Page 1 of 6
AN54.1-4 | Radiodiagnosis — SDL Guide
Learning Objectives
- Describe the principles of plain radiography, CT, MRI, PET scan, and DSA (AN54.1)
- Identify and describe features visible on a plain X-ray of the abdomen (AN54.2)
- Describe and identify barium swallow, barium meal, barium enema, cholecystography, IVP, and hysterosalpingography (AN54.3)
- Describe the role of ERCP, CT abdomen, MRI, and arteriography in abdominal radiodiagnosis (AN54.4)
INSTRUCTIONS
Read each section in order. Bold terms (like this) are key vocabulary. Attempt the self-check questions before revealing answers. Focus on linking anatomy to imaging appearances.
References
- Gray's Anatomy for Students — Imaging chapters (Textbook)
- BD Chaurasia's Human Anatomy — Radiodiagnosis sections (Textbook)
- NMC UG CBUC 2024, Competencies AN54.1–AN54.4 (Curriculum)
Version 1.0 | Academe Content Engine v2
CLINICAL SCENARIO
It is 11 PM in the casualty ward at a government hospital in Chennai. A 52-year-old man collapses with sudden severe abdominal pain. The duty surgeon requests an "X-ray abdomen erect." Within minutes, the image shows a crescent of air under the right hemidiaphragm.
What does that air mean? Where did it come from? And why could a simple X-ray tell you this?
This module explains how the anatomy you have learned becomes visible on imaging — and how recognising those images can change the course of a patient's life.
WHY THIS MATTERS
Radiodiagnosis is applied anatomy. Every image you interpret is anatomy made visible by physics:
• Plain X-ray — bones and gas stand out because they absorb radiation differently from soft tissue
• Barium studies — coat the gut lumen to reveal mucosal folds and narrowings you cannot see otherwise
• CT and MRI — slice the body in cross-section at the planes you studied in sectional anatomy
• IVP and ERCP — visualise the urinary and biliary systems by contrast that is excreted physiologically
The NMC requires you to describe and identify these investigations (AN54.1–AN54.4) because you will order or interpret them as an intern and junior doctor — every day.
RECALL
From your earlier study, you already know:
• The abdominal cavity contains the stomach, small intestine, large intestine, liver, spleen, kidneys, and pancreas
• Bones appear white (radiopaque) on X-ray; air appears black (radiolucent); soft tissue is grey
• The peritoneum forms the lining of the abdominal cavity and visceral organs
• The transpyloric plane (L1) passes through the pylorus, kidney hila, and SMA origin
In this module we apply this knowledge to real imaging.
Principles of Plain Radiography — The Physics in 3 Minutes
Plain radiography (X-ray) passes a beam of X-radiation through the body. Different tissues absorb the beam to different degrees — this differential absorption creates the image.
Five radiographic densities (from most to least opaque, i.e., whitest to blackest):
1. Metal/bone — most opaque (white) — calcium absorbs strongly
2. Soft tissue/fluid — intermediate grey — organs, blood, fluid
3. Fat — slightly darker grey — visceral fat planes
4. Air/gas — black (radiolucent) — bowel lumen, lungs, free air
5. Foreign body (depends on material)
Key principle: Two adjacent structures of the same density cannot be distinguished ("silhouette sign" — loss of normal border means disease in adjacent tissue).
Clinical application in abdomen:
• Gas under diaphragm (erect film) = free perforation (perforated peptic ulcer, perforated viscus) — this is a surgical emergency
• Bowel gas pattern — normal vs obstructed (dilated loops, air-fluid levels on erect film)
• Soft tissue masses — indistinct outlines suggest fluid or tumour
• Calcification — renal stones, gallstones (10% radio-opaque), pancreatic calcification, aortic wall calcification

Figure: Principles of Plain Radiography — The Physics in 3 Minutes
Contrast Radiography — CT — MRI — PET
Contrast radiography adds a radiopaque contrast agent to visualise hollow organs:
• Barium sulfate — insoluble, safe unless perforation suspected; coats GI mucosa
• Iodine-based contrast — soluble, used when perforation is possible (water-soluble), or injected IV for CT/angiography/IVP
Computed Tomography (CT):
X-rays from multiple angles are processed by computer to generate cross-sectional images. Hounsfield units (HU) quantify density: bone +400 to +1000 HU, soft tissue 20–80 HU, water 0 HU, fat −100 HU, air −1000 HU.
• CT abdomen — gold standard for acute abdomen, trauma, tumour staging, abdominal aortic aneurysm
• IV contrast enhances vascular structures and organs
Magnetic Resonance Imaging (MRI):
Uses magnetic field + radiofrequency pulses — no ionising radiation. Excellent soft-tissue contrast.
• T1-weighted — fat bright, water dark — good for anatomy, post-contrast enhancement
• T2-weighted — water bright — good for fluid, oedema, biliary/pancreatic ducts (MRCP)
• Best for: liver lesions, biliary system (MRCP), pelvic organs, rectal cancer staging
Positron Emission Tomography (PET scan):
Detects metabolic activity using 18F-FDG (fluorodeoxyglucose) — a radioactive glucose analogue. Cancer cells have high glucose uptake → hot spots. Usually combined with CT (PET-CT) for anatomical localisation. Used in: cancer staging, detecting recurrence, treatment response.
Digital Subtraction Angiography (DSA):
Intra-arterial contrast injection; pre-contrast image digitally subtracted to isolate vessels. Gold standard for vascular anatomy. Used for: renal artery stenosis, mesenteric ischaemia, portal hypertension, pre-operative vascular mapping.

Figure: Contrast Radiography — CT — MRI — PET
SELF-CHECK
On an erect plain X-ray abdomen, you see a crescent of air under the right hemidiaphragm. This most likely indicates:
A. Normal bowel gas
B. Free intraperitoneal air from a perforated viscus
C. A right-sided pleural effusion
D. Normal diaphragmatic anatomy
Reveal Answer
Answer: B. Free intraperitoneal air from a perforated viscus
Free air under the diaphragm on an erect X-ray is a sign of pneumoperitoneum — free intraperitoneal gas from a perforated hollow viscus (most commonly perforated peptic ulcer). It is a surgical emergency. This is one of the most important plain X-ray signs in clinical medicine.
Plain X-ray Abdomen — What to Identify Systematically
A systematic approach to reading an X-ray abdomen (AN54.2):

Figure: Plain X-ray Abdomen — What to Identify Systematically
STEP 1 — Bowel gas pattern:
• Small bowel: central, valvulae conniventes (mucosal folds cross entire width), <3 cm
• Large bowel: peripheral, haustra (partial markings), >3 cm (colon) / >5 cm (caecum)
• Dilated loops with air-fluid levels on erect film → intestinal obstruction
STEP 2 — Liver, spleen, kidney outlines:
• Liver shadow — right hypochondrium (hepatomegaly → extends across midline)
• Spleen — left hypochondrium (splenomegaly → displaces stomach gas medially)
• Kidney outlines — visible due to perirenal fat; right kidney at L1–L3, left kidney slightly higher
STEP 3 — Retroperitoneal psoas shadows:
• Psoas major forms lateral shadows from T12 to lesser trochanter
• Obliteration of psoas shadow → retroperitoneal pathology (abscess, haematoma, tumour)
STEP 4 — Calcifications:
• Renal calculi — renal angle, along ureter path, vesicoureteric junction
• Gallstones — only 10% radio-opaque (cholesterol stones invisible; pigment stones may calcify)
• Vascular calcification — aortic wall, splenic artery (worm-track calcification)
• Pancreatic calcification → chronic pancreatitis
STEP 5 — Bones:
• Lumbar vertebrae, sacroiliac joints, hip joints, ribs 10–12
• Abnormalities: fractures, metastases (lytic or sclerotic), sacroiliac joint erosion
STEP 6 — Free gas:
• Erect film: gas under diaphragm = perforation
• Supine film: Rigler's sign (both sides of bowel wall visible = gas on both sides)
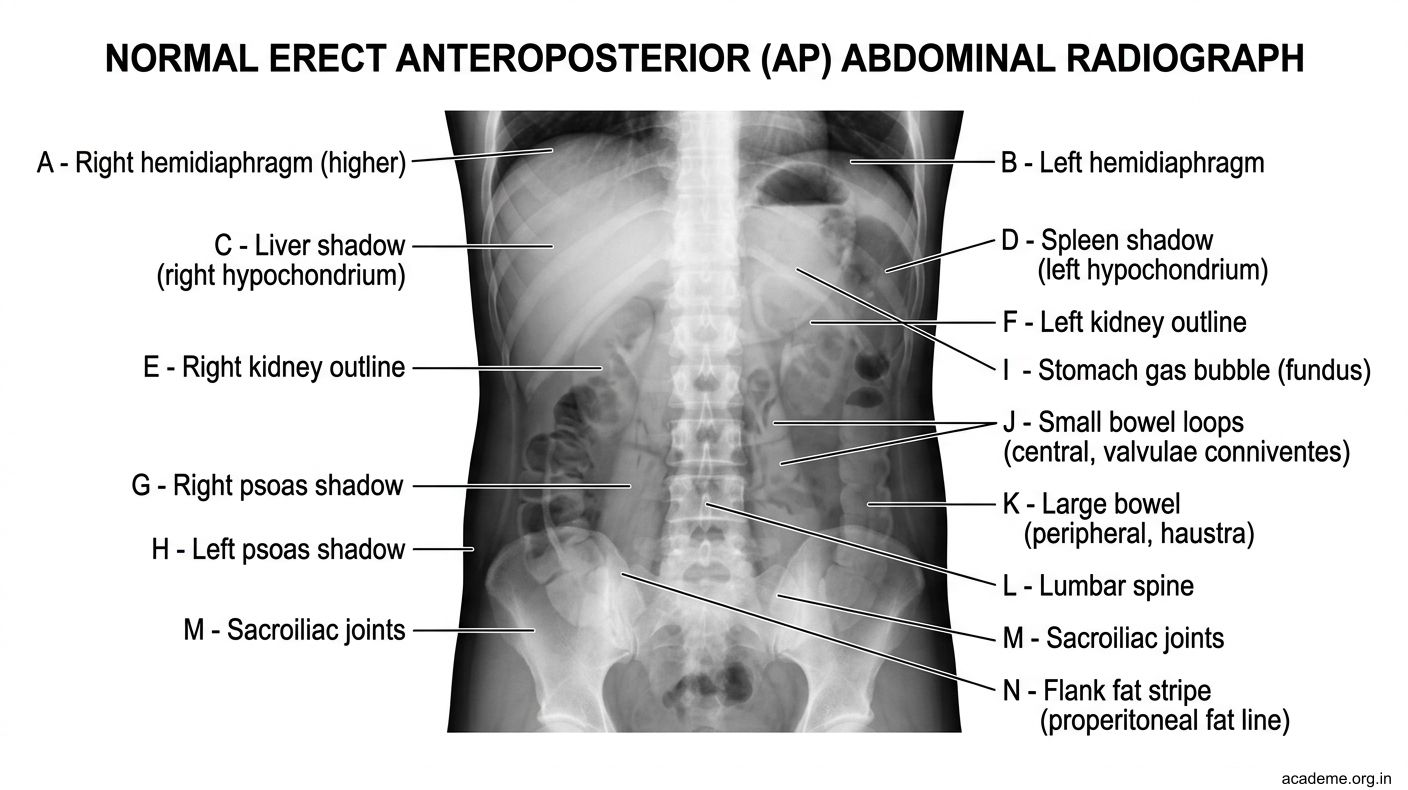
Figure: Plain X-ray Abdomen — What to Identify Systematically