Page 1 of 6
AN69.1-3 | Blood Vessels — SDL Guide
This Self-Directed Learning guide covers the histology and ultrastructure of blood vessels — arteries, veins, and capillaries — and how their microscopic structure underpins their physiological function.
Learning Objectives
- Identify elastic and muscular arteries, veins, and capillaries under the microscope (AN69.1)
- Describe the three-layered wall structure of blood vessels and structure-function correlation (AN69.2)
- Describe the ultrastructure of blood vessels including endothelial tight junctions, basement membrane, and smooth muscle (AN69.3)
INSTRUCTIONS
Work through each section in sequence. Key histological terms are bolded on first use. Attempt the self-check questions before reading the answer. The gate quiz at the end must be completed to unlock the next module.
References
- Difiore's Atlas of Histology, 12th ed. — Chapter 8: Cardiovascular System
- Ross & Pawlina, Histology: A Text and Atlas, 8th ed.
- NMC UG CBUC 2024, Competencies AN69.1–AN69.3
CLINICAL SCENARIO
A 58-year-old patient from Puducherry presents with a sudden tearing chest pain radiating to the back. CT angiography shows dissection of the thoracic aorta — blood has tracked between the layers of the vessel wall.
Why did the wall tear here? Because the tunica media of the aorta, rich in elastic fibres that normally stretch and recoil with each heartbeat, was weakened by years of hypertension. Understanding how blood vessels are built — layer by layer, fibre by fibre — is what allows you to understand why they fail.
WHY THIS MATTERS
Blood vessel histology is directly relevant to:
• Atherosclerosis — the pathology begins in the intima (tunica interna); you cannot understand plaque formation without knowing the normal intima
• Hypertension — increased workload causes hypertrophy of the tunica media of muscular arteries
• Varicose veins — failure of the thin-walled venous wall and incompetent valves
• Capillary leak syndrome — disruption of endothelial tight junctions and basement membrane integrity
• Vasculitis — inflammation of specific layers of vessel walls (e.g., giant cell arteritis targets the internal elastic lamina)
NMC requires you to identify and describe these vessels (AN69.1–AN69.3) because histopathology reports refer to vessel layers routinely.
RECALL
From your prior studies, recall:
• Blood flows through: arteries → arterioles → capillaries → venules → veins
• The heart pumps at high pressure into arteries; pressure falls progressively toward veins
• Arteries carry oxygenated blood (except pulmonary artery); veins carry deoxygenated blood (except pulmonary veins)
• You have seen basic cell biology: smooth muscle cells contract; endothelial cells line surfaces; connective tissue provides structural support
In this guide we zoom in to the microscopic architecture that makes each vessel type suited to its role in the circuit.
General Plan: The Three Tunics
Every blood vessel (except capillaries) is built on the same three-layered blueprint called tunics (from Latin tunica = coat):

Figure: General Plan: The Three Tunics
| Layer | Name | Main Components | Function |
|---|---|---|---|
| Innermost | Tunica interna (intima) | Endothelium + subendothelial connective tissue + internal elastic lamina | Non-thrombogenic lining; regulates permeability |
| Middle | Tunica media | Smooth muscle cells + elastic/collagen fibres | Vasomotion (active diameter control); structural strength |
| Outermost | Tunica externa (adventitia) | Loose collagen + fibroblasts + vasa vasorum | Anchoring; nutrition of vessel wall |
Endothelium — a single layer of flattened squamous cells lining the entire cardiovascular system (heart chambers to capillaries). It is metabolically active: it secretes NO (vasodilator), endothelin (vasoconstrictor), clotting factors, and von Willebrand factor.
Internal elastic lamina — a fenestrated (windowed) elastic sheet at the junction of intima and media. Prominent in muscular arteries; the fenestrations allow diffusion of nutrients to the media.
External elastic lamina — a less distinct elastic sheet at the junction of media and adventitia (present in muscular arteries).
Histological tip: Elastic fibres stain pink-red with H&E and brilliantly black with Verhoeff's elastic stain. The wavy appearance of elastic tissue under light microscopy is a key identification feature.
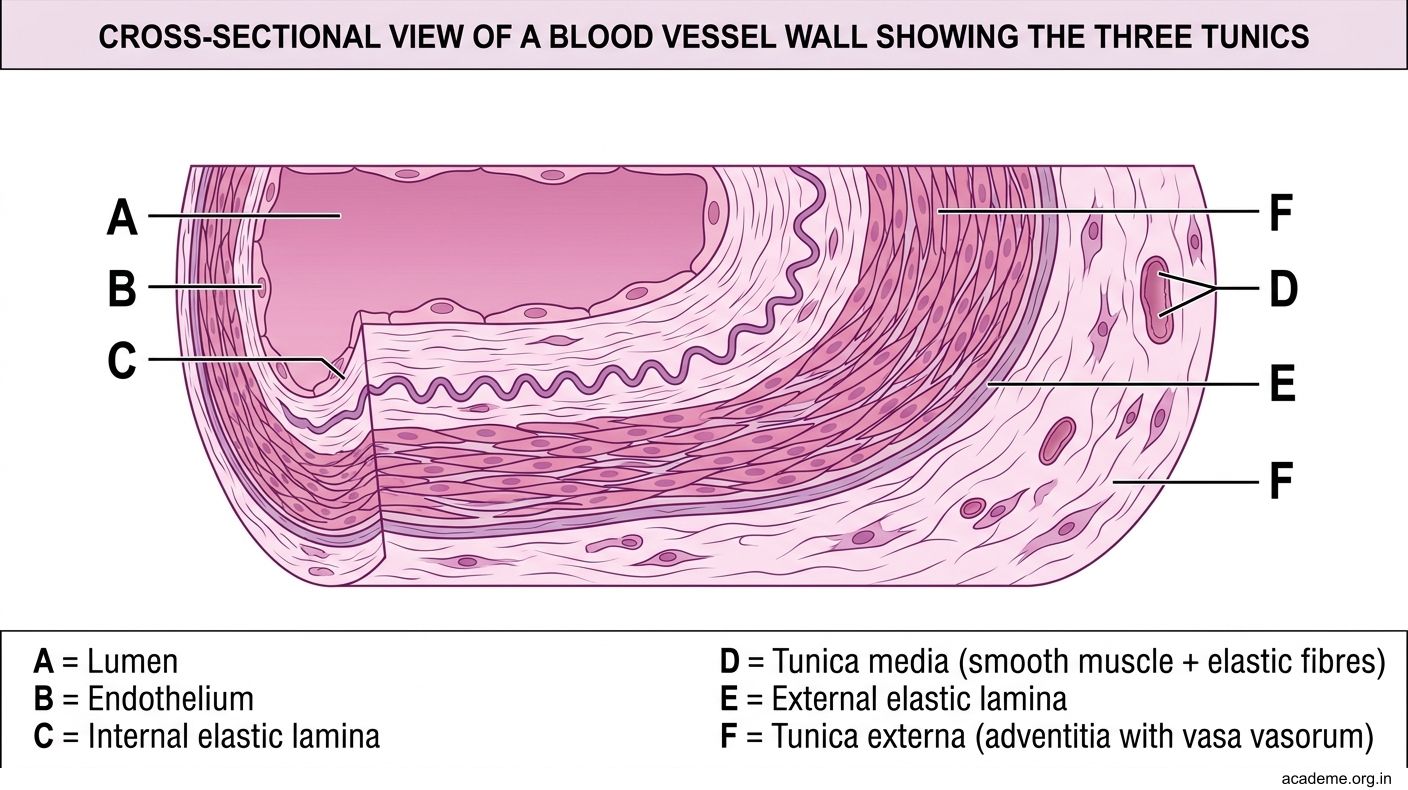
Figure: General Plan: The Three Tunics
Elastic Arteries (Conducting Arteries)
Examples: Aorta, pulmonary trunk, brachiocephalic, common carotid, subclavian arteries.
Function: Conduct blood from the heart; buffer the pressure pulse (Windkessel effect) — stretch during systole, recoil during diastole to maintain continuous flow.
Microscopic features:
- Lumen: Large; wall thickness relatively thin compared to lumen diameter
- Tunica intima: Prominent; well-developed subendothelial layer
- Tunica media: Very thick — the defining feature. Contains 40–70 concentric elastic lamellae alternating with smooth muscle cells. The numerous elastic sheets give the wall its yellow colour on gross examination and its wavy appearance on H&E staining
- Tunica adventitia: Relatively thin; contains vasa vasorum (small vessels that supply the outer media and adventitia of large vessels)
High-yield fact: Elastic arteries have many elastic lamellae in the media; muscular arteries have a prominent internal elastic lamina + external elastic lamina but far fewer medial elastic sheets.
Clinical correlation: Marfan syndrome — defective fibrillin-1 protein in elastic tissue → cystic medial necrosis → dissecting aortic aneurysm. The histology shows fragmentation of elastic lamellae and loss of smooth muscle cells in the media.

Figure: Elastic Arteries (Conducting Arteries)
Muscular Arteries (Distributing Arteries)
Examples: Femoral, radial, brachial, renal, mesenteric arteries — most named arteries in the body.

Figure: Muscular Arteries (Distributing Arteries)
Function: Distribute blood to organs; regulate regional blood flow through active vasoconstriction and vasodilation of the media.
Microscopic features:
- Tunica intima: Thin; prominent, well-defined internal elastic lamina (a crisp wavy line on H&E — the single most useful identification feature of muscular arteries)
- Tunica media: 10–40 layers of circularly arranged smooth muscle cells (the dominant cell type). Elastic fibres are sparse compared to elastic arteries
- External elastic lamina: Present (fainter than internal elastic lamina)
- Tunica adventitia: Relatively thick; well-developed collagen bundles and fibroblasts
Identification trick on histology slide: Look for TWO distinct elastic lines (internal and external elastic laminae) sandwiching a thick smooth-muscle media. The lumen wall ratio is smaller than elastic arteries (thicker wall relative to lumen).
Clinical correlation: Atherosclerosis primarily affects muscular arteries (coronary, carotid, femoral). Plaque forms in the intima, progressing through the internal elastic lamina into the media in advanced disease.

Figure: Muscular Arteries (Distributing Arteries)
SELF-CHECK — 1 : Arterial Layers
A histology slide shows a vessel with 50 concentric elastic lamellae in its wall and a relatively thin adventitia. Which vessel is most likely being examined?
A. Femoral artery
B. Thoracic aorta
C. Renal artery
D. Brachial artery
Reveal Answer
Answer: B. Thoracic aorta