Page 1 of 20
CM8.1 | CM8.1 | Communicable Disease Control at Primary Care — SDL Guide
Learning Objectives
- Quantify the burden of major communicable diseases in India and explain the primary care physician's strategic position
- Apply the epidemiological triad to explain determinants and modes of transmission
- Describe primary, secondary, and tertiary control measures including national programmes (NTEP, NVBDCP, NLEP, NACO) and essential PHC-level laboratory tests
- Explain IDSP surveillance structure, epidemic curves, and outbreak notification requirements
- Synthesise the primary care physician's role from case detection to referral and community education
INSTRUCTIONS
India still carries a substantial communicable disease burden — tuberculosis, malaria, dengue, leprosy, and HIV account for millions of disability-adjusted life years each year. As a primary care physician you will be the first point of contact for most of these cases. Understanding not just how to diagnose and treat but also how to interrupt transmission, notify authorities, and mobilise community action defines the difference between a clinician and a public health champion. This module builds both.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 5 (Communicable Diseases), Ch. 6 (National Health Programmes) (textbook)
- Mahajan & Gupta, Textbook of Preventive and Social Medicine, 4th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old agricultural worker presents to the PHC with three weeks of cough, low-grade fever, and 4 kg weight loss. His wife was treated for tuberculosis two years ago. The medical officer orders a sputum smear but realises she has not yet verified his immunization status, notified the suspected case to the district surveillance unit, or screened his two young children. She wonders: where does clinical care end and public health action begin — and can she manage both simultaneously at a busy PHC?
WHY THIS MATTERS
Communicable diseases account for roughly 30% of India's total disease burden despite decades of control programmes. The majority of patients — whether with tuberculosis, malaria, dengue, or acute diarrhoeal disease — make first contact at a primary health centre, not a tertiary hospital. This means you, as the PHC physician, hold the pivotal position in the epidemiological chain: you can diagnose early enough to prevent community spread, initiate treatment before complications arise, notify authorities to trigger a public health response, and educate families to break ongoing transmission. None of this requires a specialist — it requires you to think simultaneously as a clinician and a community epidemiologist.
RECALL
Before reading further, recall what you already know from Year 1 Community Medicine:
- The chain of infection — agent → source/reservoir → mode of transmission → portal of entry → susceptible host.
- Levels of prevention: primary (preventing disease before it occurs — immunisation, sanitation), secondary (early detection and prompt treatment), tertiary (limiting disability).
- Modes of transmission: direct contact, droplet, airborne, faeco-oral, vector-borne, parenteral, vertical.
- The epidemiological triad — agent, host, and environment, each contributing to disease occurrence.
This module builds directly on those foundations and applies them to specific national control programmes.
Disease Burden: Communicable Diseases in India
India's communicable disease burden remains among the highest globally, even as the country undergoes an epidemiological transition. Tuberculosis (TB) continues to be the single largest infectious killer: India contributes approximately 26% of the global TB incidence, with an estimated 2.8 million new cases per year (WHO Global TB Report 2023). Malaria causes approximately 2–5 million clinically confirmed cases annually in India, with Plasmodium falciparum responsible for the majority of severe disease and death; Odisha, Chhattisgarh, Jharkhand, and tribal areas of Maharashtra contribute a disproportionate share. Dengue has expanded dramatically over two decades — vector surveillance data show 200,000–300,000 confirmed cases annually (substantially under-reported), with urban areas and periurban settings particularly affected. Leprosy, though dramatically reduced from peak prevalence, still registers nearly 100,000 new cases per year, making India the country with the highest absolute new-case burden globally. HIV/AIDS is controlled but not eliminated — India's adult prevalence is approximately 0.2%, with concentrated epidemics in southern states and among key populations. Acute diarrhoeal diseases (ADD) and acute respiratory infections (ARI) remain leading causes of under-five morbidity and mortality, together responsible for approximately 20–25% of childhood deaths.
The critical epidemiological reality is that the PHC is the first and often only formal health contact for people in rural and semi-urban India. An ASHA worker refers a febrile child, a coughing farmer walks in, a woman with skin patches appears — all of these encounter the primary care system first. Early correct recognition at this level determines whether an individual case becomes a community outbreak.
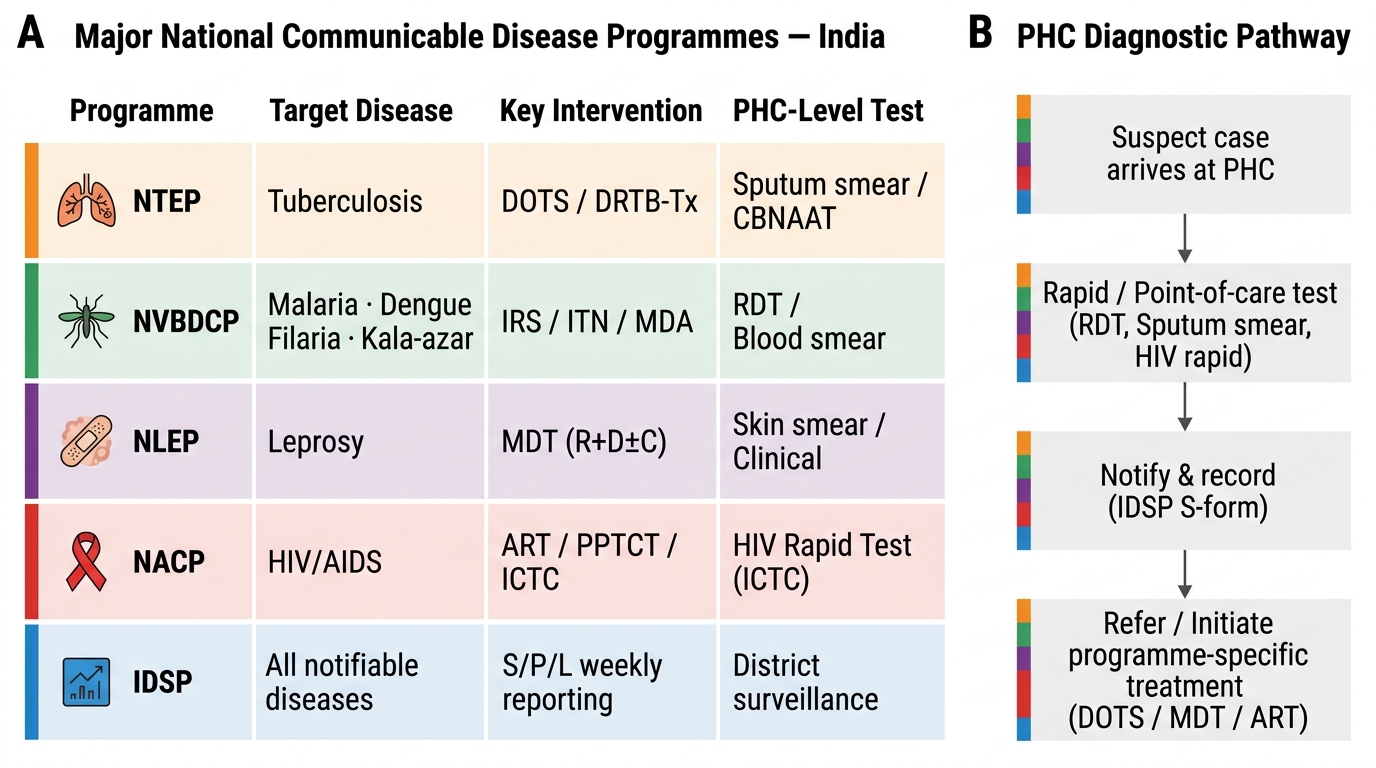
Major National Communicable Disease Control Programmes and PHC Diagnostic Pathway
SELF-CHECK
India contributes approximately what percentage of global tuberculosis incidence?
A. 10%
B. 26%
C. 40%
D. 51%
Reveal Answer
Answer: B. 26%
India contributes approximately 26% of global TB incidence according to the WHO Global TB Report 2023, making TB control through NTEP the nation's highest-priority communicable disease programme.
Determinants and Transmission at the Community Level
Every communicable disease episode arises from the interplay of three elements in the epidemiological triad: the agent (the pathogen — bacterium, virus, parasite, or fungus, with its virulence, infectivity, and pathogenicity), the host (the human or animal, with its age, immune status, nutritional state, genetic susceptibility), and the environment (physical, biological, and social — temperature, humidity, sanitation, crowding, vector habitats, healthcare access). Breaking any one link in this triad interrupts transmission; public health control strategies are essentially targeted attacks on one or more triad components.
For tuberculosis, the agent is Mycobacterium tuberculosis transmitted by airborne droplet nuclei (Wells droplet nuclei, <5 µm, remain suspended). Host factors — undernutrition (BMI <18.5 doubles risk), HIV co-infection (30× risk), diabetes mellitus, smoking — profoundly amplify susceptibility. Environmental determinants include overcrowded housing, poor ventilation, and delays in healthcare seeking. Control therefore attacks all three: DOTS treatment targets the agent (reduces infectious period from months to weeks), BCG vaccination and nutritional programmes target the host, and ventilation standards address the environment.
For vector-borne diseases (malaria, dengue, chikungunya, filariasis), the environment-agent-vector triad extends to include the arthropod vector. Anopheles mosquito breeding in stagnant water, Aedes aegypti in peridomestic water storage — these are fundamentally environmental determinants amenable to source reduction. Host susceptibility (prior immunity, sickle cell trait providing partial malaria protection) and agent characteristics (P. falciparum's drug resistance patterns) complete the picture.
For faeco-oral diseases (typhoid, hepatitis A, cholera, diarrhoeal diseases), the environment — specifically water supply safety, sewage disposal, food hygiene — dominates. The 5 F's transmission route (Faeces → Fingers → Flies → Food → Fluid → new host) is a practical teaching tool for community health education at the PHC level.
Social determinants — poverty, illiteracy, migration, gender inequality in healthcare seeking — cut across all communicable diseases and must be understood to design effective community-level interventions.
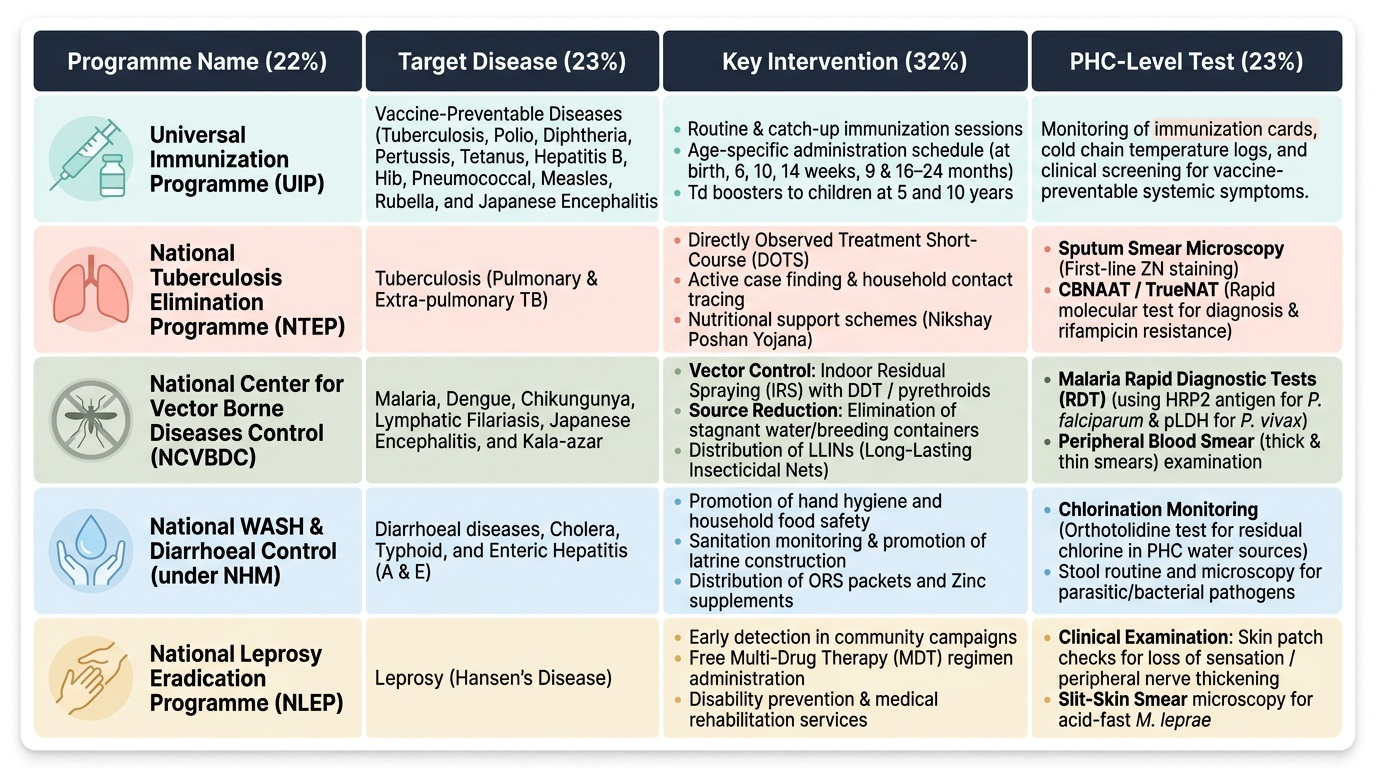
Control Measures and National Programmes
Provided image
Communicable disease control at the PHC level operates across three levels of prevention, implemented through specific programme mechanisms.
Primary prevention aims to prevent disease occurrence in susceptible individuals. At the PHC level this means: (1) Immunization — conducting routine and catch-up immunization sessions under the Universal Immunization Programme (UIP), which includes BCG (at birth), OPV (birth + 6, 10, 14 weeks + boosters), pentavalent (DTP + HepB + Hib at 6, 10, 14 weeks), PCV (6, 14 weeks, 9 months), IPV (14 weeks), MR (9 and 16–24 months), JE vaccine (in endemic areas), and Td boosters at 5 and 10 years. (2) Sanitation and safe water — promoting hand washing, safe drinking water (chlorination monitoring), latrine construction, and food hygiene. (3) Vector control — IRS (indoor residual spraying) with DDT or pyrethroid insecticides for malaria; source reduction for dengue (eliminating breeding containers).
Secondary prevention involves early detection and prompt treatment to reduce the infectious period and prevent complications. The essential PHC-level laboratory tests the physician must be able to use include:
- TB: sputum smear microscopy (ZN staining) as first-line; CBNAAT (Cartridge-Based Nucleic Acid Amplification Test) / TrueNAT for rapid molecular diagnosis and rifampicin resistance detection — now mandated for all suspected TB cases under NTEP
- Malaria: Rapid Diagnostic Tests (RDT) using HRP2 antigen for P. falciparum and pLDH for P. vivax; peripheral blood smear (Giemsa stain) for species confirmation and parasite density
- Leprosy: clinical diagnosis primarily (cardinal signs); slit-skin smear with ZN staining at PHC for bacteriological index in multibacillary cases
- Dengue: NS1 antigen test (high sensitivity in days 1–5 of fever); IgM ELISA after day 5
- Diarrhoeal diseases: stool microscopy (for parasites, RBCs), stool culture in outbreaks
Isolation of infectious cases (especially open pulmonary TB), contact tracing (examination and prophylaxis of TB contacts, identification of dengue breeding sites near index cases), and chemoprophylaxis (primaquine radical cure for P. vivax) complete secondary prevention.
National disease-specific programmes coordinated through the PHC include:
- NTEP (National Tuberculosis Elimination Programme) — renamed from RNTCP in 2020; implements DOTS, free diagnosis and treatment; NIKSHAY platform for case registration; target TB elimination by 2025 (< 1/million population incidence)
- NVBDCP (National Vector Borne Disease Control Programme) — integrates malaria, dengue, chikungunya, kala-azar, Japanese encephalitis, and lymphatic filariasis; annual blood survey for malaria; mass drug administration with DEC for filariasis
- NLEP (National Leprosy Eradication Programme) — MDT (multi-drug therapy): PB leprosy treated for 6 months (rifampicin monthly + dapsone daily), MB leprosy for 12 months (rifampicin monthly + clofazimine monthly + dapsone daily); contact examination; disability prevention
- NACO (National AIDS Control Organisation) — Integrated Counselling and Testing Centres (ICTC) for HIV testing; ART centres; prevention of parent-to-child transmission (PPTCT); targeted interventions for key populations
SELF-CHECK
A patient presents on day 3 of fever with severe myalgia and a petechial rash. Which PHC-level laboratory test is MOST appropriate as the initial screen for dengue?
A. IgM ELISA
B. NS1 antigen rapid test
C. Peripheral blood smear
D. Widal test
Reveal Answer
Answer: B. NS1 antigen rapid test
NS1 antigen tests have high sensitivity in the first 5 days of dengue infection (during the viraemic phase). IgM ELISA becomes positive only from day 5 onward. NS1 is the correct first-line test at the PHC when a patient presents in the first week of illness.