Page 2 of 7
AN31.1-5 | Orbit — SDL Guide (Part 2)
Lacrimal Apparatus (AN31.4)
The lacrimal apparatus produces and drains tears, maintaining corneal hydration and protection.

Figure: Lacrimal Apparatus (AN31.4)
Components (production to drainage):
1. Lacrimal gland — almond-shaped; located in the lacrimal fossa in the superolateral orbital roof (frontal bone). Divided by the LPS aponeurosis into:
- Orbital lobe (larger, superior)
- Palpebral lobe (smaller, inferior — visible when upper lid is everted)
Secretomotor nerve supply: Parasympathetic fibres from CN VII (facial nerve) → greater petrosal nerve → pterygoid canal → pterygopalatine ganglion → relay → zygomatic nerve → lacrimal nerve → lacrimal gland
(Mnemonic: "Greater Petrosal Takes Tear information" — Greater Petrosal → Tears)
2. Lacrimal canaliculi — superior and inferior; drain tears from the lacrimal puncta (small openings at the medial end of each eyelid) → unite to form the common canaliculus → drain into the lacrimal sac
3. Lacrimal sac — lies in the lacrimal groove (formed by lacrimal bone and frontal process of maxilla); superior to the medial canthal tendon. Clinically: dacryocystitis (infection/inflammation of the lacrimal sac) presents as painful swelling at the medial canthus — common in post-traumatic medial orbital wall fractures.
4. Nasolacrimal duct — descends ~12 mm within the bony nasolacrimal canal → opens into the inferior meatus of the nasal cavity, just behind the anterior end of the inferior turbinate
- A small mucosal fold (Hasner's valve) at the opening may fail to open at birth → congenital nasolacrimal duct obstruction (epiphora in neonates — most common cause of watering eye in Indian infants; managed by syringing/probing)
Tear film layers (clinical relevance for optometry/ophthalmology):
1. Outer lipid layer — meibomian glands
2. Middle aqueous layer — lacrimal gland
3. Inner mucin layer — goblet cells of conjunctiva
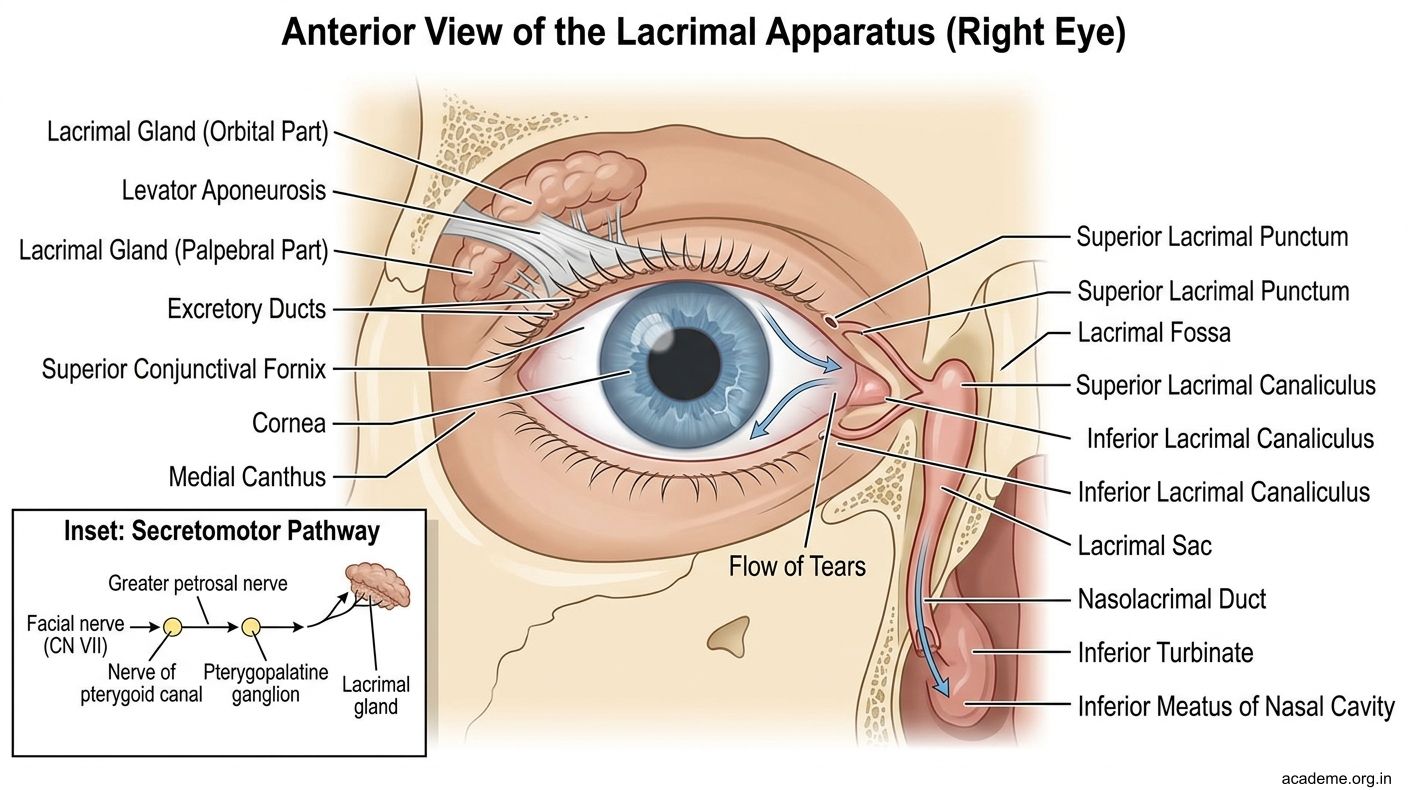
Figure: Lacrimal Apparatus (AN31.4)

Figure: Components (production to drainage):
Nerve Palsies and Strabismus — Anatomical Basis (AN31.5)
Strabismus (squint) is misalignment of the visual axes. Understanding which muscle and nerve is affected is clinically essential.
Oculomotor (CN III) Palsy:
Complete CN III palsy produces:
- Ptosis (complete — LPS fully denervated)
- Eye deviated "down and out" — lateral rectus (CN VI) pulls laterally; superior oblique (CN IV) pulls the eye down and rotates it; no medial, superior, or inferior movement possible
- Fixed dilated pupil — parasympathetic fibres to sphincter pupillae travel on the surface of CN III and are the first to be compressed in surgical CN III palsy (e.g., posterior communicating artery aneurysm, uncal herniation)
- Diplopia (relieved by the ptosis covering the eye)
Medical vs Surgical CN III palsy:
- Surgical (compressive) — pupil involved; aneurysm until proved otherwise; emergency imaging
- Medical (ischaemic — e.g., diabetes, hypertension) — pupil typically spared (microvascular disease affects core fibres first; parasympathetic fibres on the surface are relatively spared)
Trochlear (CN IV) Palsy:
- Longest intracranial course; most commonly injured in closed head trauma (wraps around the midbrain)
- Inability to depress the adducted eye → diplopia on looking down (reading, descending stairs)
- Head tilt to the opposite side and chin depression — a classic compensation
- Parks-Bielschowsky 3-step test is used to localise the affected muscle
Abducent (CN VI) Palsy:
- Lateral rectus paralysis → eye deviated medially (esotropia)
- Diplopia on lateral gaze toward the affected side
- CN VI has a long intracranial course over the petrous apex — vulnerable in raised intracranial pressure, petrous fractures, Gradenigo's syndrome (petrous apicitis from otitis media — triad: ipsilateral CN VI palsy, facial pain, otorrhoea)
Combined Palsies — Cavernous Sinus Syndrome:
All three motor nerves (CN III, IV, VI) plus V1 and V2 pass through or adjoin the cavernous sinus. Combined ophthalmoplegia with facial pain and proptosis = cavernous sinus pathology (thrombosis, fistula, aneurysm, tumour).

Figure: Nerve Palsies and Strabismus — Anatomical Basis (AN31.5)

Figure: The Pupil in CN III Palsy is the Emergency Clue
SELF-CHECK — : Orbit
A patient presents with complete ptosis, a dilated fixed pupil, and the eye deviating down and out. Which nerve is most likely affected?
A. CN IV (Trochlear)
B. CN VI (Abducent)
C. CN III (Oculomotor)
D. CN V1 (Ophthalmic)
Reveal Answer
Answer: C. CN III (Oculomotor)
Horner's syndrome (ptosis + miosis + anhidrosis) results from interruption of which pathway?
A. Parasympathetic supply to the iris
B. Sympathetic oculomotor pathway
C. Optic nerve pathway
D. Facial nerve secretomotor pathway
Reveal Answer
Answer: B. Sympathetic oculomotor pathway
Tears drain from the lacrimal sac into the nasal cavity through the nasolacrimal duct, which opens into the:
A. Superior meatus
B. Middle meatus
C. Inferior meatus
D. Sphenoethmoidal recess
Reveal Answer
Answer: C. Inferior meatus
CLINICAL PEARL
The Pupil in CN III Palsy is the Emergency Clue
A new-onset CN III palsy with a dilated, non-reactive pupil is a neurosurgical emergency until a posterior communicating artery aneurysm is excluded. Parasympathetic fibres travelling on the surface of CN III are compressed first by an expanding aneurysm. Do NOT wait for imaging results before alerting the neurosurgery team. In contrast, a diabetic CN III palsy (microvascular ischaemia) typically spares the pupil and resolves over 3 months.
This distinction — pupil-involved vs pupil-spared — is one of the most important clinical algorithms you will learn.