-palmar space (medial): Infection = dorsal + palmar oedema, semiflexed fingers
Infections spread via lumbrical canals to the dorsal web spaces → "collar-stud abscesses."
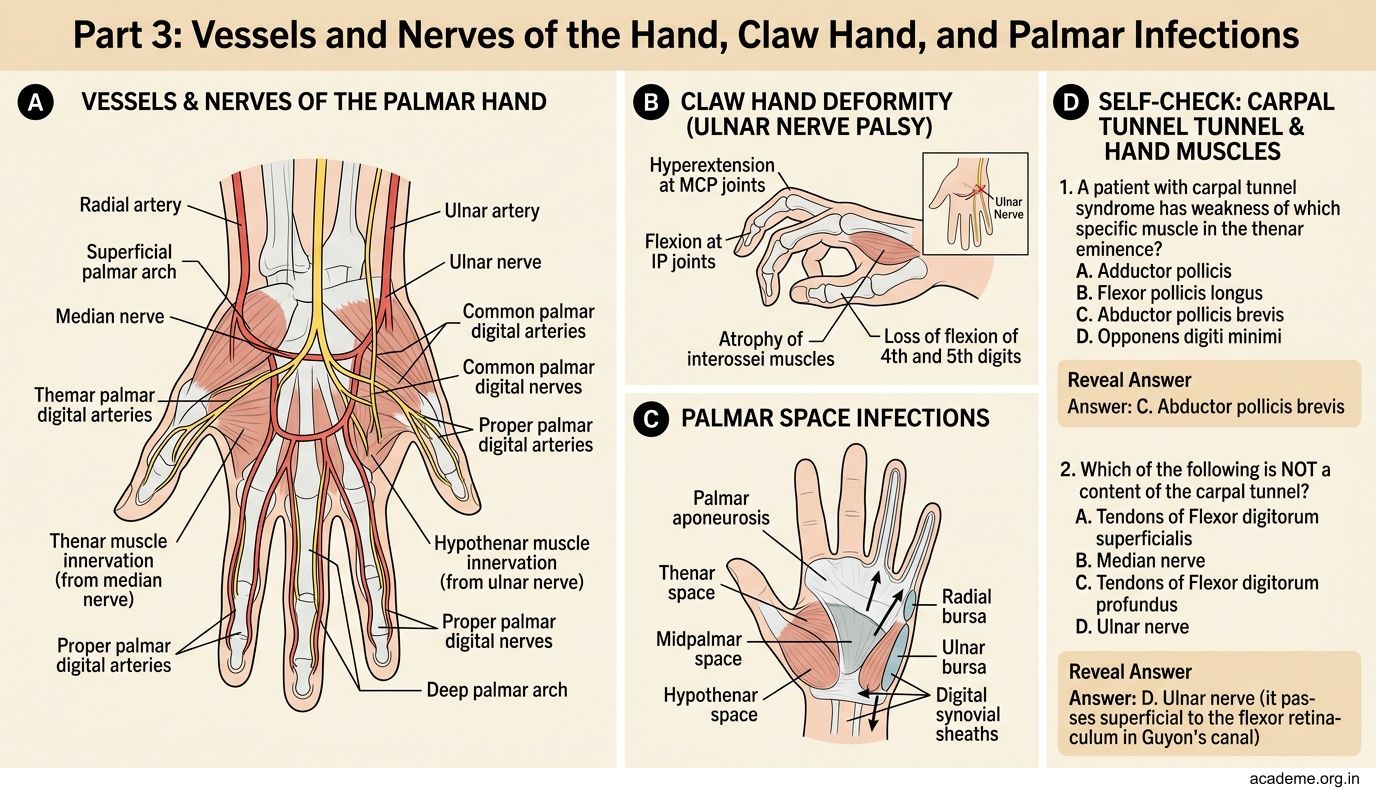
Figure: Part 3: Vessels and Nerves of the Hand, Claw Hand, and Palmar Infections

Figure: Nerves of the Hand:
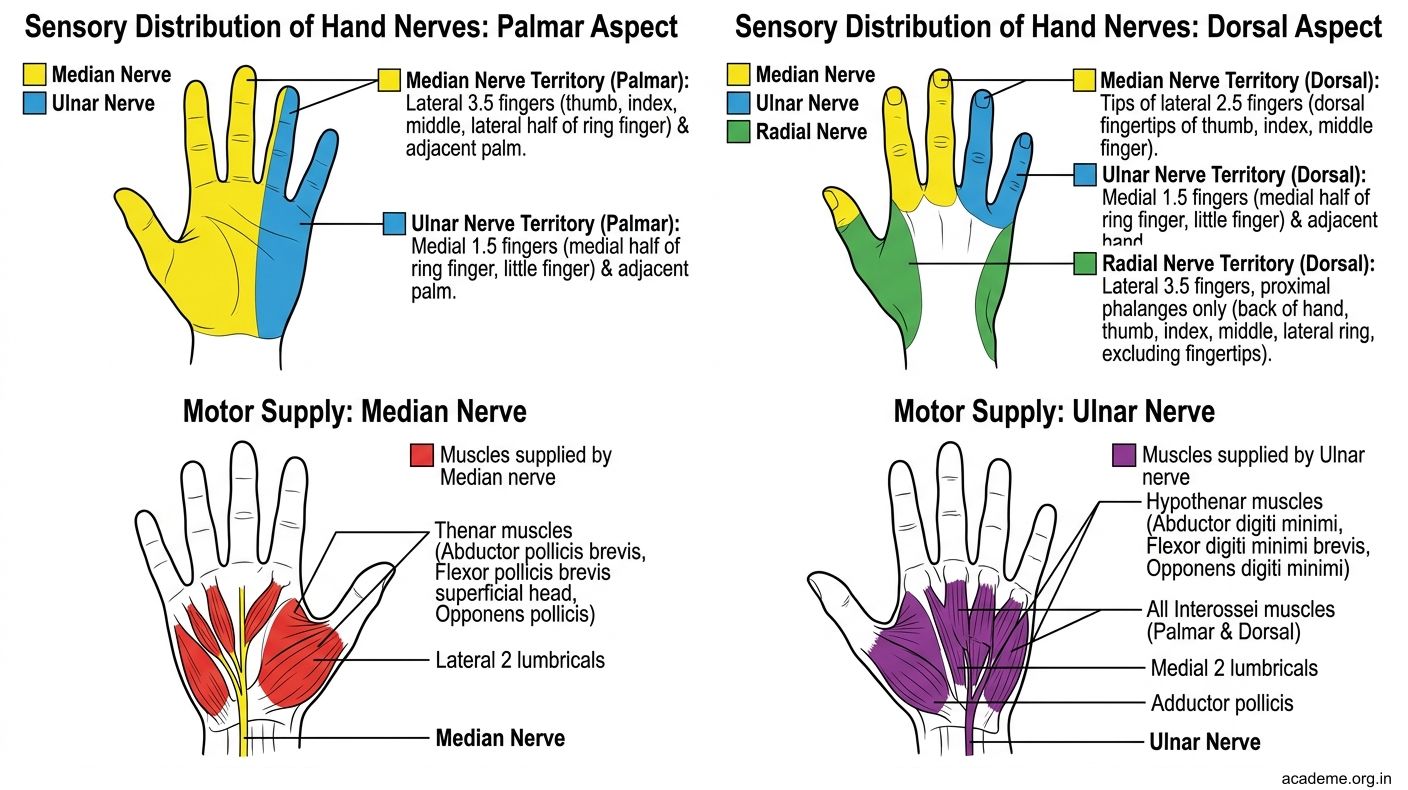
Figure: Nerves of the Hand:
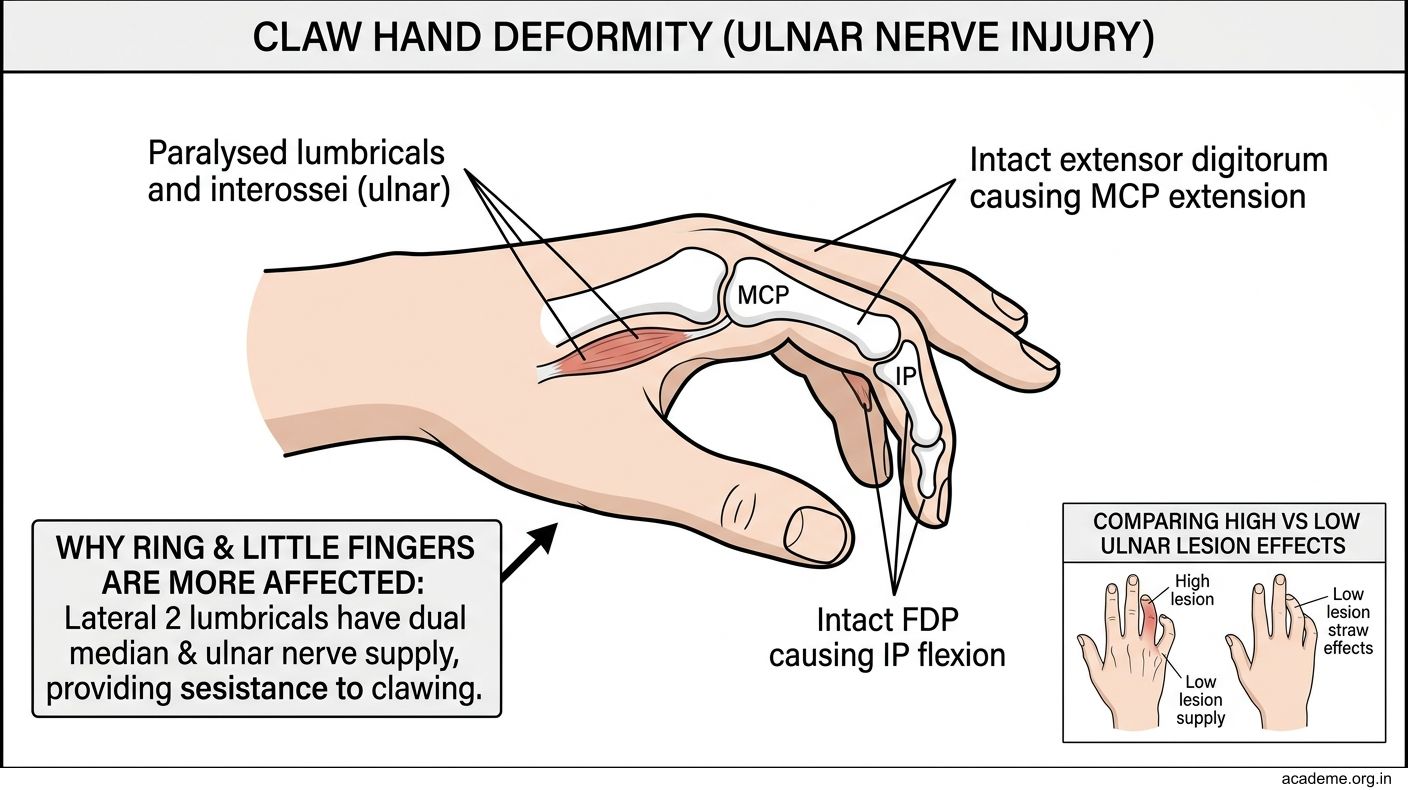
Figure: Claw Hand (AN12.8)
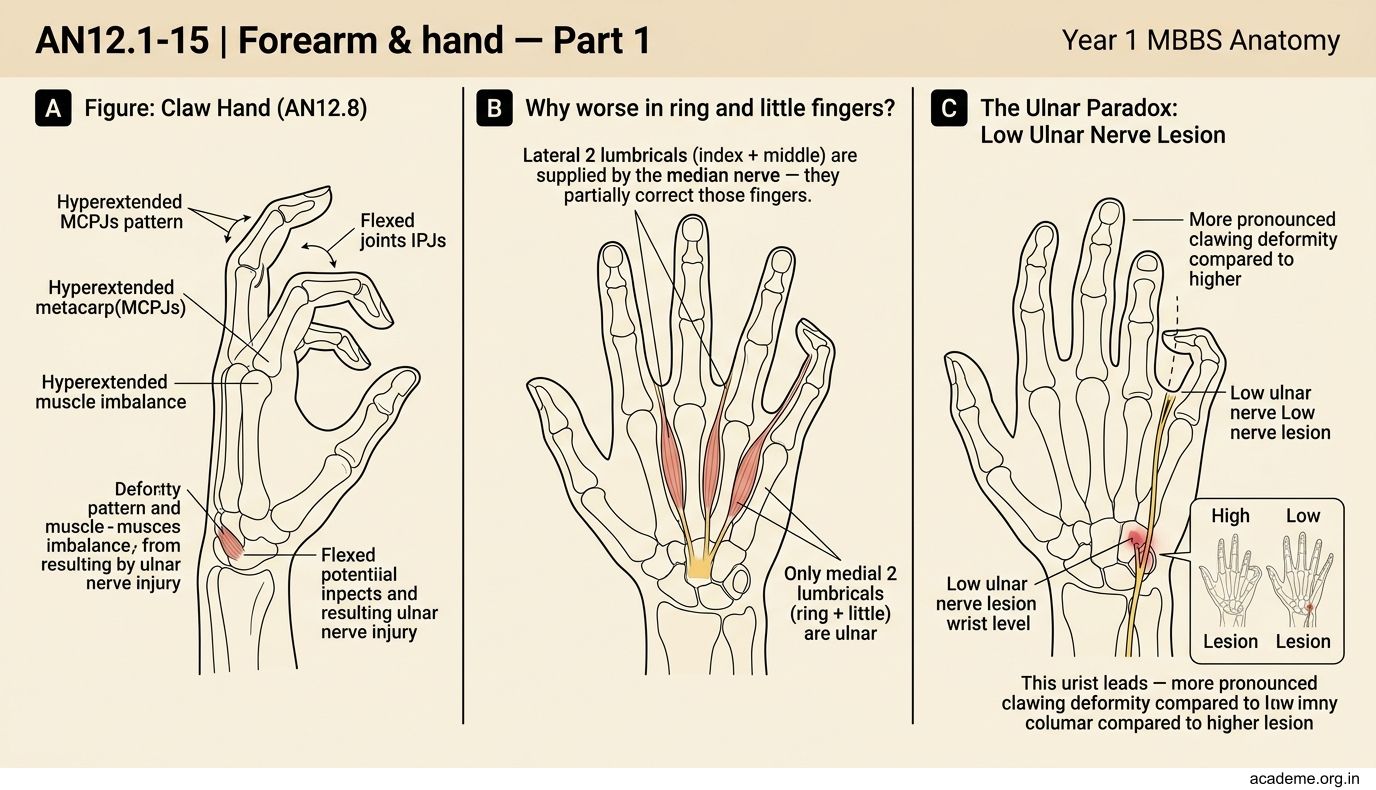
Figure: Fibrous Flexor Sheaths and Bursae (AN12.9)
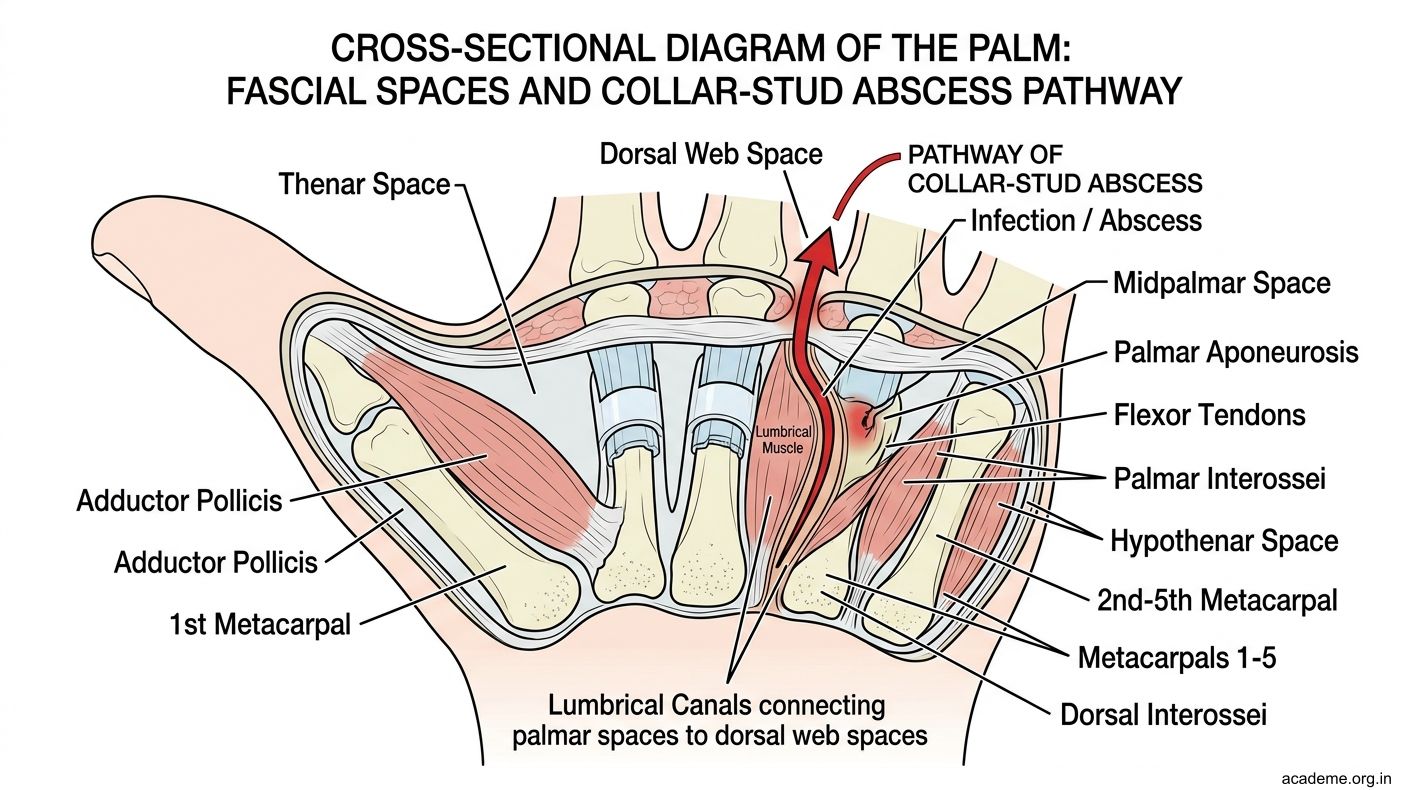
Figure: Fascial Spaces of the Palm (AN12.10)
SELF-CHECK — : Hand Vessels, Nerves & Claw Hand
A low ulnar nerve lesion at the wrist causes claw hand. Which fingers show the MOST pronounced clawing?
A. Index and middle fingers
B. Ring and little fingers
C. All four fingers equally
D. Little finger only
Reveal Answer
Answer: B. Ring and little fingers
The deep palmar arch is formed mainly by which artery?
A. Ulnar artery
B. Radial artery
C. Anterior interosseous artery
D. Superficial palmar branch of radial
Reveal Answer
Answer: B. Radial artery