Page 1 of 11
CM13.{1-2,4} | CM13.{1-2,4} | Disaster Concepts, Cycle and Authority — SDL Guide
Learning Objectives
- Define disaster and distinguish natural from man-made disasters with examples relevant to India
- Describe the four phases of the disaster management cycle and the key activities within each phase
- Explain the structure, statutory basis, and mandate of the National Disaster Management Authority (NDMA) and its subordinate bodies
- Identify the physician's role within the disaster management framework at the district and community level
INSTRUCTIONS
India loses thousands of lives to disasters every year — from cyclones on the eastern coast to floods in the Brahmaputra basin, from industrial accidents to seismic events in the Himalayan foothills. As a community physician you will be posted to a district that is almost certainly disaster-prone in some way. Understanding how disasters are defined, classified, and managed — and knowing which authority has legal responsibility for what — is foundational clinical community medicine. This module equips you with that framework.
References
- Park's Textbook of Preventive and Social Medicine, 27th Edition — Chapter on Disaster Management (textbook)
- Disaster Management Act, 2005 (Act 53 of 2005), Government of India (statutory)
- National Disaster Management Guidelines, NDMA, Government of India (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The date is 26 December 2004. You are a junior doctor completing your posting in a coastal district of Tamil Nadu. At 9:15 AM, the sea retreats — inexplicably, dramatically — from the shore. Fishermen walk out to collect stranded fish. Within minutes the water returns as a wall. The Indian Ocean tsunami has begun. By evening, your district hospital is overwhelmed with over 400 casualties, the power is out, the roads are submerged, and your phone shows no signal. You have received no training in disaster response. The district administration has no documented plan. Relief agencies are arriving but no one knows who is in charge. Thousands of preventable deaths will occur in the next 72 hours — not from the wave, but from the chaos that follows.
Today, we ask: if you were that doctor again, what would you know?
WHY THIS MATTERS
India is one of the world's most disaster-prone countries. Its geography places it at risk from virtually every category of natural disaster: earthquakes along the Himalayan belt, cyclones on both coasts, floods across the river plains, droughts in the arid zones, and landslides in the hilly states. Man-made disasters — industrial accidents, chemical leaks, epidemics — add to this burden. Disasters kill, injure, and displace millions; they collapse health infrastructure at exactly the moment that infrastructure is most needed. The 2004 tsunami killed over 10,000 Indians; the 2013 Uttarakhand floods over 5,000. Every community physician posted to a district will, at some point in their career, face a disaster — or the threat of one. The disaster management cycle and India's statutory authority framework are not administrative curiosities. They are the operational toolkit you will reach for in that moment.
RECALL
Before we build the disaster management framework, let us activate relevant prior knowledge. From your earlier community medicine modules, you know that epidemiological surveillance involves systematically detecting disease events above expected thresholds — a concept directly applicable to detecting biological disasters. From your health systems modules, you know that district health administration operates through the District Collector and the Chief Medical Officer — these very officials become the operational arms of disaster response. From preventive medicine, you know that primary prevention (reducing hazard or vulnerability) and secondary prevention (early detection and rapid response) apply equally to disease and to disaster. Keep these frameworks in mind as we build the disaster-specific overlay.
Global and Indian Burden of Disasters
Disasters impose an enormous and disproportionate burden on low- and middle-income countries, including India. Globally, the UNDRR (United Nations Office for Disaster Risk Reduction) estimates that between 2000 and 2019, disasters affected 4.2 billion people and caused economic losses exceeding USD 2.97 trillion. India accounts for a significant share of this burden: it ranks among the most disaster-prone countries in the world, owing to its vast geography, high population density, and rapid urbanisation in hazard-prone zones.
Within India, the northeastern states lie in Seismic Zone V (highest earthquake risk); the coastlines of Odisha, Andhra Pradesh, and Tamil Nadu are regularly struck by tropical cyclones; the Brahmaputra and Ganges plains experience annual flooding; Rajasthan and parts of Maharashtra face recurring droughts. The 2001 Bhuj earthquake killed over 20,000 people. The 2004 Indian Ocean tsunami killed approximately 10,000 Indians on the southern coastline. The 2013 Uttarakhand cloud-burst floods killed over 5,000 and displaced hundreds of thousands.
Disaster burden is not measured only in deaths. It is measured in the years of healthy life lost (DALYs — disability-adjusted life years), in the economic losses that push households back into poverty, and in the destruction of health infrastructure that reverberates for years. The health impact of disasters falls on multiple levels: direct trauma and drowning deaths; disease outbreaks in the post-disaster period (cholera, leptospirosis, malaria in flooded areas); mental health consequences (post-traumatic stress, grief, displacement); and long-term nutritional and developmental impacts on children. This cumulative burden is why disaster management is a core community medicine competency, not a peripheral elective.
Definition and Classification of Disasters
A disaster is defined by the United Nations as a serious disruption of the functioning of a community or society that exceeds its capacity to cope using its own resources, resulting in human, material, economic, or environmental losses and impacts. The key elements of this definition are instructive: (1) disruption must be serious, not merely disruptive; (2) the community's own coping capacity must be exceeded — this is what distinguishes a disaster from a major accident or an emergency; and (3) the consequences span multiple dimensions — human lives, physical assets, economic activity, and environmental integrity.
India's Disaster Management Act 2005 defines a disaster as a catastrophe, mishap, calamity or grave occurrence in any area arising from natural or man-made causes, or by accident or negligence, which results in substantial loss of life or human suffering or damage to, and destruction of, property, or damage to or degradation of environment, and is of such a nature or magnitude as to be beyond the coping capacity of the community of the affected area.
Disasters are classified into two broad categories based on their origin:
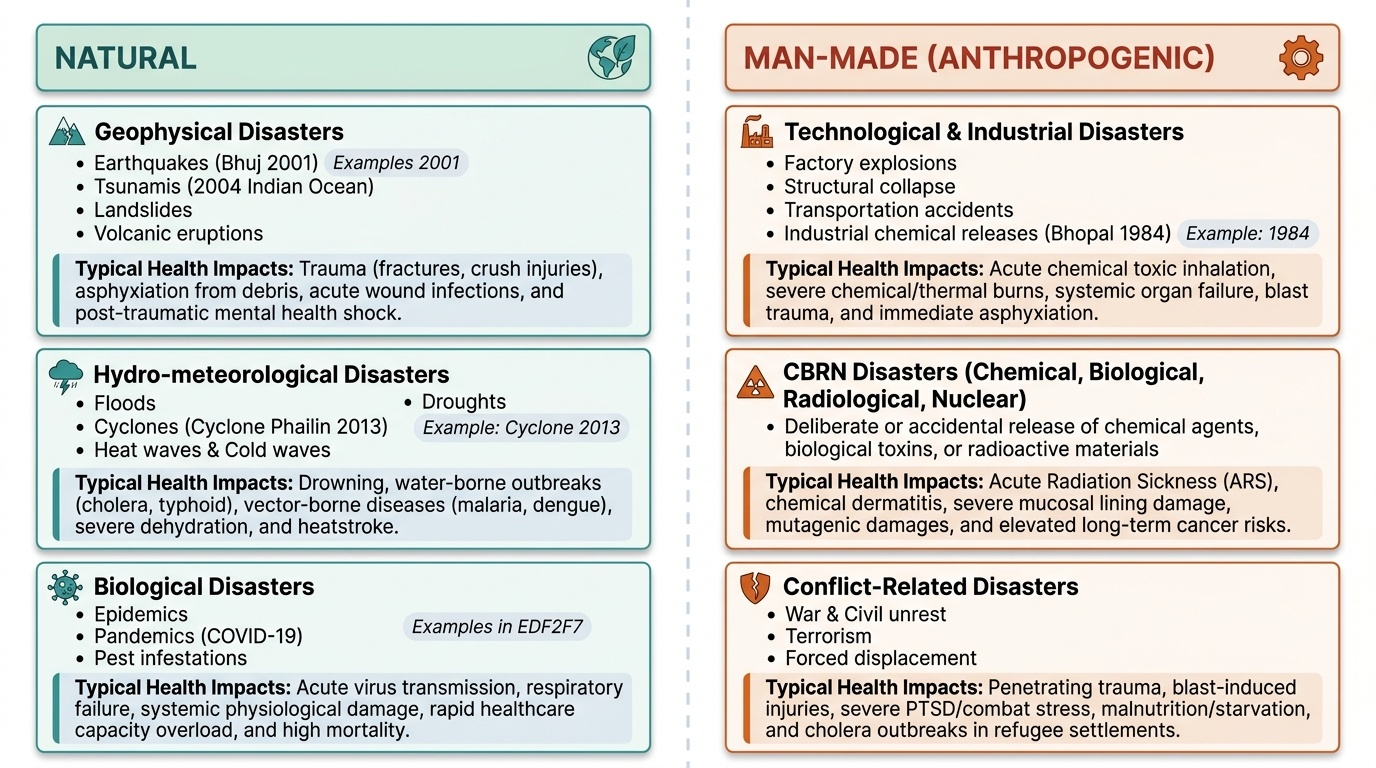
Natural disasters arise from geophysical, hydro-meteorological, or biological processes:
- Geophysical: earthquakes (Bhuj 2001), volcanic eruptions, tsunamis (2004 Indian Ocean), landslides
- Hydro-meteorological: floods, cyclones (Cyclone Phailin 2013), droughts, heat waves, cold waves
- Biological: epidemics, pandemics (COVID-19), pest infestations
Man-made (anthropogenic) disasters arise from human activity or negligence:
- Technological/industrial: factory explosions, structural collapse, transportation accidents, industrial chemical releases (Bhopal 1984)
- Chemical, biological, radiological, or nuclear (CBRN): deliberate or accidental release of CBRN agents
- Conflict-related: war, terrorism, civil unrest, forced displacement
The determinants of disaster impact — why the same hazard causes very different levels of harm in different communities — include: exposure (number and vulnerability of people in the hazard zone), vulnerability (poverty, poor housing, lack of early warning systems, inadequate health infrastructure), and capacity (institutional, financial, and community-level preparedness). Reducing vulnerability and building capacity are the twin levers of disaster risk reduction — and they are fundamentally public health activities.
Provided image
SELF-CHECK
According to the Disaster Management Act 2005, which of the following BEST captures what makes an event qualify as a 'disaster' rather than a major emergency?
A. A. The event results in more than 50 deaths
B. B. The event exceeds the local community's own coping capacity
C. C. The event is declared by the State government
D. D. The event involves a natural cause such as earthquake or flood
Reveal Answer
Answer: B. B. The event exceeds the local community's own coping capacity
The legal and operational definition of a disaster hinges not on a fixed death toll or declaration, but on whether the event exceeds the community's own coping capacity — requiring external support. A government declaration may follow, but it is not the defining criterion. The cause (natural vs man-made) determines classification, not whether it qualifies as a disaster.
The Disaster Management Cycle
The disaster management cycle is the foundational operational model for understanding how society prepares for, responds to, and recovers from disasters. It is best understood as a closed loop: the lessons learned from recovery feed back into improved mitigation and preparedness for the next event. The cycle has four phases, and understanding their sequence and inter-relationships is essential for planning.
Phase 1 — Mitigation occurs continuously, primarily before a disaster strikes, but also between disasters. Mitigation refers to actions that reduce the risk of a disaster or reduce its severity if it occurs. It encompasses structural measures (earthquake-resistant building codes, flood embankments, cyclone shelters) and non-structural measures (land-use zoning to keep settlements away from flood plains, early warning systems, insurance schemes, community awareness). Mitigation is the most cost-effective phase: a rupee spent on mitigation saves multiple rupees in response and recovery. In India, NDMA's National Disaster Management Guidelines specify mitigation priorities for each hazard type.
Phase 2 — Preparedness also occurs before the disaster, but is activated more intensively as hazard risk increases (e.g., cyclone season). Preparedness includes: contingency planning (documented response plans at district and state levels), resource stockpiling (medicines, food, rescue equipment), training of emergency response personnel, public awareness and community drills, and establishment of early warning systems. A key preparedness measure in health is the Health Emergency Operations Centre (HEOC) and pre-positioning of rapid response teams.
Phase 3 — Response is the immediate action phase — during and immediately after the disaster strikes. Response activities include: search and rescue, triage and emergency medical care, evacuation, establishment of relief camps, food and water distribution, and restoration of essential services. The golden hours principle applies: rapid response in the first 24–72 hours saves the most lives. Effective response depends entirely on the quality of preparedness — a community that has planned, trained, and stockpiled will respond far more effectively than one that has not.
Phase 4 — Recovery begins once the acute response phase is stabilised and continues until the community returns to normal functioning — or better. Short-term recovery involves: temporary shelter, restoration of water supply and sanitation, resumption of health services, and psychosocial support. Long-term recovery (reconstruction) involves: rebuilding housing and infrastructure to higher standards, restoring livelihoods, and rehabilitating mental health. Critically, recovery is an opportunity to build back better — incorporating disaster-risk reduction into reconstruction so the community is less vulnerable to the next event.
| Phase | Timing | Key Activities | Indian Example |
|---|---|---|---|
| Mitigation | Pre-disaster, continuous | Building codes, land-use zoning, early warning | Cyclone shelters on Odisha coast |
| Preparedness | Pre-disaster, ongoing | Contingency plans, drills, stockpiling, HEOCs | NDRF mock drills before monsoon |
| Response | During + immediately post | SAR, triage, evacuation, relief | Uttarakhand 2013 multi-agency rescue |
| Recovery | Post-disaster | Shelter, livelihood restoration, rebuild | Post-Bhuj reconstruction 2001–2004 |
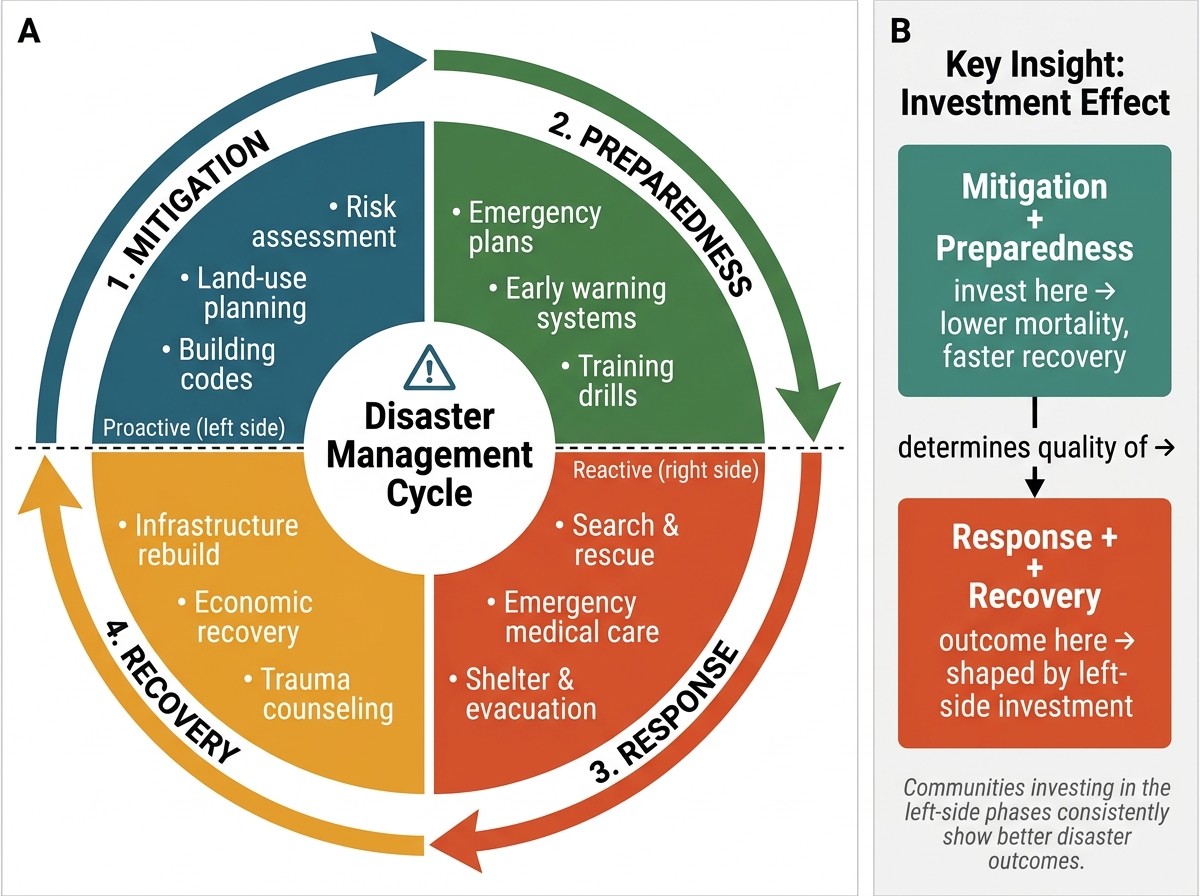
The Four-Phase Disaster Management Cycle and the Investment Effect
The cycle's most important insight is that response quality is set during preparedness, and preparedness quality is set during mitigation and recovery. Communities that invest in the left side of the cycle (mitigation and preparedness) consistently show lower mortality and faster recovery when disaster strikes.