Page 2 of 6
AN44.1-7 | Anterior abdominal wall — SDL Guide (Part 2)
Part 4: The Inguinal Canal and Hernia (AN44.4, AN44.5)
The inguinal canal is an oblique passage (~4 cm long) through the lower anterior abdominal wall, running from the deep (internal) inguinal ring to the superficial (external) inguinal ring. It runs parallel to and just above the inguinal ligament.
The inguinal canal has four walls, a roof, and a floor:
| Component | Structure |
|---|---|
| Anterior wall | External oblique aponeurosis (whole length); internal oblique muscle (lateral third) |
| Posterior wall | Transversalis fascia (whole length); conjoint tendon (medial third) |
| Roof | Arching fibres of internal oblique + transversus abdominis |
| Floor | Upper surface of inguinal ligament; lacunar ligament (medially) |
Rings:
- Deep (internal) inguinal ring: An oval defect in the transversalis fascia. Location: 1.25 cm above the midpoint of the inguinal ligament (midinguinal point). The inferior epigastric vessels lie medial to this ring — this is the key landmark distinguishing direct from indirect hernia.
- Superficial (external) inguinal ring: A triangular gap in the external oblique aponeurosis, just above and medial to the pubic tubercle.
Contents in the male:
1. Spermatic cord (vas deferens + testicular artery + pampiniform plexus + genital branch of genitofemoral nerve + ilioinguinal nerve + lymphatics)
2. Ilioinguinal nerve (L1) — lies outside the spermatic cord proper but passes through the canal
Contents in the female: Round ligament of the uterus (homologue of the gubernaculum)
Hesselbach's triangle (inguinal triangle):
Boundaries: Medially — lateral border of rectus abdominis; Laterally — inferior epigastric vessels; Inferiorly — medial half of inguinal ligament.
Direct hernias emerge within this triangle.
Inguinal hernias — Direct vs Indirect:
| Feature | Indirect inguinal hernia | Direct inguinal hernia |
|---|---|---|
| Mechanism | Passes through the deep inguinal ring, through the full length of the canal, and out through the superficial ring | Pushes directly through Hesselbach's triangle (no canal traversal) |
| Relation to inferior epigastric vessels | Lateral (outside Hesselbach's triangle) | Medial (inside Hesselbach's triangle) |
| Covering | Has all three layers of spermatic cord covering (derived from transversalis fascia, internal oblique, external oblique) | Covered only by transversalis fascia and skin |
| Age/risk | Young men, persistent processus vaginalis, high intra-abdominal pressure | Older men, weakness of transversalis fascia/conjoint tendon |
| Risk of strangulation | Higher (tight ring can compress contents) | Lower (broad-based defect) |
| Reduction with digital pressure | Deep inguinal ring compression stops hernia reappearing | Does NOT stop it reappearing |
Mnemonic: MALL — Medial = direct, Lateral = indirect (relative to inferior epigastric vessels)

Figure: Part 4: The Inguinal Canal and Hernia (AN44.4, AN44.5)

Figure: The inguinal canal has four walls, a roof, and a floor:

Figure: Inguinal hernias — Direct vs Indirect:
SELF-CHECK
A hernia sac exits medial to the inferior epigastric vessels. Which type of inguinal hernia does this represent?
A. Indirect inguinal hernia
B. Direct inguinal hernia
C. Femoral hernia
D. Umbilical hernia
Reveal Answer
Answer: B. Direct inguinal hernia
What forms the posterior wall of the inguinal canal in its medial third?
A. Transversalis fascia only
B. Conjoint tendon (combined EO + IO aponeurosis)
C. Posterior lamella of internal oblique aponeurosis
D. Peritoneum
Reveal Answer
Answer: B. Conjoint tendon (combined EO + IO aponeurosis)
Part 5: Common Abdominal Incisions (AN44.7)
Surgical incisions are designed around the muscular anatomy of the abdominal wall — their choice balances access, wound strength, nerve preservation, and healing.

Figure: Part 5: Common Abdominal Incisions (AN44.7)
1. Midline incision (laparotomy)
- Through the linea alba, from xiphisternum to pubic symphysis (or any portion)
- Advantages: avascular (linea alba), extensible, rapid, no major nerve damage
- Disadvantage: weaker wound → higher incisional hernia rate
- Uses: emergency laparotomy, exploratory surgery
2. Paramedian incision
- Vertical, 2–3 cm lateral to midline, opening the anterior rectus sheath, displacing rectus laterally, and opening the posterior sheath
- Better wound strength than midline (intact sheath reapposed over the muscle)
- Less common now (replaced by midline + adequate closure)
3. Kocher's (right subcostal) incision
- Oblique, parallel to right costal margin (~2.5 cm below it)
- Divides external oblique, internal oblique, transversus abdominis; preserves nerve supply (nerves enter from below)
- Uses: cholecystectomy (right), splenectomy (left), bilateral subcostal = "rooftop" for liver transplantation
- Note: cuts across dermatomes T7–T9 (no paralysis; dermatomal overlap preserves sensation)
4. Gridiron (McBurney's) incision
- 2.5 cm perpendicular to the line from ASIS to umbilicus at McBurney's point (1/3 of the way from ASIS)
- Split (not cut) muscles — external oblique split in line of fibres; internal oblique and transversus split perpendicular to each → no muscle is actually cut
- Uses: appendicectomy
- Self-sealing wound (muscle layers close as wall tension is restored)
5. Lanz incision
- Transverse version of the gridiron at the same point; cosmetically superior
- Uses: appendicectomy, better cosmesis (Langer's lines)
6. Pfannenstiel incision
- Low transverse, ~3 cm above pubic symphysis, within the pubic hair line
- Transverse skin + anterior rectus sheath; rectus muscles are split vertically and retracted laterally
- Virtually cosmetically invisible → standard for caesarean section, hysterectomy, bladder surgery
- Disadvantage: limited access superiorly
7. Rutherford Morison (oblique right iliac fossa) incision
- Extends from near the ASIS laterally and curves medially and downward
- Uses: renal transplant surgery
Laparoscopic port placement anatomy:
- 10 mm umbilical port: through the umbilicus (avascular, thin)
- Working ports at 5 mm: lateral to the inferior epigastric vessels (marked by transillumination or Doppler)
- Injury to the inferior epigastric artery during port insertion → port-site haematoma or catastrophic haemorrhage
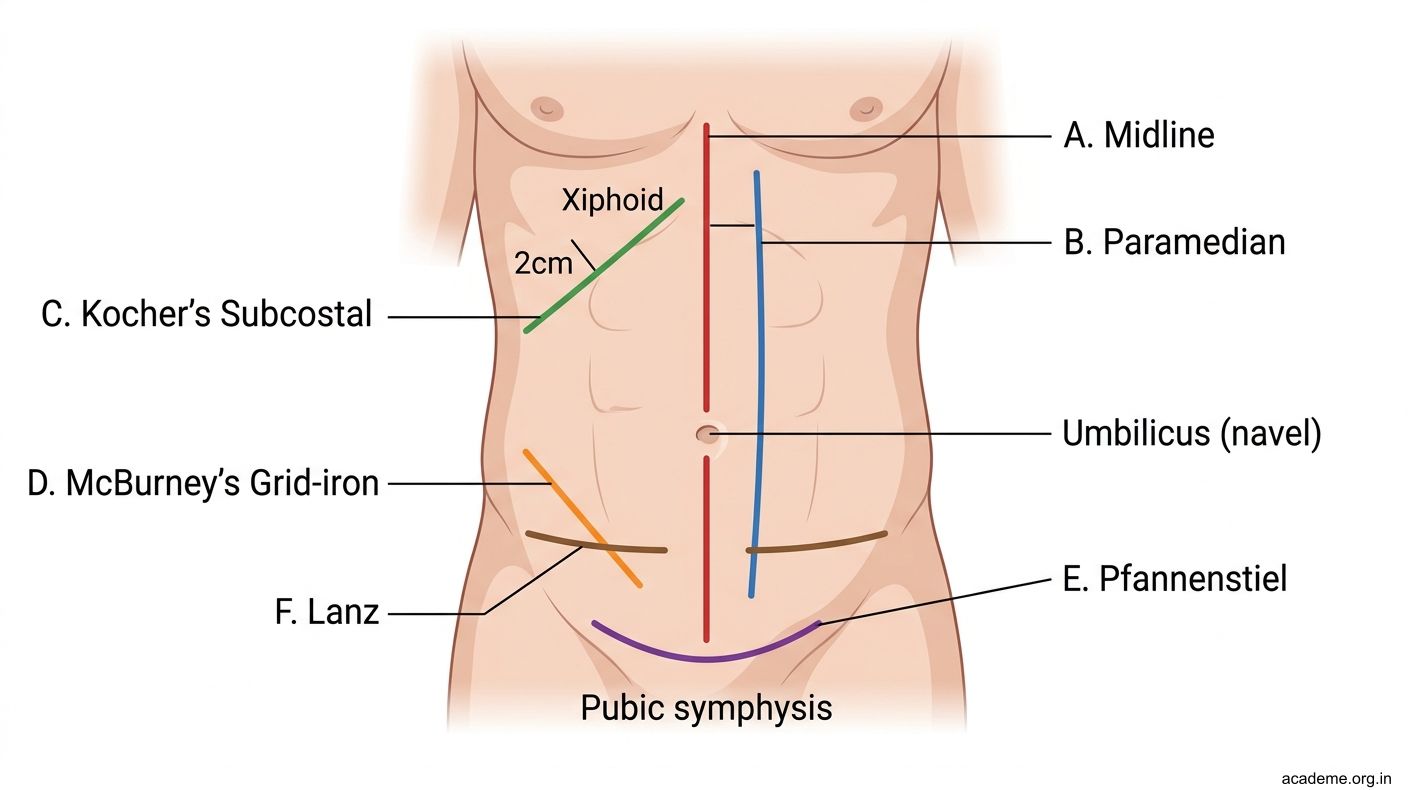
Figure: Part 5: Common Abdominal Incisions (AN44.7)
CLINICAL PEARL
The gridiron (McBurney's) incision for appendicectomy is an anatomical masterpiece. Rather than cutting through the muscles, the surgeon uses a pair of artery forceps (or a finger) to split each muscle in the direction of its own fibres:
- External oblique: split along its fibres (downward and medially)
- Internal oblique + transversus: split perpendicular to their fibres (upward and laterally)
When the retractors are removed and the patient coughs or strains, the opposing muscle contraction tends to close the split rather than open it — the wound is self-sealing.
This explains why post-appendicectomy incisional hernia is rare through a gridiron incision, whereas midline laparotomy wounds have a 10–15% incisional hernia rate. Understanding the anatomy lets you predict and prevent complications.