Page 3 of 8
BI2.1-5 | Enzyme — SDL Guide (Part 3)
Enzyme Inhibition — How Drugs Block Enzymes (BI2.3)
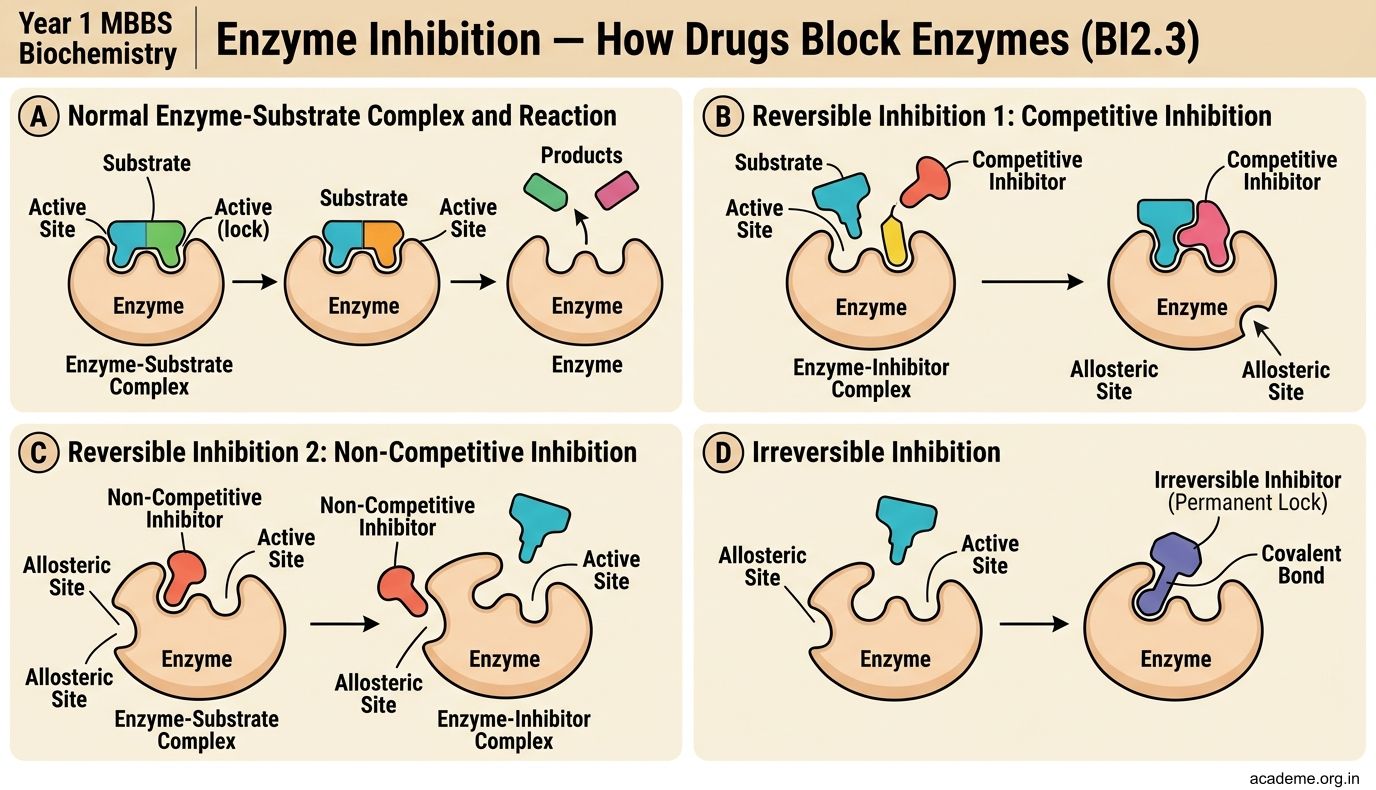
An enzyme inhibitor is a molecule that reduces enzyme activity. Inhibitors are critical in medicine because many drugs are enzyme inhibitors. There are two main categories:
Reversible Inhibition (the inhibitor binds and releases):
1. Competitive Inhibition
• The inhibitor resembles the substrate and competes for the active site
• It's like a wrong key stuck in a lock — the real key (substrate) can't get in
• Effect on kinetics: Km increases (you need more substrate to outcompete the inhibitor), but Vmax is unchanged (with enough substrate, you can overwhelm the inhibitor)
• Drug example: Methotrexate — resembles folic acid and competitively inhibits dihydrofolate reductase (used in cancer chemotherapy). Statins — competitively inhibit HMG-CoA reductase (used to lower cholesterol).
2. Non-competitive Inhibition
• The inhibitor binds to a site other than the active site (an allosteric site)
• It changes the enzyme's shape so the active site no longer works properly
• It's like someone bending your lock — even with the right key, the lock won't turn
• Effect on kinetics: Vmax decreases (some enzyme molecules are permanently disabled), but Km is unchanged (the remaining active enzyme molecules have normal substrate affinity)
• Drug example: Heavy metals (lead, mercury) — bind to sulfhydryl groups on enzymes, distorting their shape.
3. Uncompetitive Inhibition (less common)
• The inhibitor binds only to the enzyme-substrate complex (not to the free enzyme)
• Effect: Both Km and Vmax decrease
Irreversible Inhibition (the inhibitor binds permanently, destroying the enzyme):
• Drug example: Aspirin — irreversibly acetylates cyclooxygenase (COX), blocking prostaglandin synthesis. The effect lasts until new COX molecules are made.
• Organophosphates (nerve agents, some pesticides) — irreversibly inhibit acetylcholinesterase, causing a buildup of acetylcholine at nerve junctions.
Enzymes as Therapeutic Agents (BI2.3)
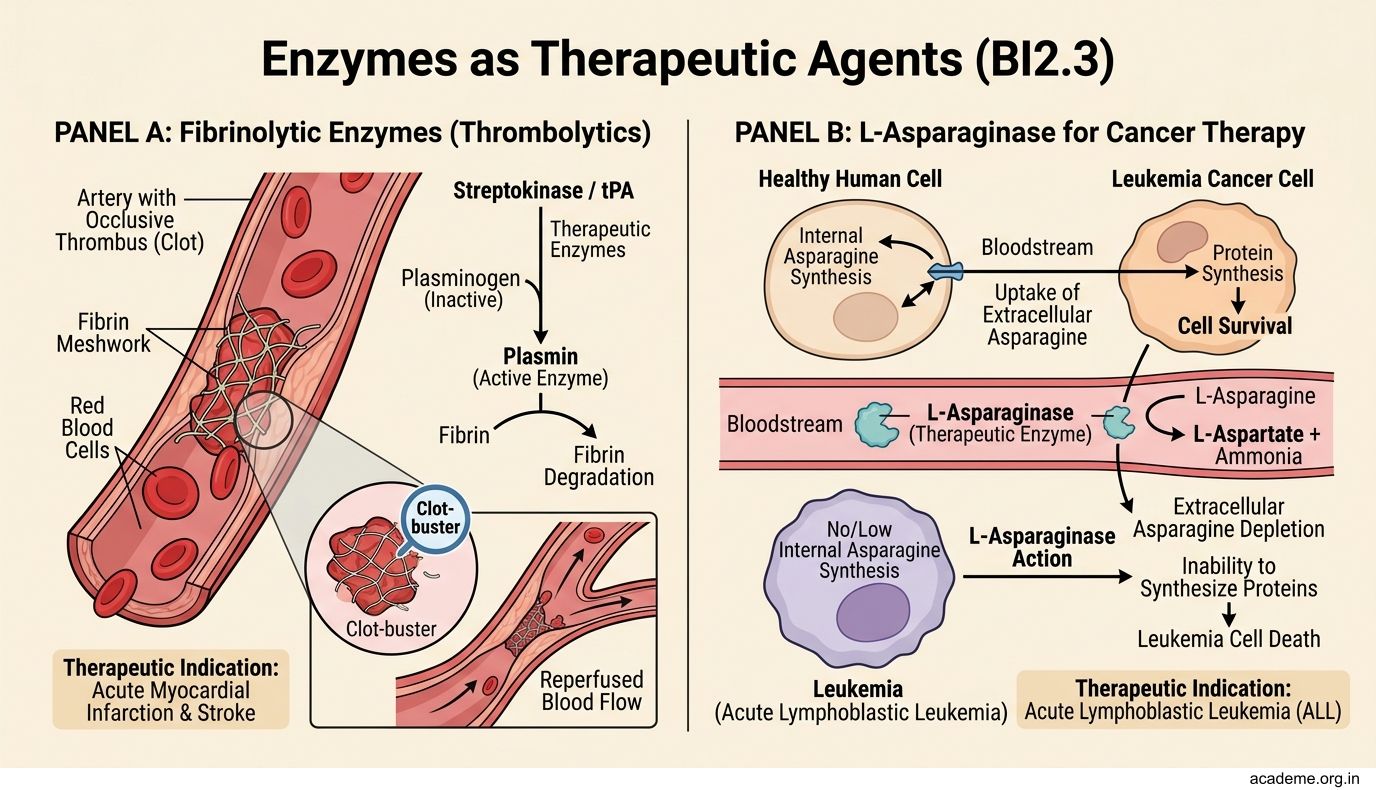
Enzymes aren't just drug targets — some are used as drugs themselves:
- Streptokinase and tissue plasminogen activator (tPA) — dissolve blood clots by activating plasminogen → plasmin, which digests fibrin. Used in acute myocardial infarction and stroke (the 'clot-buster' drugs).
- L-Asparaginase — breaks down asparagine (an amino acid). Some cancer cells (especially in acute lymphoblastic leukaemia, ALL) cannot synthesise asparagine and depend on blood supply. L-asparaginase starves these cancer cells.
- Pancreatic enzyme supplements (lipase, amylase, protease) — given to patients with chronic pancreatitis or cystic fibrosis who cannot produce enough digestive enzymes.
- α-Galactosidase (Beano®) — breaks down oligosaccharides in beans that humans can't digest, reducing flatulence.
Enzymes are also used therapeutically in enzyme replacement therapy for genetic enzyme deficiencies (e.g., imiglucerase for Gaucher disease, agalsidase for Fabry disease).
SELF-CHECK
A drug company develops a new cholesterol-lowering drug that competes with HMG-CoA for the active site of HMG-CoA reductase. How will this drug affect the enzyme's kinetics?
A. Km decreases, Vmax decreases — the enzyme is permanently damaged
B. Km is unchanged, Vmax decreases — some enzyme molecules are disabled
C. Km increases (apparent), Vmax is unchanged — more substrate can overcome the inhibition
D. Neither Km nor Vmax is affected — competitive inhibitors only work in vitro
Reveal Answer
Answer: C. Km increases (apparent), Vmax is unchanged — more substrate can overcome the inhibition
This is competitive inhibition — the drug competes with the real substrate for the active site. Km increases (you need more substrate to achieve ½Vmax because the inhibitor is blocking some active sites) but Vmax is unchanged (with enough substrate, you can outcompete the inhibitor and saturate all enzymes). This is exactly how statins work.
Clinical Enzymes — Serum Markers of Disease (BI2.4)
When cells are damaged or destroyed, their intracellular enzymes leak into the blood. By measuring these serum enzymes, doctors can identify which organ is damaged and how severely.
Here are the key diagnostic enzymes you must know:
Cardiac markers (Myocardial Infarction):
• Troponin I and T — the gold standard. Highly specific for heart muscle. Rises within 3–6 hours of MI, peaks at 12–24 hours, stays elevated for 7–14 days.
• CK-MB — rises within 4–6 hours, peaks at 24 hours, returns to normal by 72 hours. Useful for detecting re-infarction because it normalises quickly.
• LDH1 > LDH2 (flipped LDH) — rises late (24–48 hours), stays elevated for 7–10 days.
Liver function tests (LFTs):
• ALT (SGPT) — most specific for liver. Elevated in hepatitis, drug-induced liver injury.
• AST (SGOT) — found in liver, heart, and muscle. Less specific than ALT. The AST:ALT ratio (De Ritis ratio) helps differentiate: ratio >2 suggests alcoholic liver disease; ratio <1 suggests viral hepatitis.
• ALP (Alkaline Phosphatase) — elevated in obstructive jaundice (bile duct blockage) and bone disease (Paget's disease, rickets, bone metastases).
• GGT (Gamma-glutamyl transferase) — elevated in alcoholic liver disease and biliary obstruction. GGT + elevated ALP = biliary origin confirmed.
Pancreatic markers:
• Amylase — rises within hours of acute pancreatitis, returns to normal in 3–5 days.
• Lipase — more specific for pancreatitis than amylase, stays elevated longer (7–14 days).
Bone and prostate:
• Acid phosphatase — was previously used for prostate cancer (now replaced by PSA, which is not an enzyme).
• ALP (bone isoform) — elevated in bone diseases with increased osteoblast activity.
Interpreting Enzyme Results — Putting It Together (BI2.5)
Now let's practise the thinking process a doctor uses when looking at enzyme results:
Scenario 1: Chest pain + elevated Troponin + elevated CK-MB
→ Troponin is specific for heart muscle. CK-MB confirms cardiac origin. Diagnosis: Myocardial infarction.
Scenario 2: Jaundice + elevated ALT (500 U/L) + elevated AST (200 U/L) + normal ALP
→ Very high ALT + AST:ALT ratio <1 = acute viral hepatitis (hepatocyte damage releasing transaminases). Normal ALP rules out obstruction.
Scenario 3: Jaundice + mildly elevated ALT + very high ALP + elevated GGT
→ High ALP + high GGT = biliary obstruction (gallstone or tumour blocking the bile duct). GGT confirms the ALP is from bile duct, not bone.
Scenario 4: Severe abdominal pain + elevated lipase (10× normal) + elevated amylase
→ Very high lipase is highly specific for acute pancreatitis. Amylase confirms but is less specific (can be elevated in parotitis, intestinal obstruction).
Scenario 5: Chronic alcohol use + AST:ALT ratio of 2.5 + elevated GGT
→ AST:ALT ratio >2 + elevated GGT = classic pattern for alcoholic liver disease.
The pattern matters more than any single enzyme value. Always ask: Which organ do these enzymes come from? What is the ratio pattern? What does the clinical context suggest?