Page 2 of 6
AN52.1-8 | Histology & Embryology (Abdomen & Pelvis) — SDL Guide (Part 2)
Gut Development — Foregut, Midgut, Hindgut (AN52.6)
Divisions by blood supply:
| Division | Extent | Blood supply | Derivatives |
|---|---|---|---|
| Foregut | Pharynx → mid-duodenum (at ampulla of Vater) | Coeliac trunk | Oesophagus, stomach, liver, gallbladder, pancreas, upper duodenum |
| Midgut | Mid-duodenum → 2/3 of transverse colon | Superior mesenteric artery | Lower duodenum, jejunum, ileum, appendix, ascending colon, proximal 2/3 transverse colon |
| Hindgut | Distal 1/3 transverse colon → upper anal canal | Inferior mesenteric artery | Distal transverse colon, descending, sigmoid, rectum, upper anal canal |
Key developmental events:
Duodenal atresia/stenosis: During 5th–6th weeks, the duodenum becomes a solid cord of proliferating endoderm, then recanalises. Failure = duodenal atresia → "double-bubble" on X-ray (gas in stomach + proximal duodenum). Associated with Down syndrome (trisomy 21) in 30%.
Midgut rotation and fixation:
- 6th week: midgut herniates into umbilical cord (physiological umbilical hernia)
- Returns at 10–12 weeks: rotates 270° counterclockwise around the axis of the superior mesenteric artery
- Malrotation: incomplete rotation → caecum high in the abdomen + abnormal peritoneal bands (Ladd's bands) across duodenum → duodenal obstruction; risk of volvulus around SMA pedicle → catastrophic ischaemia
Hirschsprung's disease (congenital aganglionosis):
- Failure of neural crest cells to migrate to the distal colon → absence of Auerbach's and Meissner's plexuses
- Aganglionic segment fails to relax → functional obstruction; normal (ganglionic) proximal bowel dilates → megacolon
- Common in Indian males; presents with delayed passage of meconium, abdominal distension
Omphalocele vs gastroschisis:
| Feature | Omphalocele | Gastroschisis |
|---|---|---|
| Defect site | Central (umbilicus) | Paraumbilical (right side) |
| Sac | Present (peritoneum + amnion) | Absent (bowel free) |
| Associated anomalies | Common (cardiac, chromosomal) | Rare |
| Aetiology | Failure of physiological hernia to reduce | Avascular necrosis of umbilical vein/right omphalomesenteric artery |
Meckel's diverticulum ("rule of 2s"): 2% population, 2 feet (60 cm) from the ileocaecal valve, 2 inches long, 2 types of ectopic tissue (gastric mucosa → peptic ulceration, pancreatic tissue), presents in 2% of those who have it, commonest complication in first 2 years of life. Remnant of vitellointestinal (omphalomesenteric) duct.

Figure: Gut Development — Foregut, Midgut, Hindgut (AN52.6)

Figure: Key developmental events:

Figure: Omphalocele vs gastroschisis:
Development of the Urinary System (AN52.7)
Three successive kidney generations from intermediate mesoderm:
1. Pronephros (week 4): non-functional; cervical region; disappears completely
2. Mesonephros (weeks 4–8): functional; mesonephric (Wolffian) duct drains to cloaca; contributes to the male reproductive system
3. Metanephros (week 5 onward): permanent kidney; develops from ureteric bud (outgrowth of mesonephric duct) + metanephric mesenchyme
Ureteric bud induces metanephric mesenchyme → nephron formation (collecting system).
Ascent of kidney: Kidneys ascend from the pelvis to L1–L2 as the embryo grows; they rotate 90° medially.
Congenital anomalies:
- Horseshoe kidney: inferior poles of both kidneys fuse across the midline (before ascent) → ascent blocked by inferior mesenteric artery at L3; usually asymptomatic; increased risk of pelviureteric junction obstruction, stone formation, and Wilms' tumour
- Renal agenesis (unilateral): failure of ureteric bud to develop; contralateral kidney undergoes compensatory hypertrophy
- Polycystic kidney disease (PKD): Autosomal dominant (ADPKD) — failure of collecting tubule and secretory tubule to fuse → cysts; presents in adults. Autosomal recessive (ARPKD) — defect in tubular differentiation; presents at birth (bilateral flank masses, oligohydramnios, Potter sequence)
- Duplex collecting system: bifid renal pelvis or double ureter from bifurcation of ureteric bud; the upper moiety ureter opens more medially and inferiorly than normal (Weigert-Meyer rule) → prone to obstruction and ectopic ureter
Bladder development: The cloaca divides by the urorectal septum at week 7 → urogenital sinus (anterior) + anorectal canal (posterior). The upper part of the urogenital sinus → urinary bladder; the lower part → urethra.

Figure: Development of the Urinary System (AN52.7)
Development of the Reproductive System (AN52.8)
Indifferent stage (weeks 1–7): Both male and female embryos have gonadal ridges + Wolffian (mesonephric) ducts + Müllerian (paramesonephric) ducts.

Figure: Development of the Reproductive System (AN52.8)
Sex determination:
- SRY gene (on Y chromosome) → testes differentiate
- In the absence of SRY → ovaries differentiate
Male differentiation:
- Sertoli cells → Anti-Müllerian Hormone (AMH) → Müllerian ducts regress
- Leydig cells → testosterone → Wolffian duct persists → epididymis, vas deferens, seminal vesicle
- DHT (from testosterone by 5α-reductase) → external genitalia masculinisation (penis, scrotum)
Female differentiation:
- No AMH → Müllerian ducts persist → uterine tubes, uterus, upper vagina
- No testosterone → Wolffian ducts regress
- Labia majora, labia minora, clitoris develop from indifferent external genitalia
Testicular descent:
- Testes descend from the posterior abdominal wall (retroperitoneal) through the inguinal canal into the scrotum (7th–8th month)
- Guided by gubernaculum testis
- Peritoneal processus vaginalis accompanies the testis → normally obliterates → if patent = congenital inguinal hernia or hydrocele
Congenital anomalies:
- Undescended testis (cryptorchidism): testis arrested anywhere along its path; increased risk of infertility and testicular cancer; treated with orchidopexy before 2 years of age
- Hypospadias: failure of urethral folds to fuse over the urogenital sinus → urethral opening on the ventral surface of the penis (commonest urological malformation in boys; 1 in 250 births in India)
- Epispadias: rare; urethral opening on the dorsal surface; associated with bladder exstrophy
- Double uterus/bicornuate uterus: incomplete fusion of Müllerian ducts → various uterine anomalies (arcuate, subseptate, bicornuate, didelphys)
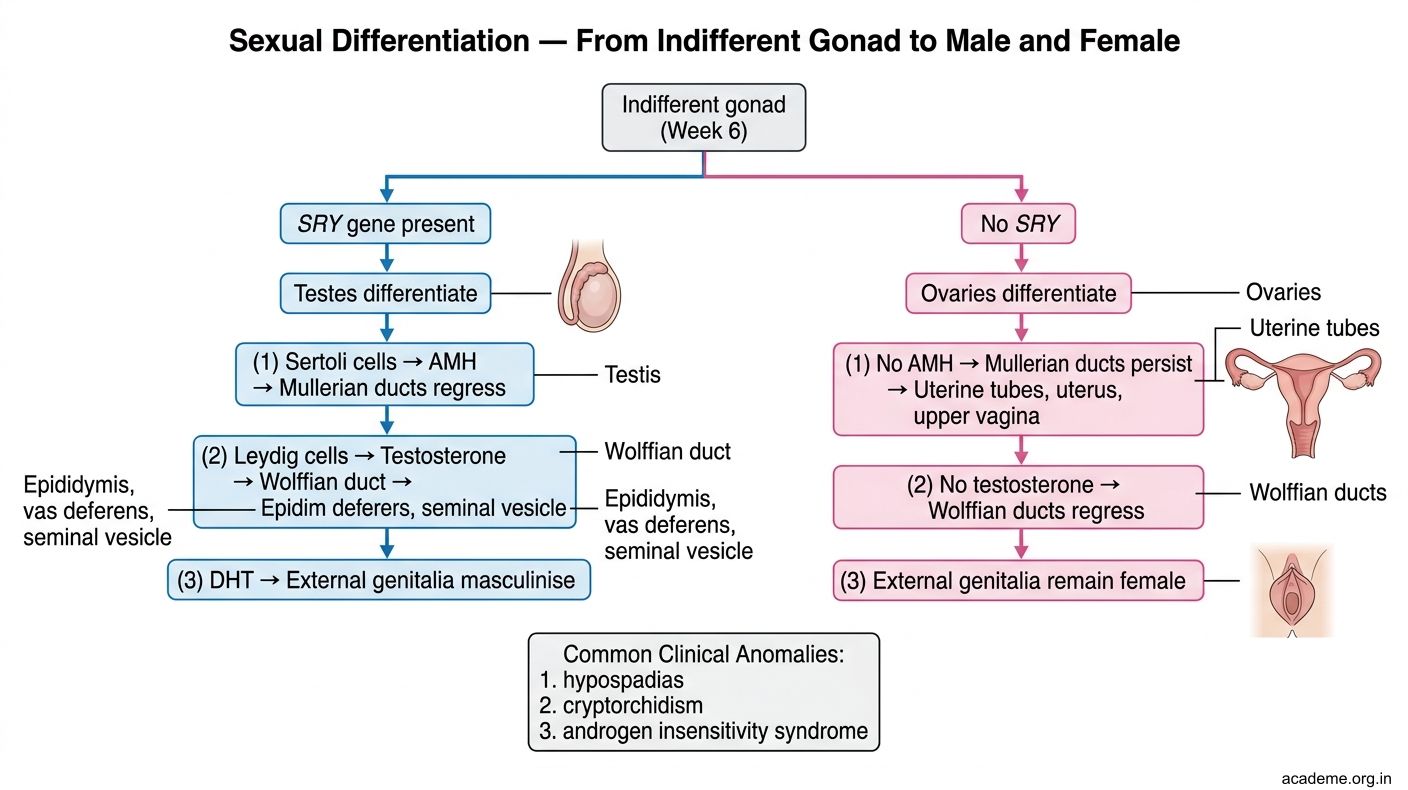
Figure: Development of the Reproductive System (AN52.8)
SELF-CHECK
A. Pyloric stenosis — hypertrophy of pyloric smooth muscle due to neonatal inflammation
B. Duodenal atresia — failure of recanalisation of the solid cord phase of duodenal development; associated with Down syndrome in 30%
C. Malrotation — incomplete counterclockwise rotation of the midgut loop leading to Ladd's bands
D. Meckel's diverticulum — persistent vitellointestinal duct causing luminal obstruction
Reveal Answer
Answer: see explanation below
The 'double-bubble' sign (gas in stomach + proximal duodenum with no distal gas) is pathognomonic of duodenal atresia (or severe duodenal stenosis). Embryological basis: during weeks 5–6, the duodenum becomes a solid cord of proliferating endoderm, then recanalises. Failure = complete obstruction. Check for Down syndrome (trisomy 21) in 30% of cases. Bilious vomiting confirms the obstruction is below the ampulla of Vater (bile duct opens here). Management: duodenoduodenostomy.
SELF-CHECK
A. Autosomal dominant polycystic kidney disease (ADPKD) — accumulation of cysts in adults from defective cystogenesis
B. Horseshoe kidney — fusion of inferior poles preventing ascent
C. Autosomal recessive polycystic kidney disease (ARPKD) — defect in tubular differentiation; presents in infancy/childhood
D. Wilms' tumour (nephroblastoma) — malignant kidney tumour of childhood
Reveal Answer
Answer: see explanation below
ARPKD (autosomal recessive PKD) presents in the neonatal period or early childhood — bilateral flank masses, oligohydramnios (Potter sequence if severe), hypertension, renal failure. Consanguinity increases the risk. The defect is in PKHD1 (fibrocystin) → abnormal tubular differentiation with diffuse microcrysts in collecting ducts. ADPKD presents in adults (3rd–5th decade) with fewer, larger cysts.
CLINICAL PEARL
Hirschsprung's disease — remembering the embryological basis: Neural crest cells migrate craniocaudally along the bowel wall from weeks 5–12. The LAST segment to be colonised is the distal rectum/sigmoid. In Hirschsprung's, migration stops prematurely → the distal segment (beyond the migration arrest) is aganglionic. The aganglionic bowel remains tonically contracted (no Auerbach's/Meissner's plexus → no peristaltic relaxation) → functional obstruction. The dilated proximal bowel (which IS ganglionic and functions normally but cannot empty) is what the surgeon sees — not the aganglionic segment — hence the pull-through operation (resect the aganglionic segment, anastomose ganglionic bowel to the anus). Rectal suction biopsy confirms aganglionosis.