Page 1 of 4
AN34.1-3 | Submandibular region — SDL Guide
Learning Objectives
- Describe and demonstrate the superficial and deep structures, muscles, nerves, vessels, and glands in the submandibular region (AN34.1)
- Describe and demonstrate the morphology, relations, and nerve supply of the submandibular salivary gland and submandibular ganglion (AN34.2)
- Describe the basis of formation of submandibular stones (sialolithiasis) (AN34.3)
INSTRUCTIONS
Focus on the three-dimensional relationship of structures in the floor of the mouth and submandibular triangle. Understand the duct drainage and stone formation.
References
- Gray's Anatomy for Students — Submandibular Region and Floor of Mouth (Textbook)
- BD Chaurasia's Human Anatomy Vol. 3 — Oral Cavity (Textbook)
- Oral and Maxillofacial Surgery — Salivary Gland Disease (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 45-year-old man from a rural area near Chennai presents with pain and swelling under his jaw that gets dramatically worse every time he eats. He says the swelling appears suddenly at mealtimes and gradually subsides over the next hour. On examination, a firm, non-tender swelling is palpable bimanually in the floor of the mouth.
What structure is obstructed? Why does the swelling worsen at mealtimes? What is the likely diagnosis? What predisposes to this condition?
By the end of this module, you will be able to answer all of these questions and understand the complete anatomy of the submandibular region.
WHY THIS MATTERS
The submandibular region is clinically important in everyday practice in India:
- Submandibular salivary stones (sialolithiasis) — 80% of all salivary stones occur in the submandibular gland (Wharton's duct); presenting with meal-time swelling
- Ludwig's angina — a rapidly spreading cellulitis of the floor of the mouth; originates from lower molar infections; can cause airway obstruction and death; a surgical emergency
- Submandibular lymphadenopathy — common in tuberculosis (scrofula), dental infections, and metastatic oral cancer
- Submandibular gland excision — common procedure in ENT/maxillofacial surgery; requires detailed knowledge of the lingual nerve and hypoglossal nerve relationships
- Ranula — a retention cyst of the sublingual gland; presents as a translucent swelling in the floor of the mouth
RECALL
Before we begin, recall:
- The mylohyoid muscle separates the sublingual space (above) from the submandibular space (below)
- The lingual nerve (branch of CN V3) carries general sensation from the anterior 2/3 of the tongue + carries taste fibres (from chorda tympani, CN VII) to the anterior tongue
- The hypoglossal nerve (CN XII) supplies all intrinsic and extrinsic tongue muscles (except palatoglossus — CN X)
- The submandibular gland is the second largest salivary gland; its duct (Wharton's duct) opens beside the frenulum of the tongue
Submandibular Region — Structures, Muscles, Nerves, and Vessels (AN34.1)
Floor of the Mouth — Layers:

Figure: Submandibular Region — Structures, Muscles, Nerves, and Vessels (AN34.1)
Superficial to deep:
1. Skin → platysma → investing fascia
2. Superficial muscles:
- Anterior belly of digastric — from mental symphysis → intermediate tendon (attached to hyoid via fascial sling)
- Mylohyoid — the principal muscle forming the floor of the mouth; from the mylohyoid line of the mandible → median fibrous raphe + hyoid body; acts as a muscular diaphragm separating the submandibular space (below) from the sublingual space (above)
3. Deep to mylohyoid (sublingual space):
- Sublingual gland (anterolateral)
- Deep part of the submandibular gland and Wharton's duct (wrapping around mylohyoid's posterior border)
- Lingual nerve (medial to the duct)
- Hypoglossal nerve (CN XII) (runs on the hyoglossus)
- Lingual artery and vein (deep to hyoglossus)
4. Hyoglossus — deeper layer; from hyoid body and greater horn → side of tongue
Nerve relationships in the floor of the mouth (Mnemonic: "Lingual Nerve → Whips Down And Under"):
- The lingual nerve first passes lateral to, then beneath, then medial to Wharton's duct — it crosses the duct twice:
1. First crossing: lingual nerve is lateral and superior to the duct at the posterior floor
2. Second crossing: lingual nerve passes under the duct (medially) at the anterior floor near the sublingual gland
This double crossing means the lingual nerve is at risk of injury during submandibular duct stone extraction and gland excision.
Vessels:
- Lingual artery — from ECA; passes deep to hyoglossus; branches: dorsal lingual, sublingual, deep lingual (profunda linguae) arteries
- Facial artery — arises from ECA; hooks under the posterior belly of digastric; grooves the submandibular gland posteriorly; crosses the mandible at masseter anterior border → continues on face
- Submental artery — branch of facial artery in the submandibular region
- Lingual vein — drains into the internal jugular vein (or common facial vein)
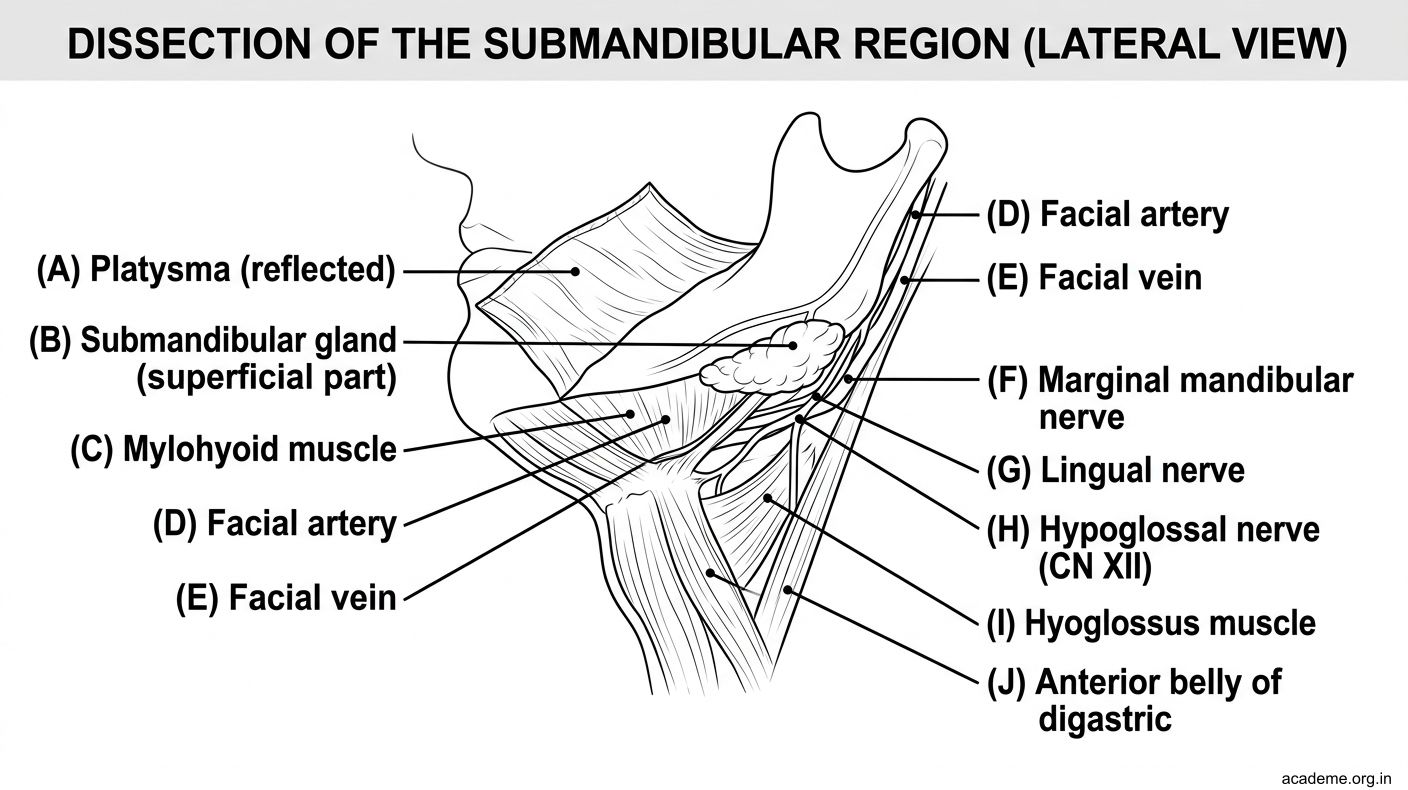
Figure: Submandibular Region — Structures, Muscles, Nerves, and Vessels (AN34.1)
Submandibular Gland and Ganglion (AN34.2)
Submandibular Gland — Morphology:

Figure: Submandibular Gland and Ganglion (AN34.2)
The submandibular gland is a mixed (seromucous) salivary gland — largest predominantly serous of the major glands (parotid is purely serous; sublingual is predominantly mucous). It produces ~70% of the resting salivary volume.
Shape: J-shaped; wraps around the posterior border of the mylohyoid muscle.
Parts:
1. Superficial part (larger) — lies below the mylohyoid; occupies the digastric/submandibular triangle; bounded above by mandible, below by anterior/posterior bellies of digastric, medially by hyoglossus and mylohyoid
2. Deep part (smaller) — lies above the mylohyoid; projects into the sublingual space; continuous with the superficial part around the posterior free border of mylohyoid
Wharton's Duct (submandibular duct):
- 5 cm long
- Emerges from the medial surface of the deep part of the gland
- Runs forward on the hyoglossus → then on the genioglossus
- Opens at the sublingual papilla (caruncula sublingualis) beside the frenulum of the tongue
- The duct has a long, tortuous course that runs upward and forward against gravity from gland to opening — this is the principal anatomical reason stones form (pooling, stasis)
Relations (clinically important):
- Lingual nerve hooks under the duct twice (as described above)
- Hypoglossal nerve runs between the duct and the hyoglossus, deep to the superficial part of the gland — at risk during gland excision
- Facial artery grooves or pierces the posterior surface of the gland
Blood supply: Facial and lingual arteries.
Venous drainage: Facial and lingual veins → internal jugular vein.
Submandibular Ganglion:
- Parasympathetic ganglion suspended from the lingual nerve by two roots
- Location: Medial surface of the deep part of the gland, on the hyoglossus
- Preganglionic parasympathetic input: CN VII → chorda tympani → joins lingual nerve (CN V3) → submandibular ganglion
- Postganglionic fibres: Supply submandibular gland (directly) and sublingual gland (via lingual nerve branches)
- Sympathetic fibres: Pass through without synapsing (from superior cervical ganglion via facial artery plexus) — vasoconstriction
- Sensory fibres: CN V3 via lingual nerve — pass through without synapsing
Sublingual Gland:
- Smallest of the three major salivary glands
- Location: Floor of the mouth, above mylohyoid, below the mucous membrane of the mouth
- Predominantly mucous
- Multiple small ducts (ducts of Rivinus) open directly into the floor of the mouth along the sublingual fold
- Some ducts join Wharton's duct
- No single main duct (unlike parotid and submandibular)
- Ranula — a mucous retention cyst of the sublingual gland; presents as a translucent blue swelling in the floor of the mouth (resembles a frog's belly — rana = frog in Latin)
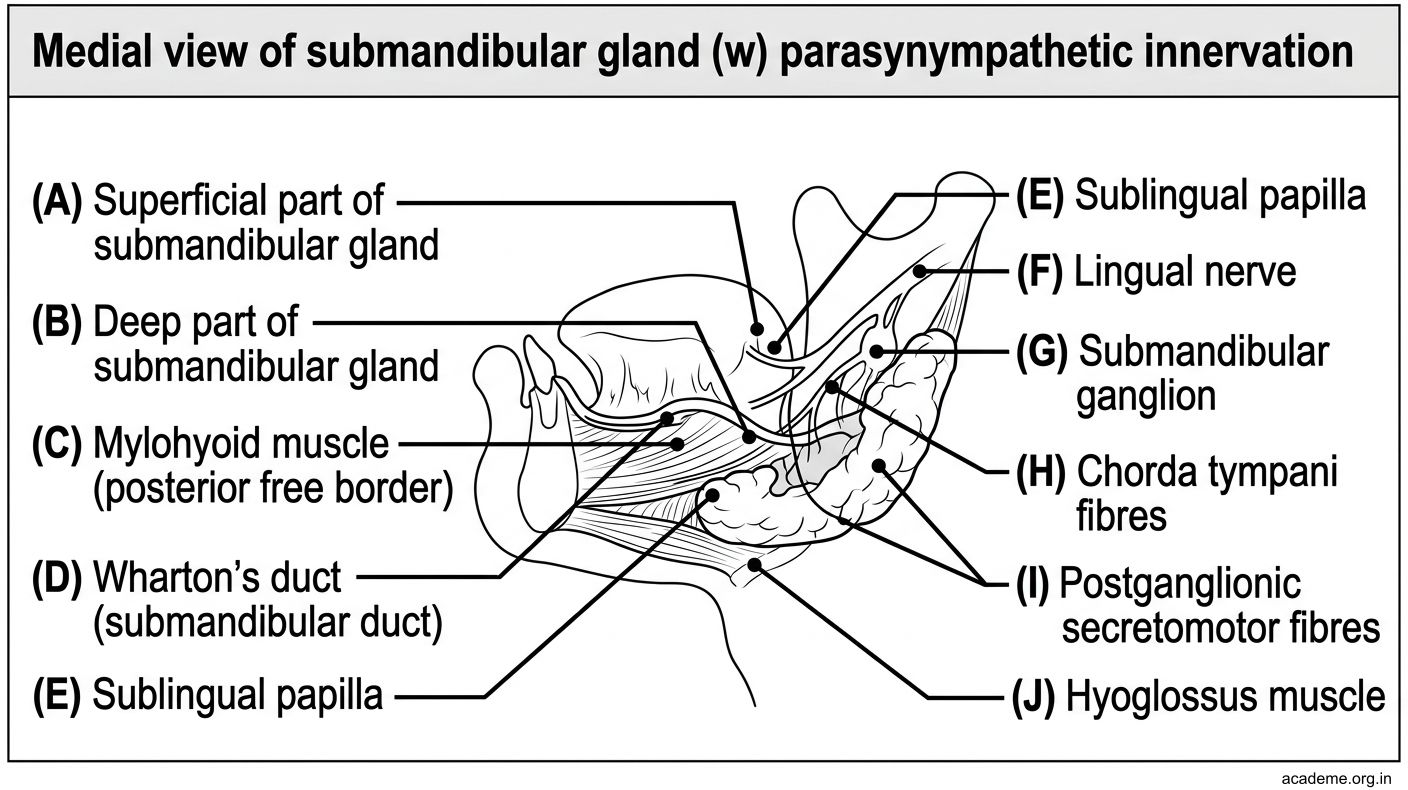
Figure: Submandibular Gland and Ganglion (AN34.2)
Submandibular Stones — Basis of Formation (AN34.3)
Sialolithiasis (Salivary Gland Stones)
Epidemiology:
- 80–90% of salivary calculi occur in the submandibular gland/duct
- Only ~5–10% in the parotid; rare in sublingual
Why does the submandibular gland form stones so much more frequently?
Three anatomical and physiological reasons:
1. Duct characteristics — longest, most tortuous, runs AGAINST gravity:
- Wharton's duct (5 cm) is longer and more tortuous than the parotid (Stensen's) duct
- The duct runs upward and forward — saliva must flow uphill against gravity from the gland (in the floor of the neck) to the papilla (in the floor of the mouth)
- This creates stasis — saliva pools, allowing precipitation of calcium phosphate crystals
2. Saliva composition — more viscous, higher pH, more calcium:
- Submandibular saliva is more mucous than parotid saliva
- Higher pH (more alkaline) → calcium salts (calcium phosphate, calcium carbonate) are less soluble → easier precipitation
- Higher calcium concentration compared to parotid saliva
3. Wider ductal orifice — but narrower proximal segment:
- The duct narrows as it passes around the posterior border of mylohyoid — creating a natural point of relative obstruction
Mechanism of Stone Formation:
Retrograde contamination of bacteria + mucus glycoproteins form a nidus (organic matrix) around which calcium phosphate and calcium carbonate crystals precipitate → progressive calcification → stone (sialolith).
Clinical Features:
- Meal-time swelling and pain — eating stimulates saliva secretion; flow blocked by stone → gland distends
- Swelling subsides as saliva reabsorbs over ~1 hour
- Bimanual palpation: stone felt as hard, non-tender lump in the floor of mouth along the duct course
- Infection → submandibular abscess (if untreated)
Investigations: OPG (orthopantomogram) X-ray — most calculi are radio-opaque. Ultrasound or sialography for radiolucent stones.
Treatment:
- Anterior stones: intraoral stone removal (incising the duct, extracting the stone)
- Posterior stones (in the gland): submandibular gland excision
- Risks during excision: lingual nerve (double crossing of Wharton's duct), hypoglossal nerve (CN XII), marginal mandibular branch of facial nerve (CN VII — in the skin incision area)

Figure: Submandibular Stones — Basis of Formation (AN34.3)

Figure: Why does the submandibular gland form stones so much more frequently?

Figure: Submandibular Region — Key Points
SELF-CHECK — : Submandibular Region
The lingual nerve crosses Wharton's duct how many times in the floor of the mouth?
A. Once (from lateral to medial)
B. Twice (lateral → beneath → medial)
C. Three times
D. It does not cross the duct
Reveal Answer
Answer: B. Twice (lateral → beneath → medial)
Wharton's duct opens into the mouth at:
A. The parotid papilla (opposite upper second molar)
B. The sublingual fold laterally
C. The sublingual papilla (caruncula sublingualis) beside the frenulum
D. The posterior soft palate
Reveal Answer
Answer: C. The sublingual papilla (caruncula sublingualis) beside the frenulum
Why are 80% of salivary stones found in the submandibular gland/duct?
A. The gland secretes acidic saliva with low calcium
B. The duct is the widest, causing turbulent flow
C. The duct is tortuous, runs upward against gravity, and saliva is more mucous and alkaline
D. The gland is the largest and most active
Reveal Answer
Answer: C. The duct is tortuous, runs upward against gravity, and saliva is more mucous and alkaline
CLINICAL PEARL
Ludwig's Angina — Anatomy is the Key to Understanding Spread
Ludwig's angina is a rapidly spreading cellulitis involving the submandibular, sublingual, and submental spaces bilaterally. It typically originates from a lower second or third molar periapical abscess.
Why does it spread so rapidly? The mylohyoid muscle is the floor separating the sublingual (above) from the submandibular (below) space. Once infection crosses the mylohyoid (via fascial connections at its posterior border), it spreads rapidly across three bilaterally symmetric spaces simultaneously.
The danger: Oedema and induration elevate and push the tongue posteriorly and superiorly → airway obstruction. This is the cause of death — not sepsis itself.
Management: Secure the airway FIRST (awake fiberoptic intubation or surgical airway), then broad-spectrum IV antibiotics, then surgical drainage. In Indian hospitals with limited resources, the airway must be anticipated and secured early before any intervention.
This is one of the few true surgical emergencies of the head and neck.
REFLECT
During a submandibular gland excision, the surgeon needs to protect three nerves. Name them. For each, describe its location relative to the gland/duct, what deficits will occur if damaged, and a specific anatomical step to protect it.
KEY TAKEAWAYS
Submandibular Region — Key Points
- Mylohyoid: muscular floor of mouth; separates sublingual (above) from submandibular (below) space.
- Submandibular gland: J-shaped; wraps around mylohyoid's posterior border; superficial part in digastric triangle; deep part in sublingual space.
- Wharton's duct: 5 cm; runs uphill from gland → sublingual papilla; lingual nerve crosses it TWICE.
- Submandibular ganglion: CN VII (chorda tympani via lingual nerve) → parasympathetic supply to submandibular + sublingual glands.
- Sialolithiasis: 80% in submandibular — due to tortuous upward-running duct + mucous/alkaline/calcium-rich saliva.
- Nerves at risk in submandibular surgery: Marginal mandibular branch (CN VII) in skin incision; lingual nerve (CN V3) — crosses duct twice; hypoglossal nerve (CN XII) — deep on hyoglossus.
- Ludwig's angina: Bilateral 3-space cellulitis; airway emergency; lower molar origin.