Page 2 of 8
AN22.1-7 | Heart & Pericardium — SDL Guide (Part 2)
The Coronary Arteries — The Heart Feeds Itself First (AN22.3)
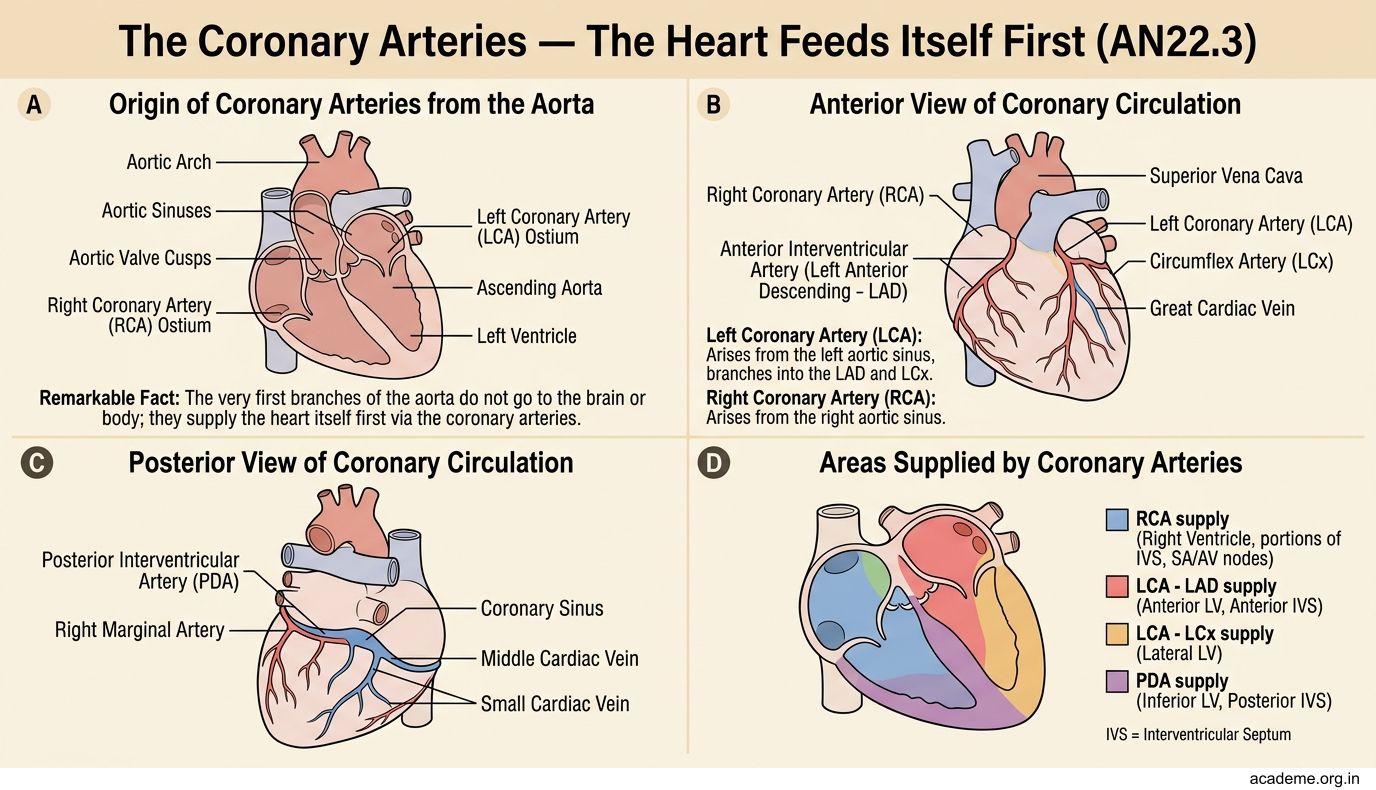
Here's a remarkable fact: the very first branches of the aorta don't go to the brain, the kidneys, or the muscles — they go straight back to the heart itself. The heart feeds itself first, before sending blood anywhere else in the body.
The coronary arteries arise from the aortic sinuses (small dilations just above the aortic valve). There are two:
- Left coronary artery (LCA) — arises from the left aortic sinus. After a short left main stem (1–2 cm), it divides into:
- Left anterior descending artery (LAD) — runs in the anterior interventricular groove (between the two ventricles on the front of the heart). Supplies: anterior wall of the left ventricle, anterior 2/3 of the interventricular septum, and the apex. This is the most commonly blocked artery in heart attacks.
- Left circumflex artery (LCx) — runs in the left atrioventricular groove (between the left atrium and left ventricle). Supplies: lateral and posterior wall of the left ventricle, left atrium
- Right coronary artery (RCA) — arises from the right aortic sinus. Runs in the right atrioventricular groove. Supplies: right atrium, right ventricle, SA node (in 60% of people), AV node (in 80% of people), posterior 1/3 of the interventricular septum, and the inferior wall of the left ventricle (via the posterior descending artery in right-dominant circulation)
Dominance: The artery that gives off the posterior descending artery (PDA) determines the 'dominance' of the heart:
• Right dominant (85% of people) — PDA comes from the RCA
• Left dominant (8%) — PDA comes from the LCx
• Co-dominant (7%) — PDA is supplied by both
Think of it this way: the LAD is the motorway feeding the front of the heart (anterior wall + septum), the LCx feeds the side (lateral wall), and the RCA feeds the back and bottom (inferior wall + posterior septum + the conducting system nodes).
Ischaemic Heart Disease — When the Pipes Block (AN22.4)
Ischaemic heart disease (IHD) is the single most common cause of death worldwide. In India, it's reaching epidemic proportions — Indians develop coronary artery disease a decade earlier than Western populations, and the prevalence is rising rapidly in urban and rural areas alike.

Figure: Ischaemic Heart Disease — When the Pipes Block (AN22.4)
The anatomical basis is straightforward: atherosclerosis — cholesterol-laden plaques build up inside the coronary artery walls (this is where Biochemistry's BI4 lipid metabolism connects). Over years, the plaque narrows the artery lumen. When the narrowing exceeds ~70%, the heart muscle downstream doesn't get enough oxygen during exertion (angina pectoris — chest pain on exercise). If the plaque ruptures and a blood clot forms on top of it, the artery blocks completely — this is a myocardial infarction (MI) — heart attack.
Which artery is blocked determines which part of the heart dies:
- LAD occlusion → anterior MI — the most dangerous ('widow-maker'). The anterior wall and septum are damaged. Can lead to cardiogenic shock, ventricular fibrillation, and death. The LAD supplies such a large territory that its complete blockage is often fatal.
- RCA occlusion → inferior MI — the inferior wall is damaged. May also damage the AV node (since RCA supplies it in 80% of people), causing heart block. Can also cause right ventricular infarction — the right ventricle fails, causing low blood pressure with distended neck veins.
- LCx occlusion → lateral MI — the lateral wall of the left ventricle is damaged. Less common than LAD or RCA occlusions but can be extensive in left-dominant hearts.
- Posterior MI (RCA territory in dominant hearts) — often missed on standard ECG because it's on the back of the heart. Always get a posterior ECG (leads V7–V9) if you suspect posterior MI.
Spiral forward: You'll study the ECG patterns for each MI territory in Physiology (PY5). The anatomy you're learning now — which artery feeds which territory — is the key to interpreting those ECG changes.
The Coronary Sinus — Venous Drainage of the Heart (AN22.5)
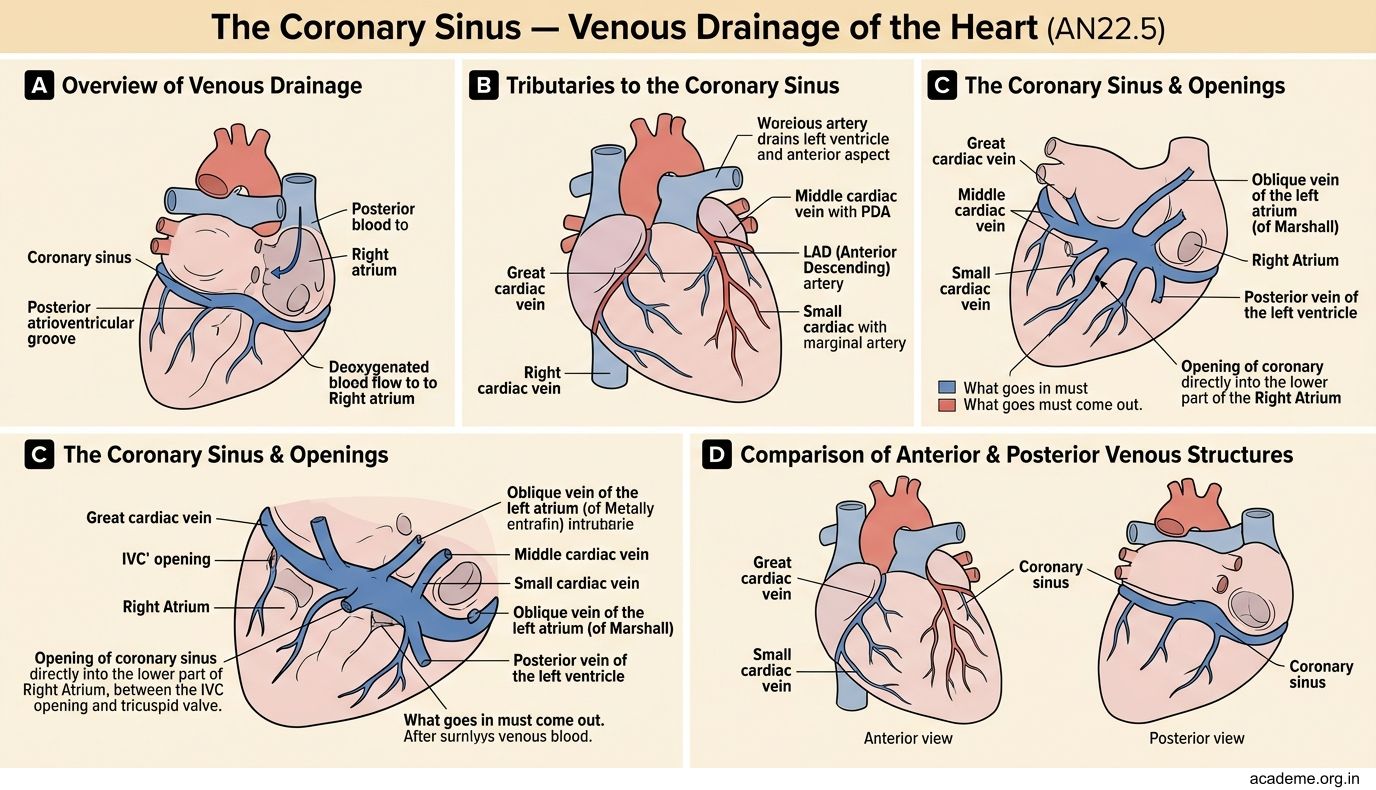
What goes in must come out — after supplying the heart muscle, deoxygenated blood needs to drain back. The main venous drainage of the heart is through the coronary sinus — a large venous channel that runs in the posterior atrioventricular groove and empties into the right atrium.

Figure: The Coronary Sinus — Venous Drainage of the Heart (AN22.5)
The coronary sinus receives several tributaries:
- Great cardiac vein — runs alongside the LAD in the anterior interventricular groove, then curves left to join the coronary sinus. Drains the territories supplied by the LAD and LCx.
- Middle cardiac vein — runs alongside the posterior descending artery in the posterior interventricular groove. Drains the inferior wall.
- Small cardiac vein — runs alongside the RCA (in the right atrioventricular groove). Drains the right atrium and right ventricle.
- Posterior vein of the left ventricle — drains the posterior surface of the left ventricle
- Oblique vein of the left atrium (of Marshall) — a small vein on the posterior left atrium (remnant of the left superior vena cava)
Additional venous drainage:
• Anterior cardiac veins — 3–4 small veins that drain the anterior right ventricle and empty directly into the right atrium (they bypass the coronary sinus)
• Venae cordis minimae (Thebesian veins) — tiny veins that drain directly into all four chambers. These are the heart's private drainage system.
Key point: Almost all cardiac venous blood ultimately reaches the right atrium — either through the coronary sinus or directly through the anterior cardiac veins and Thebesian veins.
The Conducting System — The Heart's Own Pacemaker (AN22.7)
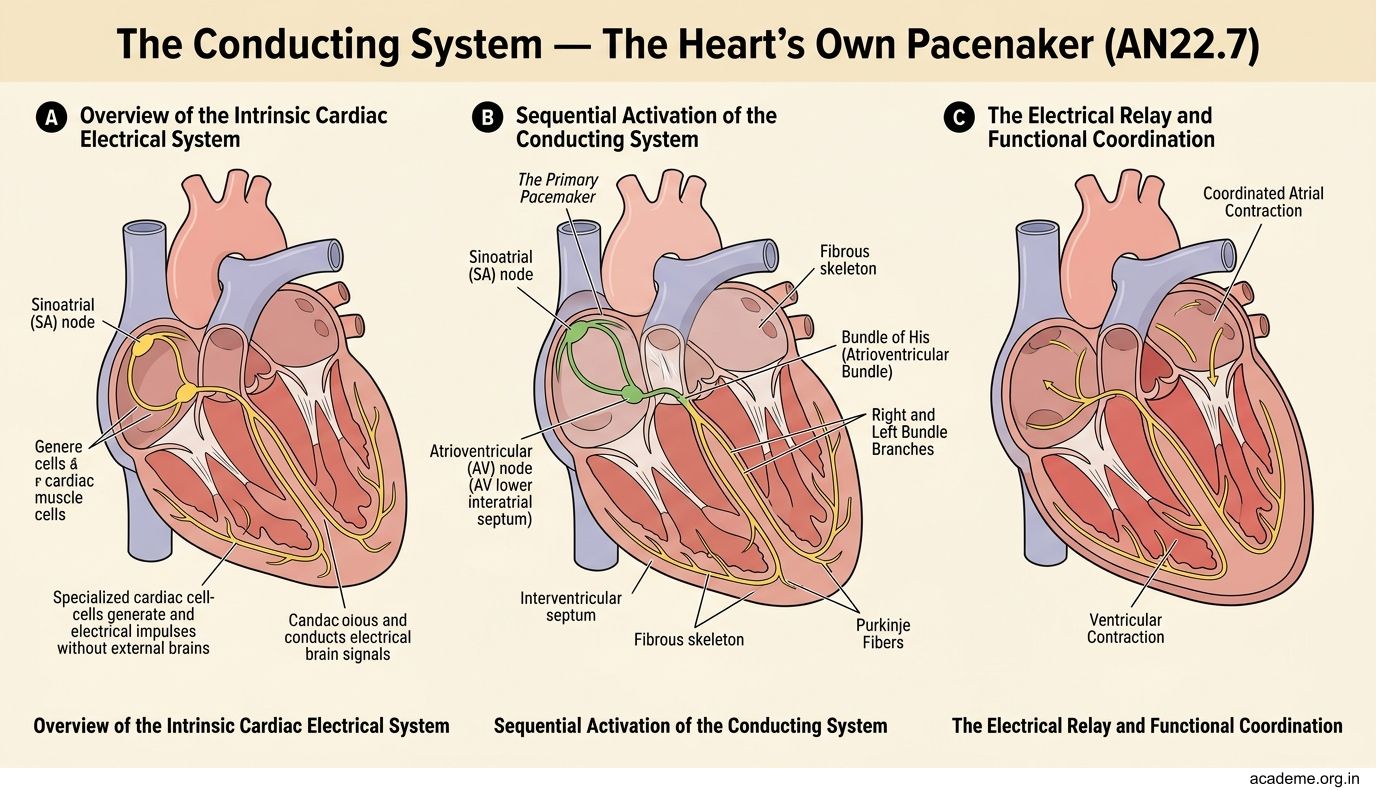
Here's something that amazes students: the heart has its own built-in electrical system. It doesn't need the brain to beat — a transplanted heart (with all its nerves cut) still beats rhythmically. This is because of the conducting system — specialised cardiac muscle cells that generate and conduct electrical impulses.
The conducting system works in sequence, like a relay race:
1. Sinoatrial (SA) node — the heart's natural pacemaker. Located in the right atrium, at the junction of the SVC and the right auricle (near the crista terminalis). It generates impulses at 60–100 beats per minute. The SA node sets the heart rate.
- Blood supply: SA nodal artery — from the RCA (60%) or LCx (40%)
- Interatrial pathways — the impulse spreads through the atrial muscle, causing both atria to contract (atrial systole). Three internodal tracts (anterior, middle, posterior) carry the impulse preferentially to the AV node.
3. Atrioventricular (AV) node — located in the interatrial septum, just above the tricuspid valve (in the triangle of Koch — bounded by the coronary sinus, tendon of Todaro, and tricuspid annulus). The AV node has a critical function: it delays the impulse by about 0.1 seconds. This delay ensures the atria finish contracting before the ventricles begin — allowing complete ventricular filling.
- Blood supply: AV nodal artery — from the RCA (80%) or LCx (20%)
- Intrinsic rate: 40–60 bpm (if the SA node fails, the AV node takes over as a backup pacemaker)
4. Bundle of His — the only electrical pathway through the fibrous skeleton (remember: the fibrous skeleton insulates atria from ventricles). The bundle passes through the membranous part of the interventricular septum and immediately divides into:
- Right bundle branch — travels along the right side of the septum, reaches the anterior papillary muscle via the moderator band (septomarginal trabecula)
- Left bundle branch — divides into anterior and posterior fascicles, spreads across the left side of the septum
- Purkinje fibres — the terminal network that distributes the impulse rapidly across the ventricular myocardium, from endocardium (inside) to epicardium (outside). This ensures both ventricles contract almost simultaneously.
The complete sequence: SA node → atrial muscle → AV node (delay) → Bundle of His → right and left bundle branches → Purkinje fibres → ventricular muscle (ventricular systole)
The key concept: The SA node is the pacemaker, the AV node is the gatekeeper (with its crucial delay), and the His-Purkinje system is the rapid distribution network.
SELF-CHECK
A patient with an inferior MI (RCA occlusion) develops a very slow heart rate (35 bpm). Which part of the conducting system is most likely damaged, and why is the RCA responsible?
A. SA node; the RCA supplies the SA node in all hearts
B. AV node; the RCA supplies the AV node in approximately 80% of hearts
C. Bundle of His; the RCA is the sole supply to the interventricular septum
D. Purkinje fibres; the RCA supplies the ventricular endocardium
Reveal Answer
Answer: B. AV node; the RCA supplies the AV node in approximately 80% of hearts
The AV node is supplied by the AV nodal artery, which arises from the RCA in approximately 80% of hearts. An inferior MI (RCA occlusion) can therefore damage the AV node, causing heart block — the impulse from the atria cannot reach the ventricles properly, resulting in a dangerously slow heart rate. This is why inferior MIs are often associated with bradycardia.
CLINICAL PEARL
The 'widow-maker': Complete occlusion of the LAD artery (especially its proximal segment before the first diagonal branch) is nicknamed the 'widow-maker' because it supplies such a large territory — the entire anterior wall, the apex, and the anterior 2/3 of the septum. Sudden LAD occlusion causes massive anterior MI, often leading to ventricular fibrillation and sudden cardiac death. In India, where the 'golden hour' for reaching a catheterisation lab is often missed due to distance and delay, LAD occlusions are disproportionately fatal compared to Western countries. This is why the government's push for primary PCI centres (percutaneous coronary intervention — opening the blocked artery with a stent) in district hospitals is so critical. Every minute of delay in opening a blocked LAD costs myocardium — time is muscle.