Page 2 of 7
AN25.1-9 | Thorax — SDL Guide (Part 2)
Thoracic Inlet, Outlet, and Imaging (AN25.5, AN25.6)
Thoracic Inlet (Superior Thoracic Aperture):
- Bounded by: T1 body (posterior), first rib (lateral), manubrium (anterior)
- Structures passing through: trachea, oesophagus, subclavian vessels, brachial plexus, thoracic duct, phrenic nerves, vagus nerves, sympathetic chains, internal thoracic arteries
- Thoracic outlet syndrome: compression of brachial plexus (lower trunk, C8–T1) and/or subclavian vessels at the inlet by a cervical rib, tight scalene muscles, or Pancoast tumour

Figure: Thoracic Inlet, Outlet, and Imaging (AN25.5, AN25.6)
Thoracic Outlet (Inferior Thoracic Aperture):
- Bounded by: T12 (posterior), 12th rib (lateral), costal margin (11th and 12th ribs + costal cartilages), xiphoid (anterior)
- Closed by the diaphragm
Thoracic Imaging (AN25.6) — CXR anatomy:
Key structures to identify on PA CXR:
1. Trachea: midline, slight rightward deviation at aortic arch — widened carina suggests subcarinal nodes
2. Right hilum: lower than left; formed mainly by the right pulmonary artery (upper) and lower lobe pulmonary vein (lower)
3. Left hilum: higher than right (left PA arches over left bronchus)
4. Cardiac silhouette: right border = SVC (upper) + RA (lower); left border = aortic knuckle + PA (upper) + left atrial appendage + LV (lower)
5. Costophrenic angles: should be acute; blunted = effusion (>200–300 mL)
6. Lung markings: bronchovascular markings taper toward periphery
7. Bones: ribs (count by the posterior angle), vertebrae, clavicles, scapulae
Rib counting on CXR: Start from the manubrium (1st rib/costal cartilage junction is at the manubrium upper border); or identify 12th rib posteriorly and count up.
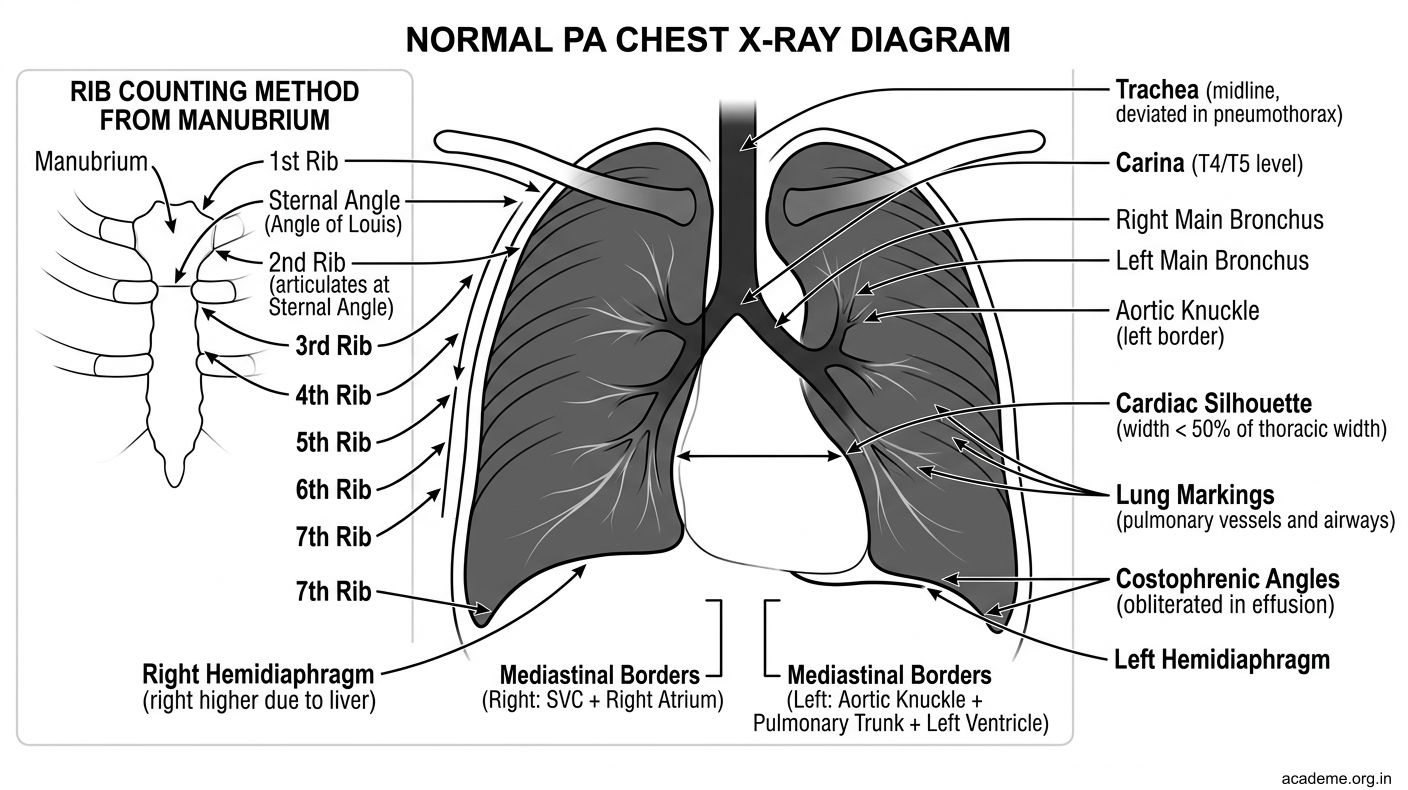
Figure: Thoracic Imaging (AN25.6) — CXR anatomy:
SELF-CHECK
A. Aorta and thoracic duct
B. Oesophagus and vagal trunks
C. Inferior vena cava and right phrenic nerve
D. Left phrenic nerve and lymphatic vessels
Reveal Answer
Answer: see explanation below
The caval opening at T8 transmits the IVC and right phrenic nerve. The IVC opening is in the central tendon — this is important because the IVC (a thin-walled vessel) needs the non-contractile central tendon around it to stay open during inspiration.
Anomalies, Surface Markings, and Clinical Applications (AN25.7, AN25.8, AN25.9)
Common Thoracic Cage Anomalies (AN25.7):
| Anomaly | Description | Clinical Significance |
|---|---|---|
| Cervical rib | Extra rib from C7 | Thoracic outlet syndrome (brachial plexus + subclavian compression) |
| Pectus excavatum | Funnel chest — sternum depressed | Cardiopulmonary compromise; cosmetic |
| Pectus carinatum | Pigeon chest — sternum protrudes | Associated with Marfan syndrome |
| Bifid rib | Rib divided anteriorly | Usually incidental on CXR |
| Rib notching | Scalloping of inferior rib borders | Coarctation of aorta (enlarged collateral intercostal arteries) |
Surface Markings of Thoracic Viscera (AN25.8):
Heart borders (on chest wall):
- Upper right: 3rd right costal cartilage, 1.5 cm from sternum
- Lower right: 6th right costal cartilage, 1.5 cm from sternum (RA)
- Lower left: 5th left intercostal space, midclavicular line (apex — LV)
- Upper left: 2nd left costal cartilage, 1.5 cm from sternum (PA trunk)
- Cardiac apex = site of apex beat (maximum impulse) — normally 5th ICS MCL
Lung and pleural borders: (see Lungs module)
Key surface markings:
- Right cardiophrenic angle: overlies inferior vena cava + right phrenic nerve
- Liver dullness: below 5th right ICS (MCL) — if dullness is higher, hepatomegaly; if tympany, pneumoperitoneum
- Spleen dullness: between 9th–11th ribs, posterior axillary line
Clinical Applications (AN25.9):
- Flail chest: 3+ consecutive ribs fractured at 2 sites → paradoxical movement (segment moves in on inspiration) → ineffective ventilation → emergency
- Rib fractures: most common at the rib angle (posterior); complications = pneumothorax, haemothorax, pulmonary contusion
- Intercostal nerve block: inject 0.5% bupivacaine at costal groove — useful for multiple rib fractures
- Needle thoracostomy: 2nd ICS MCL for tension pneumothorax (emergency decompression)
- Heimlich manoeuvre: uses the air trapped behind a foreign body — sharp upward thrust below the costal margin compresses the diaphragm
- CPR: compressions applied over the lower sternum → compress the heart between sternum and vertebral column
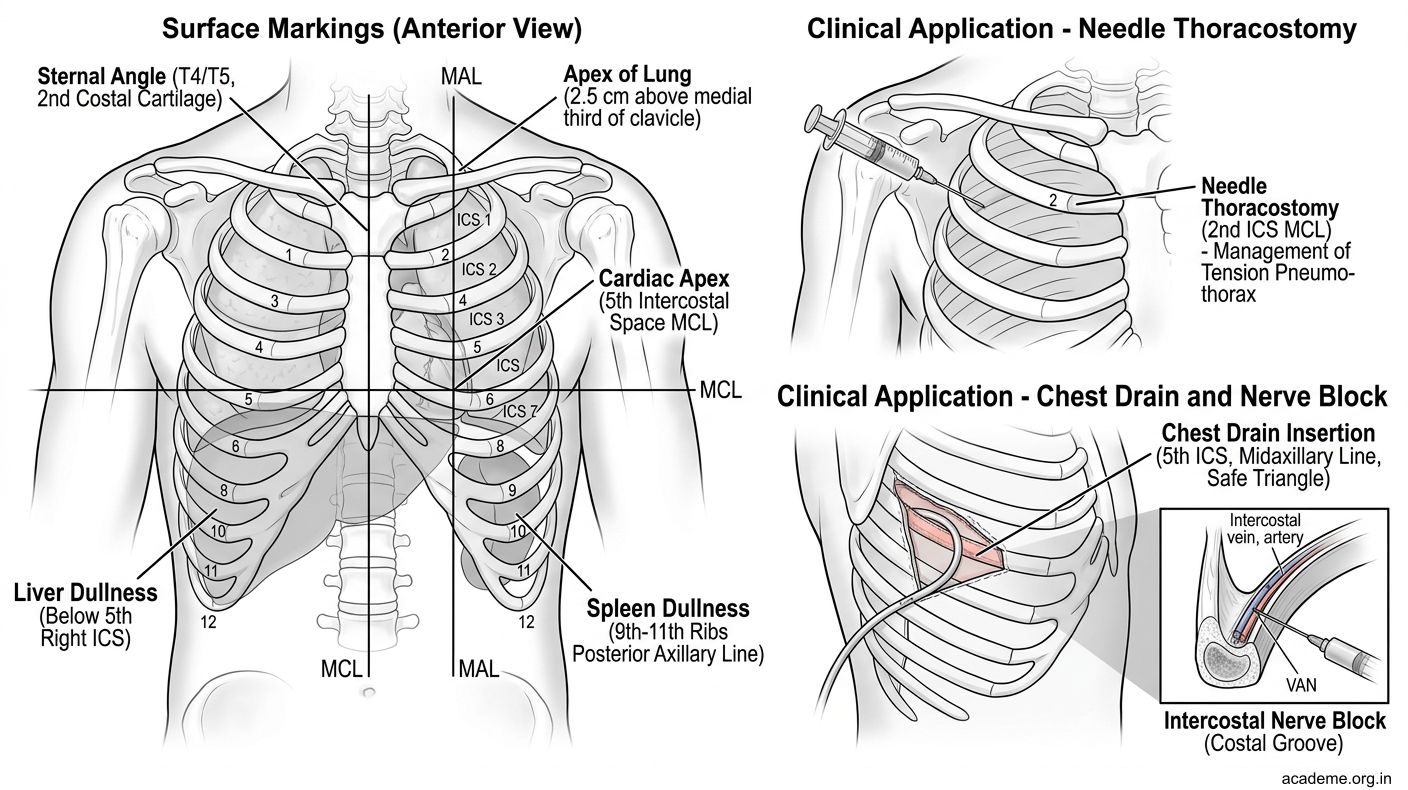
Figure: Anomalies, Surface Markings, and Clinical Applications (AN25.7, AN25.8, AN25.9)
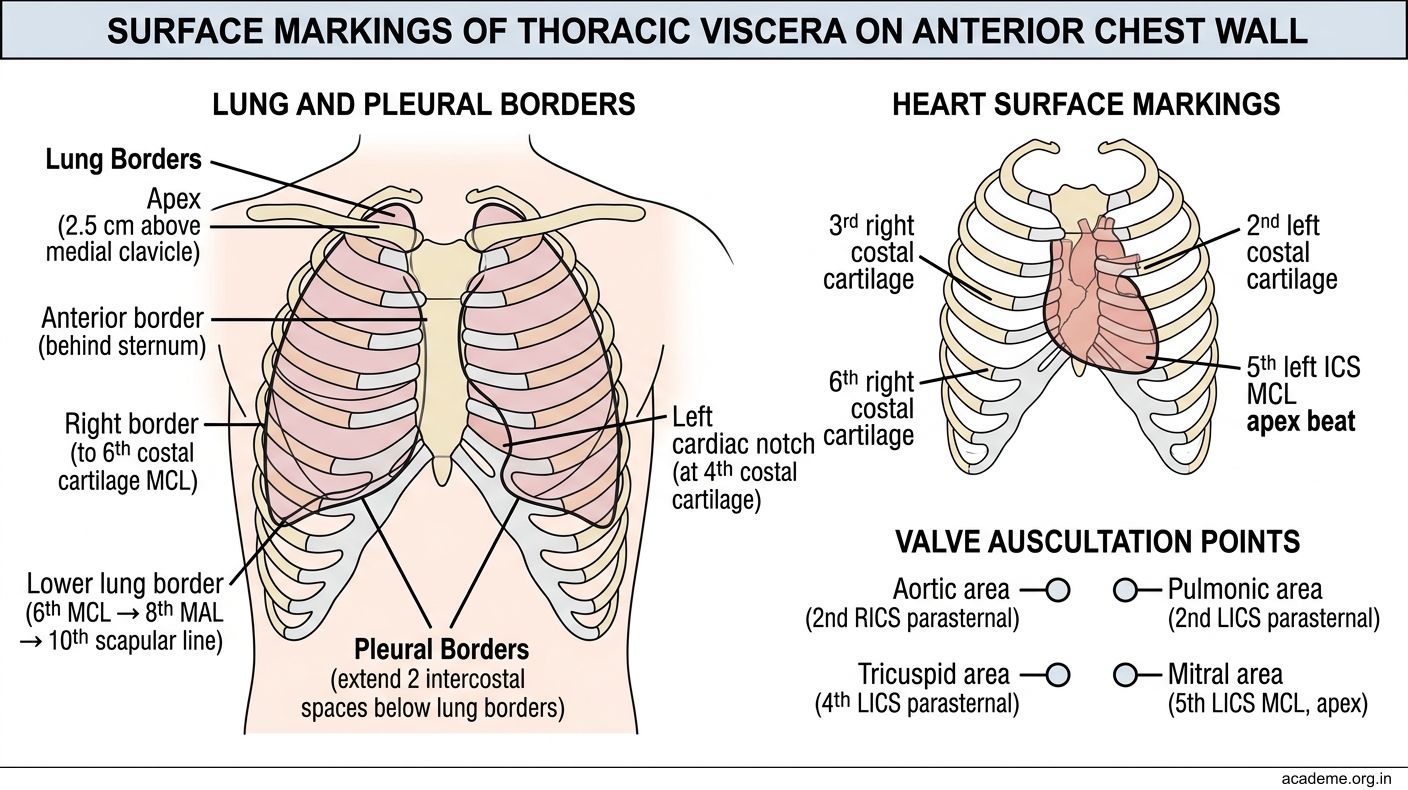
Figure: Surface Markings of Thoracic Viscera (AN25.8):
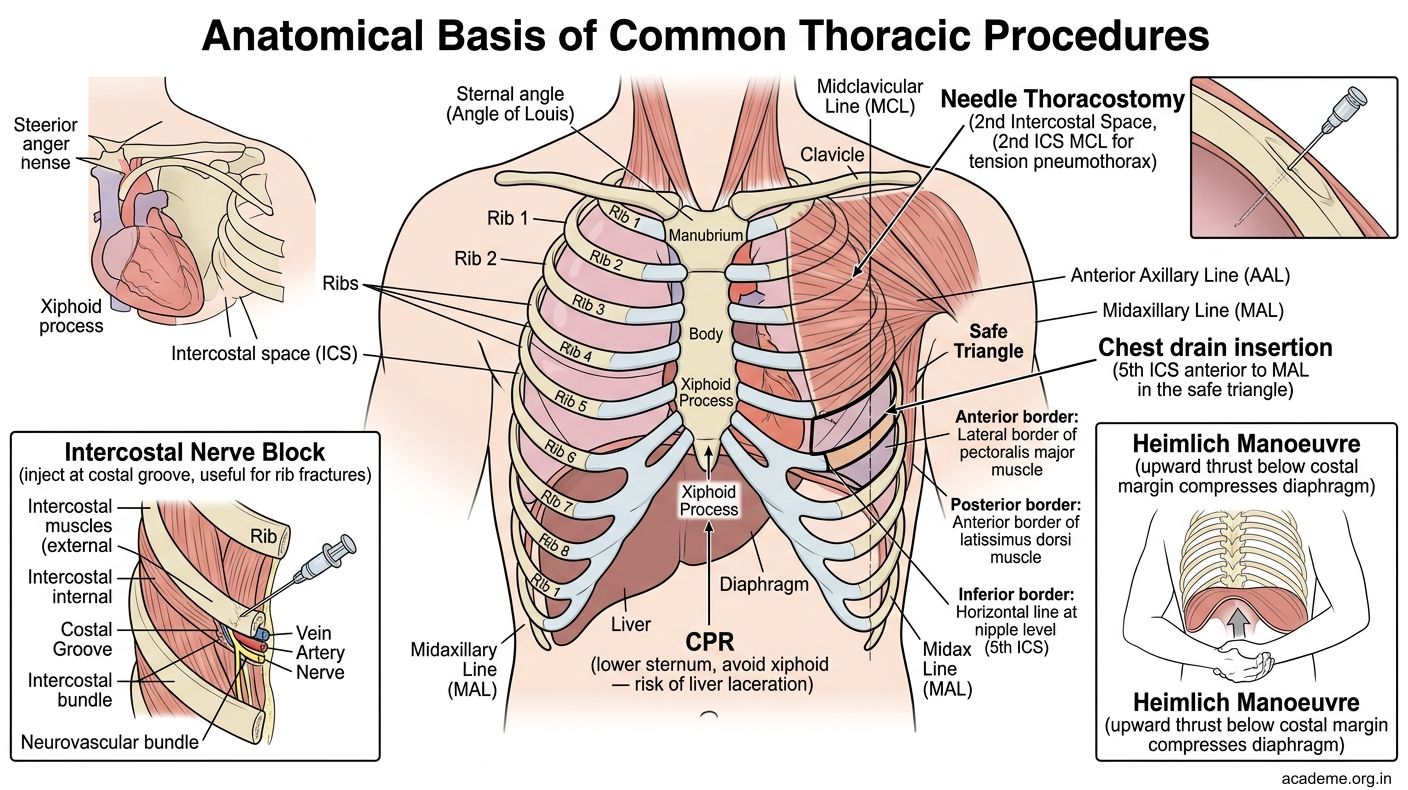
Figure: Clinical Applications (AN25.9):
SELF-CHECK
A. Pulmonary hypertension
B. Coarctation of the aorta
C. Atrial septal defect
D. Pericardial effusion
Reveal Answer
Answer: see explanation below
In coarctation of the aorta, enlarged collateral intercostal arteries (bypassing the obstruction) erode the inferior surface of the ribs, creating the classic "rib notching" appearance on CXR, typically affecting ribs 3–8.
CLINICAL PEARL
Cervical rib is present in 0.5% of the population. It arises from C7 and can be a complete bony rib or a fibrous band. It causes thoracic outlet syndrome — compression of the lower trunk of the brachial plexus (C8, T1) → wasting of the small muscles of the hand + ulnar border pain + weakness. The subclavian artery can also be compressed → reduced radial pulse on the affected side (positive Adson's test). On CXR, look for a bony opacity just above the first rib on the symptomatic side.