Page 2 of 7
AN4.1-5 | General features of skin and fascia — SDL Guide (Part 2)
What Lies Beneath — Superficial Fascia (AN4.3)
Beneath the skin lies a layer of loose connective tissue called superficial fascia (also called the hypodermis or subcutaneous tissue). Think of it as the body's packing material — it fills the space between the skin and the structures beneath.
What's inside superficial fascia?
- Fat (adipose tissue) — its main component. The amount varies enormously by body region:
- Thick over the abdomen, buttocks, and thighs (energy storage)
- Thin over the back of the hand and eyelids (these need to stay flexible)
- Absent over the nipple, penis, and scrotum
- In women, fat in the breast (mammary gland) is embedded in superficial fascia
- Cutaneous nerves — nerves that supply the skin travel through this layer
- Superficial veins — the veins you can see through your skin (like the veins on the back of your hand) run in superficial fascia
- Cutaneous lymphatics — lymph vessels that drain the skin
Clinical connection: When a nurse gives a subcutaneous injection (like an insulin injection), the needle goes into superficial fascia. The fat in this layer absorbs the drug slowly, which is why subcutaneous injections are used for medications that need gradual absorption.
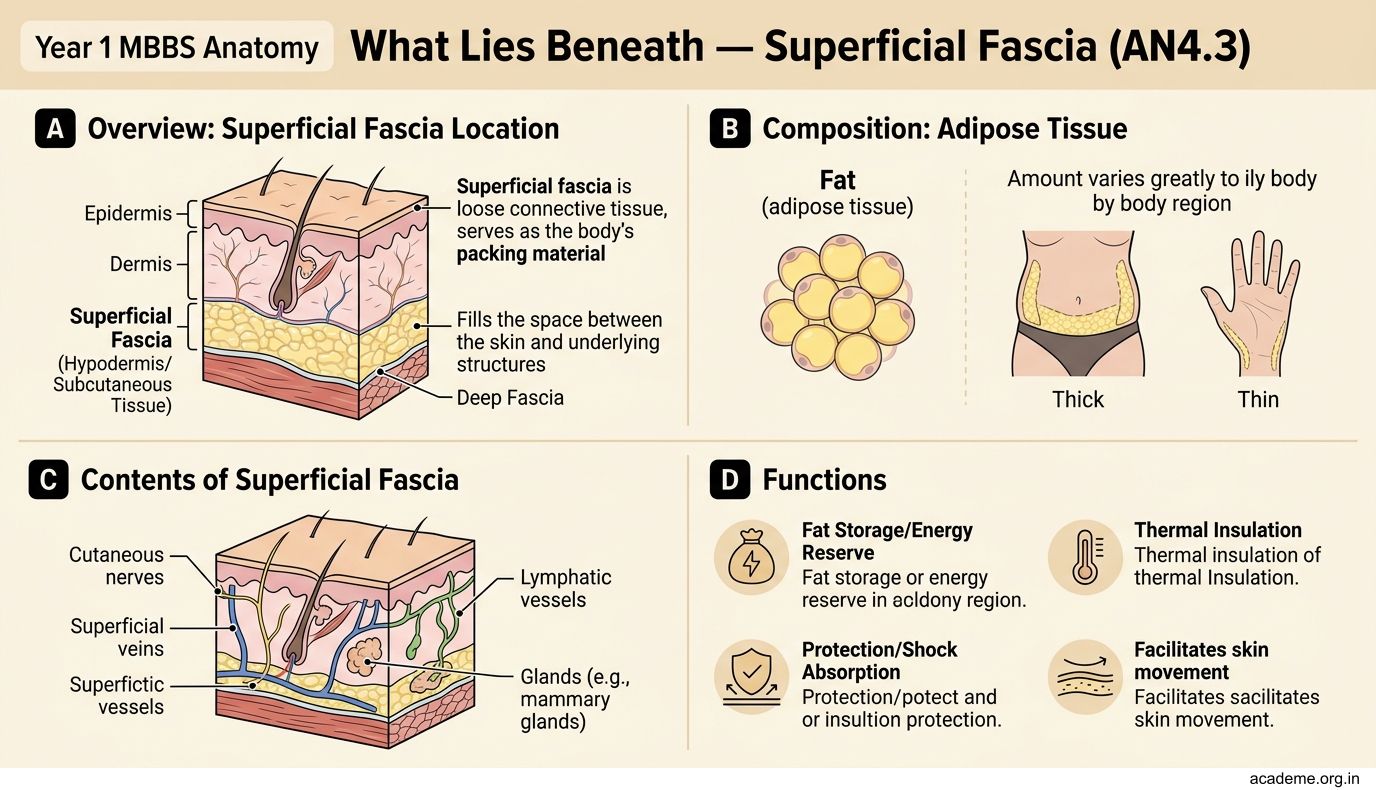

Figure: What Lies Beneath — Superficial Fascia (AN4.3)
SELF-CHECK
A nurse needs to give a subcutaneous insulin injection. She chooses a site on the abdomen rather than the back of the hand. Why is the abdomen a better site?
A. The abdomen has thicker epidermis for needle protection
B. The abdomen has more superficial fascia (subcutaneous fat) for drug absorption
C. The abdomen has fewer blood vessels, reducing bleeding risk
D. The abdomen has no dermatomes, so injections are painless
Reveal Answer
Answer: B. The abdomen has more superficial fascia (subcutaneous fat) for drug absorption
The abdomen has a thick layer of superficial fascia (subcutaneous fat), which provides a good depot for slow drug absorption. The back of the hand has almost no subcutaneous fat — an injection there would be painful and absorb too quickly. Subcutaneous injection sites are chosen based on fat thickness in the superficial fascia.
Deep Fascia — The Body's Internal Wrapping (AN4.4)
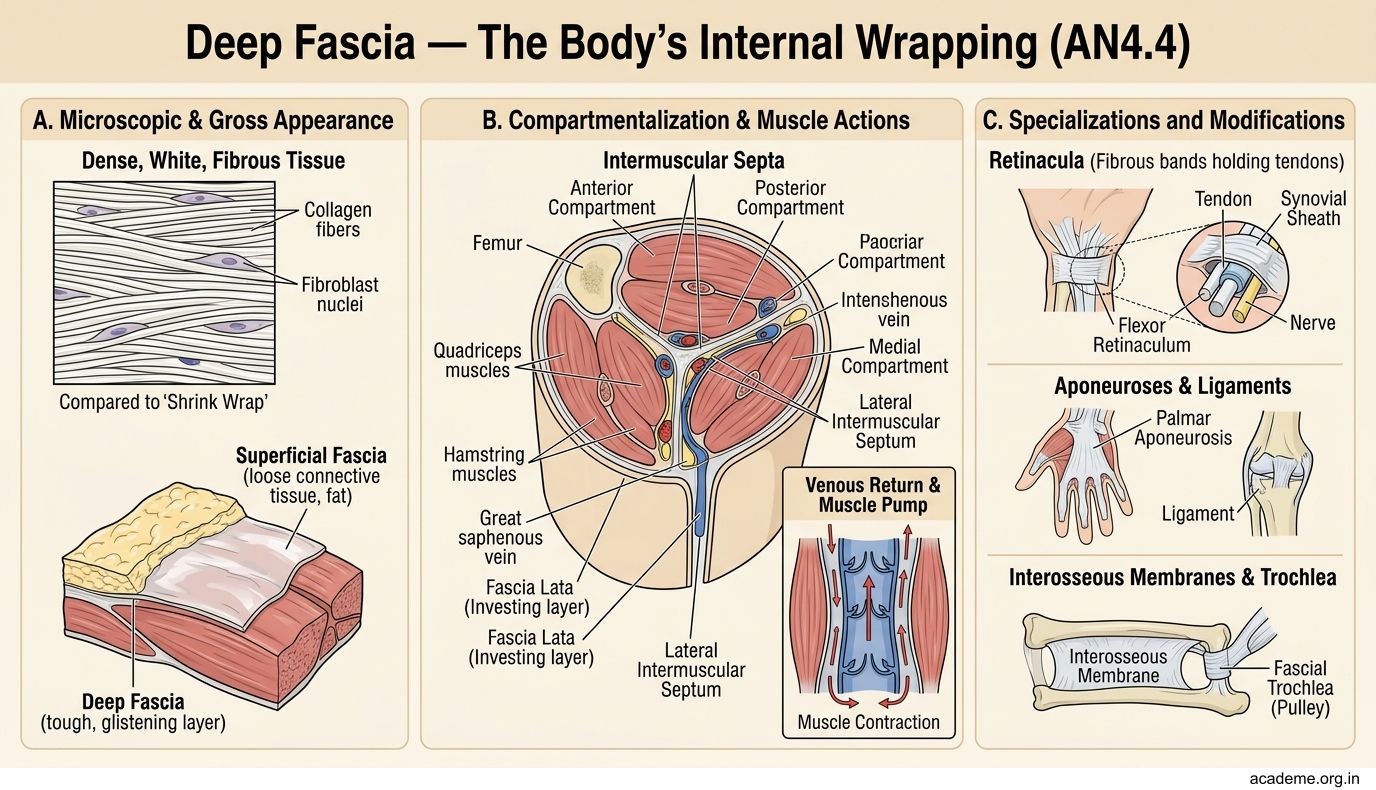
Beneath the superficial fascia lies a tougher, denser layer called deep fascia. If superficial fascia is packing material, deep fascia is like shrink wrap — it tightly envelops muscles, blood vessels, and nerves, holding them in place and separating them into compartments.
Deep fascia has no fat — it's dense, white, fibrous tissue made mainly of collagen.
Modifications of deep fascia — in certain locations, deep fascia becomes specialised:
- Retinacula (singular: retinaculum) — thickened bands of deep fascia that hold tendons in place at joints. You have retinacula at your wrist (preventing your flexor tendons from bowstringing when you flex your hand) and ankle.
- Intermuscular septa — sheets of deep fascia that divide the limb into compartments. Each compartment contains a group of muscles with their nerve and blood supply. This is clinically crucial — in compartment syndrome (after a fracture or crush injury), swelling inside a compartment can compress the blood vessels and nerves, killing the muscle if not treated urgently.
- Fascial sheaths — tubes of deep fascia that wrap around individual blood vessels and nerves (like the carotid sheath in the neck).
- Aponeuroses — flat, sheet-like tendons made of deep fascia (like the palmar aponeurosis in the hand or the plantar aponeurosis in the sole of the foot).
Why Surgeons Cut in a Particular Direction — Langer's Lines (AN4.5)
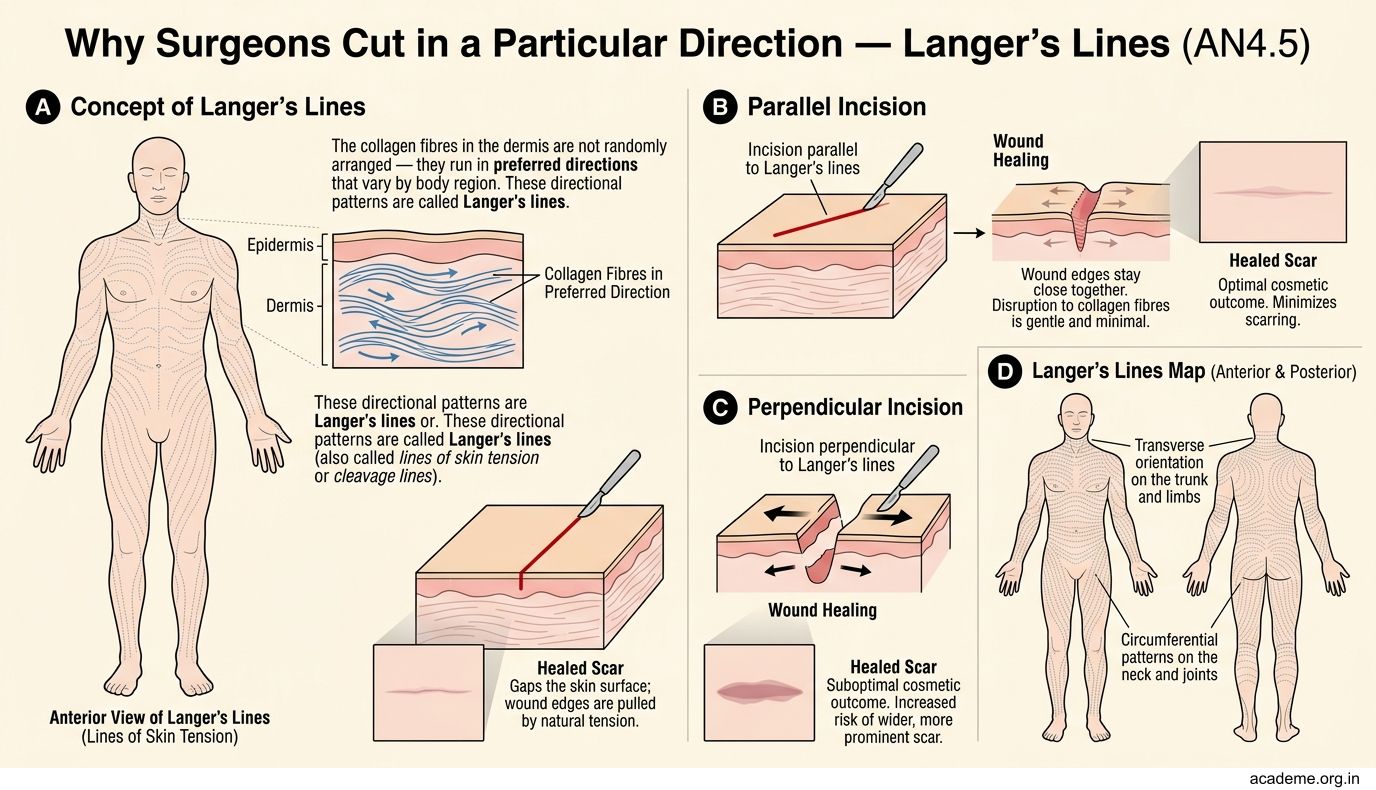
The collagen fibres in the dermis are not randomly arranged — they run in preferred directions that vary by body region. These directional patterns are called Langer's lines (also called lines of skin tension or cleavage lines).
Why do Langer's lines matter?
- An incision made parallel to Langer's lines separates collagen fibres gently — the wound edges stay close together and heal with a thin, neat scar
- An incision made across Langer's lines cuts through collagen bundles — the wound gapes open and heals with a wide, thick scar
This is why surgeons plan their incisions carefully. On the face (where cosmetic outcome matters most), incisions always follow Langer's lines. On the abdomen, the direction depends on which organs need to be accessed.
Try this: Gently pinch the skin on the back of your forearm in different directions. You'll notice it stretches more easily in one direction than another — the direction of easier stretch is perpendicular to Langer's lines (and the direction of less stretch is along them).
SELF-CHECK
A surgeon is planning an incision on the face for a cosmetic procedure. To minimise scarring, the incision should be made:
A. Perpendicular to Langer's lines, to allow maximum wound gaping for drainage
B. Parallel to Langer's lines, so collagen fibres are separated gently and the scar is thin
C. In any direction, because facial skin heals well regardless of incision orientation
D. Diagonally to Langer's lines, as a compromise between access and cosmesis
Reveal Answer
Answer: B. Parallel to Langer's lines, so collagen fibres are separated gently and the scar is thin
Incisions made parallel to Langer's lines cut between collagen bundles rather than across them. The wound edges stay close together, and the resulting scar is thin and neat. On the face, where cosmetic outcome is critical, this is essential. An incision across Langer's lines produces a wide, unsightly scar because the collagen bundles pull the wound edges apart.
CLINICAL PEARL
Compartment syndrome is a surgical emergency. After a fracture (especially of the forearm or leg), swelling inside a tight fascial compartment can compress the arteries and nerves within it. The classic signs are the 5 P's: Pain (out of proportion, especially on passive stretching), Pallor, Pulselessness, Paraesthesia (tingling), and Paralysis. The treatment is an emergency fasciotomy — cutting open the deep fascia to release the pressure. Knowing that deep fascia forms rigid compartments explains why this happens and why it's so urgent.