Page 5 of 11
CM13.{3,5} | CM13.{3,5} | Man-made Disasters and Simulated Response — SDL Guide (Part 2)
Medical Countermeasures and Decontamination in Man-Made Disasters
Man-made disasters — particularly those involving chemical or radiological agents — require two medical response priorities beyond standard trauma care: decontamination (removing the hazard from the casualty before it spreads) and specific medical countermeasures (antidotes or protective agents targeting the specific hazardous agent).
Decontamination is the process of removing contaminating substances from casualties, responders, and equipment. It must occur BEFORE contaminated casualties enter the medical treatment area — failure to decontaminate allows the hazardous agent to spread to health workers, other casualties, and the healthcare facility itself. This is not a theoretical risk: in chemical incidents, responders have been incapacitated by secondary exposure from undecontaminated casualties. Decontamination is performed in a dedicated decontamination corridor established upwind and upstream of the medical treatment area. The corridor has three zones: the hot zone (contaminated — only fully equipped responders enter), the warm zone (decontamination — casualties are undressed, brushed/washed, and re-assessed), and the cold zone (clean medical treatment area). For chemical agents, decontamination involves: removal of clothing (which removes approximately 80% of surface contamination), followed by copious water flushing; for radiological agents, similar wet decontamination is used, with radiation monitoring to confirm adequate decontamination before entry to the cold zone.
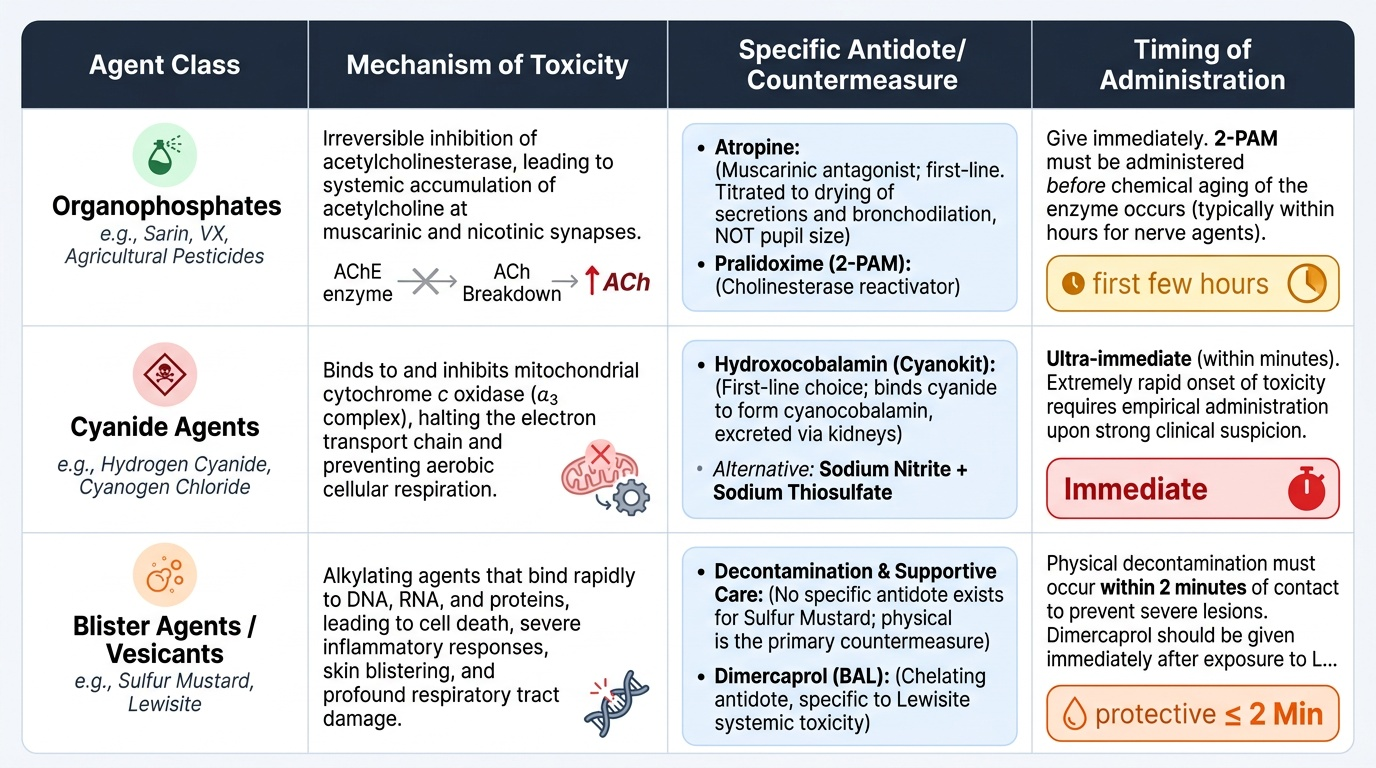
Medical countermeasures by agent class are as follows:
For organophosphate chemical agents (including nerve agents such as sarin and VX, as well as agricultural organophosphate pesticides — the most common chemical disaster in India): the mechanism is irreversible inhibition of acetylcholinesterase, causing accumulation of acetylcholine at muscarinic and nicotinic synapses. Treatment: atropine (muscarinic antagonist — the first-line antidote, given in large doses titrated to drying of secretions and bronchodilation, NOT to pupil size), plus pralidoxime (2-PAM) (oxime that reactivates inhibited cholinesterase — effective only if given before ageing, which occurs within hours for sarin but may take longer for agricultural organophosphates).
For cyanide agents (hydrogen cyanide, cyanogen chloride): mechanism is inhibition of cytochrome c oxidase, blocking cellular respiration (cellular asphyxia despite adequate blood oxygenation). Casualty presents with: altered consciousness, metabolic acidosis, high venous oxygen saturation (cells cannot use delivered oxygen). Antidote: hydroxocobalamin (binds cyanide to form cyanocobalamin — given IV, now preferred over the older methemoglobin-producing kit).
For radiological/nuclear exposure: no antidote for radiation itself. Management includes: thyroid protection with potassium iodide (KI) (for radioiodine-131 exposure — blocks thyroid uptake; must be given within hours of exposure to be effective), G-CSF (granulocyte colony-stimulating factor — for bone marrow suppression after high-dose whole-body radiation), and symptomatic supportive care for acute radiation syndrome.
The NDRF maintains specialised CBRN response teams with training in all these countermeasures, decontamination protocols, and protective equipment. District hospitals in disaster-prone areas should maintain a CBRN decontamination kit and an antidote formulary for the most likely regional hazards (organophosphates for agricultural areas; industrial chemicals for areas near chemical plants).
Provided image
SELF-CHECK
In a chemical mass casualty incident involving a nerve agent (organophosphate), decontamination of casualties MUST occur at which point in the response sequence?
A. A. After triage has been completed for all casualties
B. B. Before contaminated casualties enter the medical treatment area
C. C. After administration of the initial dose of atropine
D. D. Only for casualties in the RED (immediate) triage category
Reveal Answer
Answer: B. B. Before contaminated casualties enter the medical treatment area
Decontamination MUST occur before any contaminated casualty enters the medical treatment (cold zone) area, regardless of triage category. This is non-negotiable — failure to decontaminate allows secondary exposure of health workers and other casualties. Decontamination happens in the warm zone (the decontamination corridor), which is separate from and upstream/upwind of the treatment area. It is not triage-category-dependent; even GREEN (minor) casualties who are contaminated must be decontaminated before treatment.
Evaluating Simulated Disaster Response
The competency CM13.5 specifies that medical graduates must be 'able to understand the management of handling a disaster in a simulated environment.' The use of the word simulated is deliberate — it reflects the pedagogical consensus that disaster medicine skills cannot be learned from textbooks alone. They must be practised in realistic scenarios where learners experience the cognitive load, time pressure, and interpersonal coordination demands of a real event.
Simulation-based learning in disaster medicine typically takes the form of tabletop exercises (scenario discussion without physical enactment — efficient for planning review), functional exercises (communication and coordination tested without physical movement of resources), and full-scale exercises (physical enactment with actors playing casualties, resource mobilisation, field operations — the most realistic but most resource-intensive). NDMA guidelines mandate annual full-scale multi-agency mock drills at the district level.
A well-designed disaster simulation is evaluated against predefined performance criteria:
- Triage accuracy: what proportion of casualties were correctly categorised? A common error is undertriage (assigning a RED casualty to YELLOW — the dangerous error, as it delays life-saving care) and overtriage (assigning a YELLOW casualty to RED — the safe error, which wastes resources but does not cause direct harm). START triage, applied correctly, achieves undertriage rates of approximately 5–10% in simulation studies.
- Response time: time from disaster notification to first medical team activation; time from scene arrival to triage completion; time from triage to RED-category treatment initiation.
- Command and coordination: was ICS activated? Was unified command established between agencies? Were communication protocols followed?
- Decontamination protocol compliance: for chemical scenarios, was the decontamination corridor established before treatment? Were health workers using appropriate PPE?
- Documentation: were triage tags applied correctly? Were medical records started for each casualty? Was data transmitted to the hospital receiving the evacuated casualties?
After-action review (AAR) of simulation exercises uses the same four-question structure as post-real-disaster review: What was planned? What happened? Why the difference? What to change? Crucially, a simulation AAR should be conducted by the exercise director within 24–48 hours while memory is fresh, and findings must be documented and incorporated into updated response plans.
For the medical student and junior doctor, the learning objectives of disaster simulation participation include: experiencing triage decision-making under time pressure; practising ICS communication (SBAR — Situation, Background, Assessment, Recommendation — is the standard format); and reflecting on personal cognitive limitations under stress — a form of professional self-awareness that improves real-event performance.
Applying Response Skills in a Simulated Environment
The application of disaster response knowledge in practice requires integrating the conceptual frameworks (ICS, START triage, decontamination, countermeasures) into rapid, team-coordinated action under the kinds of time and resource constraints that characterise real events. This section outlines the physician's specific tasks in a simulated mass casualty incident and connects them to the broader NDMA framework.
When you arrive at a simulated MCI scene, your first actions follow a structured sequence. Scene safety is assessed first: identify the nature of the hazard (chemical, blast, structural), determine whether the hot zone has been secured, confirm that you are in the cold zone before beginning patient contact. If you are not in appropriate PPE for the hazard type, you do not enter the hot or warm zone — a contaminated or injured physician is a liability, not a resource.
Triage is initiated immediately using START. As triage officer, you move rapidly through the scene, applying colour-coded tags, not treating. The triage officer's role is to categorise and direct — not to stop and treat, even a compelling RED casualty. Treatment begins in the treatment area (cold zone), not at the point of discovery.
Communication with the Incident Commander uses the SBAR format: 'Situation — I have completed initial triage: 12 RED, 22 YELLOW, 13 GREEN, 3 BLACK. Background — the majority of RED casualties have blast injuries with uncontrolled haemorrhage. Assessment — we need 3 additional surgeons and 8 additional nurses to the RED treatment area. Recommendation — request immediate activation of DDMA health annex and notification of the tertiary care centre for surgical capacity.'
Chain of evacuation is coordinated with the transport officer: RED casualties are evacuated first to the hospital with the highest surgical capacity; YELLOW casualties follow; GREEN casualties are directed to peripheral health facilities. The transport officer maintains a log of all evacuated casualties and their destination — this is how missing person reports are resolved in the aftermath.
Activation of post-disaster surveillance is initiated from the first hours, even while acute response continues. The public health officer (or the physician serving that role) activates the district surveillance system for: wound infections in the post-acute period; communicable disease outbreaks in relief camps; mental health presentations in the days following the event. This function is easy to defer and difficult to restart once the acute phase has passed — which is why it must be activated as a planned step, not an afterthought.
Park's textbook emphasises that disaster preparedness is a professional responsibility of the community physician — not an optional interest. The competency CM13.5 formalises this by requiring functional simulation-based training. The physician who has participated in at least one well-designed MCI simulation is demonstrably better prepared to function in a real event: they have experienced the cognitive load, practised triage decisions, and formed the team relationships that enable coordinated response.
For Year 3 students at the point of joining clinical postings: you should know the START algorithm by heart, be able to describe the ICS structure to a colleague, and be able to locate the decontamination protocol in your district hospital's emergency plan. These are minimum functional skills for a community physician in India's disaster-prone geography.
SELF-CHECK
During a simulated mass casualty incident, a 28-year-old male casualty is breathing 34 times per minute, has a capillary refill time of 1.5 seconds, and can follow commands. Using START triage, which category does he receive?
A. A. GREEN — he can follow commands, so he is walking wounded
B. B. RED — his respiratory rate exceeds 30/minute, meeting the RED criterion
C. C. YELLOW — his perfusion and mental status are normal, so he is delayed
D. D. BLACK — high respiratory rate suggests severe injury with poor prognosis
Reveal Answer
Answer: B. B. RED — his respiratory rate exceeds 30/minute, meeting the RED criterion
In START triage, the RED category is assigned if ANY of three criteria is met: respiratory rate > 30/min, capillary refill > 2 seconds (or radial pulse absent), or inability to follow simple commands. This patient has a respiratory rate of 34/min — which exceeds the threshold of 30/min — so he receives RED (immediate) even though his perfusion and mental status are normal. The RED threshold is applied as an OR condition, not an AND: meeting any single criterion assigns RED. The fact that he can follow commands does not override an abnormal respiratory rate.
CLINICAL PEARL
The most dangerous triage error is undertriage, not overtriage. In a mass casualty incident, placing a truly RED casualty in the YELLOW category (undertriage) means that person does not receive life-saving intervention in time — and dies preventably. Overtriage (placing a YELLOW casualty in RED) wastes resources but does not kill. START triage, applied rigorously, achieves undertriage rates of 5–10% in simulation — imperfect but acceptable. The most common cause of undertriage is over-reassurance by a calm demeanour — a casualty who is alert and apparently stable but has a respiratory rate of 32 or absent radial pulse is RED, not YELLOW. Always complete all three START assessments before assigning category, even for apparently stable casualties. The second most common cause: triage creep — the triage officer stops to treat a compelling casualty and loses track of the remaining untriaged patients. The triage officer's role is categorise-and-move, not treat.