Page 8 of 15
CM9.4-6 | CM9.4-6 | Population Dynamics and Population Policy — SDL Guide
Learning Objectives
- Enumerate and describe the causes of population explosion in India and their health consequences
- Describe the concept of demographic dividend and India's current window of opportunity
- Describe and compare contraceptive methods — barrier, hormonal, IUD, permanent sterilisation, and emergency contraception — with mechanisms, efficacy, and reversibility
- Describe non-contraceptive determinants of population control: female education, age at marriage, women's empowerment
- Describe the National Population Policy 2000 — its goals (immediate, medium-term, long-term) and key strategies
- Apply population policy and contraceptive knowledge to primary health care counselling
INSTRUCTIONS
India is at a demographic crossroads. National fertility has reached replacement level, yet the population continues growing due to momentum from its youthful age structure. The decisions made now — on family planning services, female education, and social security — will determine whether India harvests its demographic dividend or squanders it. This module connects population theory to the frontline reality of primary health care: the contraceptive counselling conversation, the NPP 2000 targets you are expected to help achieve, and the family planning programme you will be part of.
References
- Park K. Parks Textbook of Preventive and Social Medicine, 26th ed., Ch. 2 — Demography and Family Planning (textbook)
- National Population Policy 2000, Ministry of Health and Family Welfare, Government of India (policy)
- National Family Health Survey (NFHS-5) 2019-21, Ministry of Health & Family Welfare, India (survey)
- Sample Registration System Statistical Report 2020, Registrar General of India (report)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
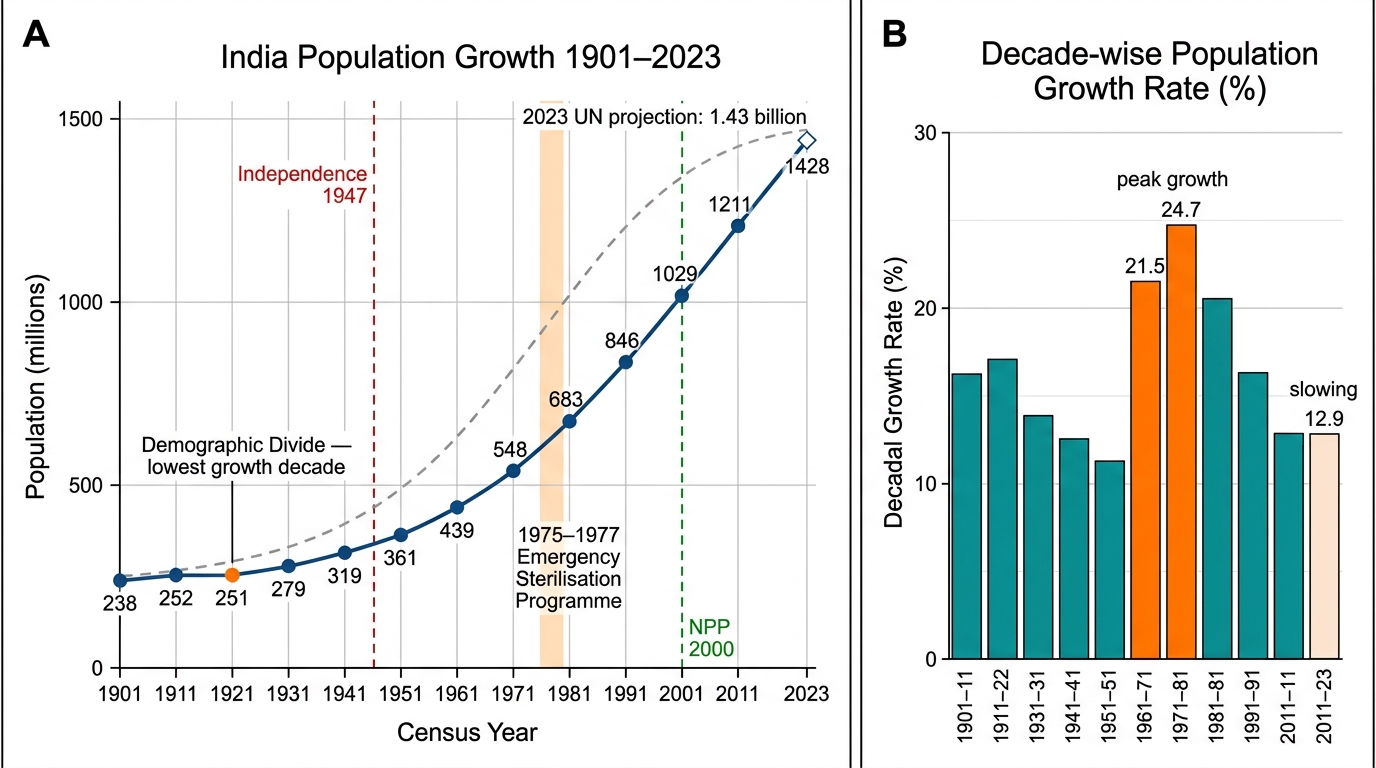
In 1901, India's population was 238 million. By 1947, it had grown to 340 million. By 1975, it crossed 600 million — prompting the Emergency-era sterilisation programme that coercively sterilised an estimated 6-8 million people in a single year, a catastrophic policy failure that set back voluntary family planning in India by a generation. By 2011 it reached 1.21 billion, and by 2023 — 1.43 billion. Yet here is the paradox: India's national Total Fertility Rate has reached 2.0 (NFHS-5, 2019-21), at replacement level. The population is still growing, but because of momentum from its existing age structure, not because fertility is uncontrolled. How did we get here? What works in population control, and what catastrophically doesn't? And what does the National Population Policy 2000 ask of you, the future primary health care physician, in the next decade of community service?
WHY THIS MATTERS
Population control is not a historical subject — it is live policy. India's National Population Policy 2000 established specific targets that the health system is still working toward. The contraceptive prevalence rate in India (modern methods) is approximately 56.5% among married women aged 15-49 (NFHS-5), meaning over 40% of women who are or could be fertile are not protected by modern contraception. The unmet need for family planning — women who want to space or limit births but are not using contraception — is approximately 9.4% nationally (NFHS-5). These are the women you will encounter in your PHC's antenatal clinic, your immunisation camp, and your community outreach visits. Knowing the contraceptive options, their mechanisms, their side effects, and their non-contraceptive benefits — and knowing how to counsel a couple in the context of their specific fertility desires, health status, and cultural context — is a core clinical competency. This module gives you the foundation.
RECALL
From previous modules, recall: (1) India's population follows the demographic transition model — Stage 2 to Stage 3-4 over the 20th century. (2) The Total Fertility Rate (TFR) is the average lifetime births per woman at current age-specific rates; replacement level TFR ≈ 2.1. (3) The crude birth rate and crude death rate determine the rate of natural increase. (4) From first-year Physiology, recall the hypothalamic-pituitary-ovarian axis — this is the mechanism that hormonal contraceptives target. (5) Population momentum means that even after a population achieves replacement-level TFR, it continues growing for decades because the large existing cohort of young women continues to bear children (at replacement rate) — the growth has been 'pre-programmed' by the youthful age structure.
India's Population Explosion: Scale and Consequences
The term population explosion refers to the rapid and unprecedented growth of human populations during the 20th century, driven by a combination of declining mortality and persistently high fertility — characteristic of Stage 2 of the demographic transition. For India, the explosion began in earnest in the 1920s-1930s, when improvements in famine management, plague control, and basic public health began to lower the CDR without any corresponding fall in the CBR. The annual growth rate peaked at approximately 2.2% per year in the 1970s-80s — meaning India was doubling its population in approximately 31 years.
The trajectory in absolute numbers is striking: 238 million in 1901, 340 million in 1947, 548 million in 1971, 683 million in 1981, 1.03 billion in 2001, 1.21 billion in 2011, and approximately 1.43 billion in 2023. India surpassed China as the world's most populous nation in 2023 — a milestone driven not by continued high fertility (India's TFR is now at replacement) but by the momentum of its earlier demographic trajectory and its younger median age compared to China.
The health consequences of population explosion are pervasive and multi-systemic. At the healthcare system level, rapid population growth outpaces the expansion of health infrastructure: physician-to-population ratios, bed-to-population ratios, and vaccine coverage all suffer when the denominator grows faster than the numerator. At the individual level, closely spaced births (birth-to-birth interval less than 24 months) are independently associated with higher infant and maternal mortality — malnutrition, anaemia, and obstetric complications are more common when women have insufficient recovery time between pregnancies. At the community level, overcrowding in urban areas drives infectious disease transmission, water and sanitation overload, and mental health burden. At the national level, rapid population growth has historically been associated with lower GDP per capita growth because a larger fraction of national income must be directed to 'maintaining' the population (food, basic education, basic health) rather than investing in productivity-enhancing infrastructure.
India's Population Trajectory 1901–2023: Census Data, Milestones, and Decadal Growth Rates
Causes of Population Explosion and Dynamics
The proximate and distal causes of India's population explosion can be organised into three interacting domains: biological-demographic, socioeconomic, and health system factors. Understanding this causal structure is essential for designing effective population policy — interventions must target the right points in the causal chain to be effective.
The demographic causes are structural. India's Stage 2 transition (rapidly falling CDR, persistently high CBR) produced the initial growth surge. Once a large cohort of young people is born, population momentum ensures continued growth even after fertility falls: the 1980-2000 birth cohort — now in their 20s and 30s — continues producing children at replacement rate, but because this cohort is so numerically large, the absolute number of births remains high. This mathematical momentum is the reason India's population continues growing despite a national TFR of 2.0.
The socioeconomic causes of high fertility include:
- Son preference: the desire for male children leads families to keep having children until they achieve their desired number of sons. In communities with strong son preference, families with two daughters have a much higher probability of a third birth than families with two sons.
- Low female education: female literacy is the strongest socioeconomic predictor of fertility decline. Women with no education have a TFR approximately 3-4 times higher than women with secondary or higher education, across multiple NFHS rounds. Education delays age at marriage, raises women's opportunity cost of time, and empowers reproductive decision-making.
- Early age at marriage: India's legal minimum age at marriage is 18 for women and 21 for men (Child Marriage (Amendment) Bill 2021 proposes 21 for both). Despite legal prohibition, child marriage persists, particularly in rural Rajasthan, Bihar, and UP. Earlier marriage extends the reproductive window, increasing lifetime births even without higher ASFR at each age.
- Inadequate social security: in the absence of formal pension systems, children — particularly sons — are the primary old-age security for rural households. High child mortality historically drove high fertility as insurance against losing children.
- Inadequate family planning access: unmet need for contraception (9.4% nationally, NFHS-5) means that approximately 8-10 million women who wish to avoid pregnancy are not using effective contraception.
The health system causes include provider bias against certain contraceptive methods (historically, permanent sterilisation was overemphasised at the expense of spacing methods, creating coercion risk), poor ASHA training in contraceptive counselling, and supply chain failures for pills and condoms at peripheral facilities.
SELF-CHECK
India's national TFR is 2.0 (at replacement level) but the population is still growing. Which concept best explains this?
A. The CDR is rising, cancelling out the falling TFR
B. Population momentum — the large existing cohort of young women continues bearing children at replacement rate, sustaining high absolute birth numbers
C. The TFR data is wrong — actual fertility is higher than 2.0 in rural areas
D. Immigration from neighbouring countries is driving population growth
Reveal Answer
Answer: B. Population momentum — the large existing cohort of young women continues bearing children at replacement rate, sustaining high absolute birth numbers
Population momentum is the phenomenon where a population continues to grow even after TFR falls to replacement level (2.1), because the large cohort of women born during the earlier high-fertility era is now of reproductive age. Even at a TFR of 2.0 (replacement), each of these women produces approximately 2 children — but because there are so many of them, absolute births remain high. The population will only stabilise after this large cohort ages past reproductive age — a process that takes 20-30 years. This is why India's population will continue growing until approximately 2050-2060 even though TFR has effectively reached replacement.
Methods of Population Control
Population control methods fall into two broad categories: contraceptive methods (which prevent conception or implantation) and non-contraceptive determinants (socioeconomic factors that reduce fertility without explicit contraceptive use). An effective national population policy addresses both — contraceptive access without female empowerment and education produces incomplete fertility decline, as demonstrated by India's own historical experience.
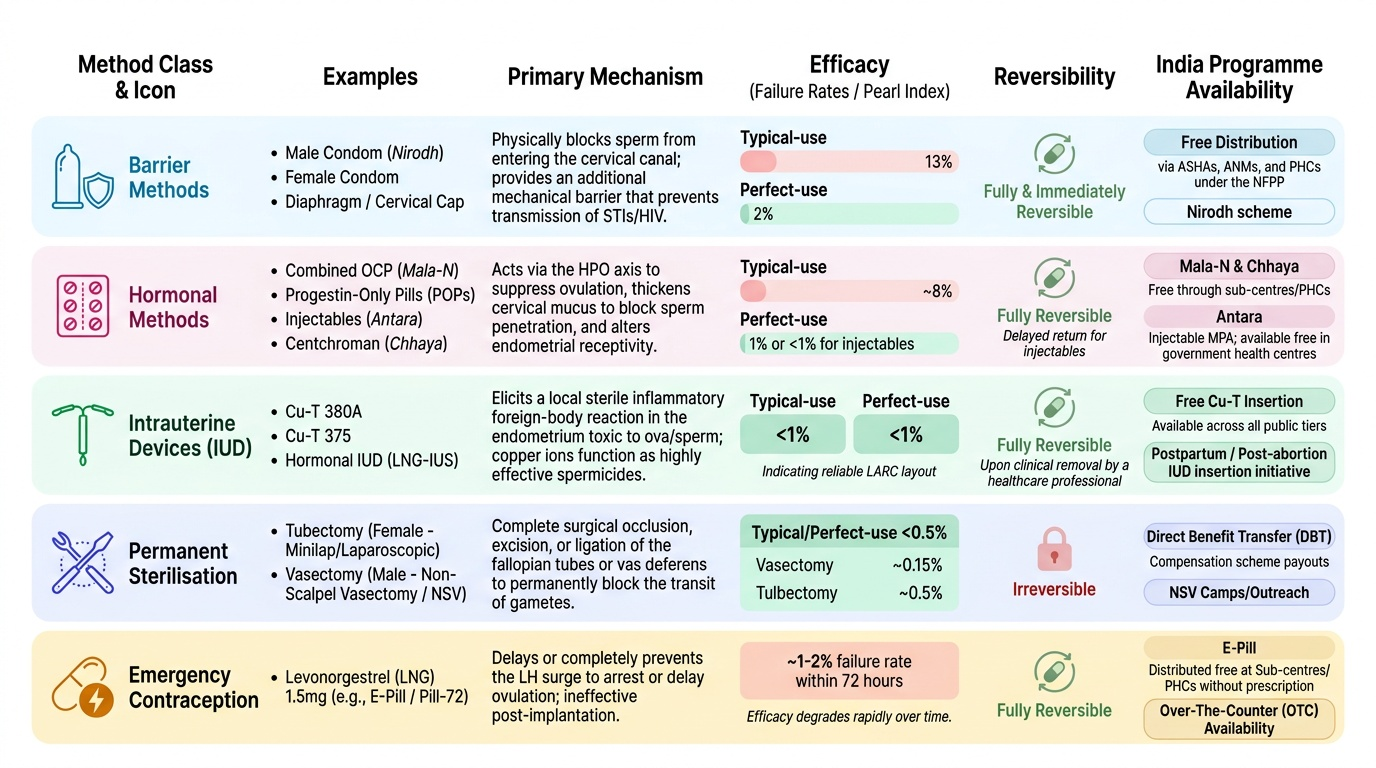
Barrier methods physically prevent sperm from reaching the egg. The male condom is the most widely used barrier method in India's public health system — it is freely distributed through ANMs, ASHAs, and PHC pharmacies, and has the additional benefit of STI/HIV prevention. Typical-use failure rate is approximately 13% (13 pregnancies per 100 woman-years); perfect-use rate is 2%. The female condom is available but underused in India. The diaphragm and cervical cap require fitting and are rarely used in India's public health context.
Hormonal methods act via the hypothalamic-pituitary-ovarian axis to suppress ovulation (combined methods), thicken cervical mucus (both combined and progestin-only), and alter endometrial receptivity. The combined oral contraceptive pill (OCP) contains synthetic oestrogen + progestin; perfect-use failure rate <1%, typical-use ≈8%. Contraindications include hypertension, DVT risk, migraines with aura, and breastfeeding (within 6 months postpartum — use progestin-only). The progestin-only pill (POP or mini-pill) is safe for breastfeeding women. Injectable contraceptives — DMPA (Depot Medroxyprogesterone Acetate, 'Antara' programme in India, 3-monthly injection) — offer high efficacy with long duration; suitable for women who want spacing without daily adherence. Implants (subdermal progestin rods, 3-5 years) offer very high efficacy but require trained insertion/removal providers.
Intrauterine Devices (IUDs): The copper IUD (Cu-T 380A) is a non-hormonal device that works primarily by creating a spermicidal copper ion environment; effective for 10-12 years; can also be used as emergency contraception within 5 days of unprotected intercourse. The levonorgestrel IUS (Mirena) releases progestin locally, causing endometrial suppression and cervical mucus thickening; effective for 5 years; reduces menstrual blood loss (benefit in anaemic women). Both require skilled insertion; contraindicated in active pelvic infection and distorted uterine cavity.
Permanent methods (sterilisation): Vasectomy (male) is the simpler, safer, and less expensive procedure — a 15-minute outpatient procedure under local anaesthesia. Despite this, India's national family planning programme has historically over-relied on tubectomy (female), reflecting gender inequity in programme design. India's tubectomy rate is among the highest in the world. Both are intended as permanent; reversal success rates are limited. The historical Emergency-era forced sterilisation programme (1975-77) created lasting distrust; voluntary informed consent is now the cornerstone of India's programme.
Emergency contraception pills (ECPs): Levonorgestrel 1.5 mg taken as a single dose within 72 hours of unprotected intercourse (efficacy falls with delay; some evidence of partial efficacy up to 120 hours). ECPs act primarily by delaying or inhibiting ovulation — they are not abortifacient if taken after a fertilised egg has already implanted. ECPs are not intended for regular contraception. Available over the counter in India as 'I-Pill,' 'Unwanted-72,' etc.
Non-contraceptive determinants: Female education is the most powerful non-contraceptive fertility determinant — every additional year of schooling for a girl is associated with later age at first birth, fewer total births, and better child survival. The PCPNDT Act and Beti Bachao Beti Padhao address sex-selective abortion and gender equity. Age at marriage legislation (minimum 18 for women) reduces fertility by compressing the reproductive window.
Provided image