Page 4 of 20
CM8.2 | CM8.2 | Non-Communicable Disease Control at Primary Care — SDL Guide
Learning Objectives
- Quantify the burden of diabetes, hypertension, stroke, obesity, and cancer in India and explain premature mortality as the policy driver
- Identify the four major modifiable NCD risk factors and explain how social and environmental determinants amplify risk
- Describe NPCDCS programme structure, PHC-level screening tests, diagnostic thresholds, and treatment initiation
- Explain NCD programme monitoring through the cascade of care concept and key performance indicators
- Apply PHC physician responsibilities in opportunistic screening, lifestyle counselling, pharmacological management, and referral
INSTRUCTIONS
Non-communicable diseases now account for more than 60% of all deaths in India — and the majority of these are premature deaths in productive middle age. Most people with hypertension, diabetes, or early cancer in rural India have never been screened, let alone treated. The primary care physician, working within the NPCDCS framework, has the unique opportunity to find these cases early, prevent complications, and reduce the catastrophic household costs that NCDs impose. This module shows you how.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 12 (Non-Communicable Diseases) (textbook)
- Operational Guidelines for Prevention, Screening and Control of Common NCDs — MoHFW India, 2023 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old woman attends the PHC for a minor wound dressing. While waiting, she mentions she feels 'tired all the time' and has had blurring of vision for months. Her random blood sugar done on impulse is 312 mg/dL. She has never had her blood pressure checked. Her BMI is 28. She smokes beedis and has not seen a doctor in four years. This single opportunistic encounter, if used well, could prevent a stroke, renal failure, or blindness. Will the PHC physician use it?
WHY THIS MATTERS
India is in the midst of an NCD epidemic that threatens to overwhelm its health system. Non-communicable diseases — led by cardiovascular disease, diabetes, cancer, and chronic respiratory disease — now cause over 63% of all deaths nationally. The WHO estimates that India loses approximately 10 million productive life years annually to NCDs, imposing catastrophic financial burden on households. Crucially, 80% of premature NCD deaths are preventable with known, affordable interventions available at the primary care level. The PHC physician — detecting undiagnosed hypertension with a blood pressure cuff, initiating metformin for a newly diagnosed diabetic, performing VIA screening for cervical cancer — is the most cost-effective actor in India's NCD response.
RECALL
From your earlier studies, recall:
- Levels of prevention: primary (stopping disease before it starts — immunisation, tobacco cessation), secondary (early detection and treatment — screening), tertiary (preventing complications and disability).
- Epidemiological transition: shift from predominantly communicable to non-communicable disease burden as countries develop — India is mid-transition, facing a double burden.
- Risk factor: any attribute that increases the probability of disease occurrence in the individual or population.
- Screening: application of a test to detect a disease or pre-disease condition in asymptomatic individuals in a defined population.
This module applies all four concepts to the specific challenge of NCD control at primary care.
India's NCD Burden: Scale and Premature Mortality
India's non-communicable disease burden has reached epidemic proportions, and its most alarming feature is the youth of its victims. Unlike high-income countries where NCDs predominantly kill the elderly, India's NCD mortality peak falls in the 40–69 year age group — the most economically productive segment of the population. The WHO's Global Burden of Disease data shows that NCDs account for approximately 63% of all deaths in India, with cardiovascular diseases alone responsible for 28%, cancers for 9%, and diabetes and chronic respiratory disease each contributing significantly.
Diabetes mellitus affects approximately 77 million adults in India (IDF 2021), making India the world's second-largest diabetic population after China. More alarming is the reservoir of undiagnosed diabetes — surveys suggest nearly 50% of those with diabetes in India are undetected, creating a hidden epidemic of macro- and microvascular complications.
Hypertension is even more prevalent: national surveys (NFHS-5, 2019–21) show approximately 35% of adults aged 15 and above meet diagnostic criteria for hypertension. The control rate — those with measured hypertension achieving BP <140/90 mmHg — remains below 15% nationally, reflecting a profound treatment gap.
Stroke is the leading cause of disability in India; its incidence is rising in younger adults (40–59 years) due to uncontrolled hypertension and diabetes. Obesity (BMI ≥25 for Asians) now affects approximately 22–25% of adult women and 18–20% of adult men nationally (NFHS-5), with the highest prevalence in urban areas and among higher socioeconomic groups — though rural prevalence is catching up rapidly.
Cancer contributes approximately 806,000 deaths annually in India. The three most common cancers accounting for a large proportion of PHC-relevant burden are: oral (tobacco-related, highest in males), cervical (HPV-related, second most common cancer in Indian women), and breast cancer.
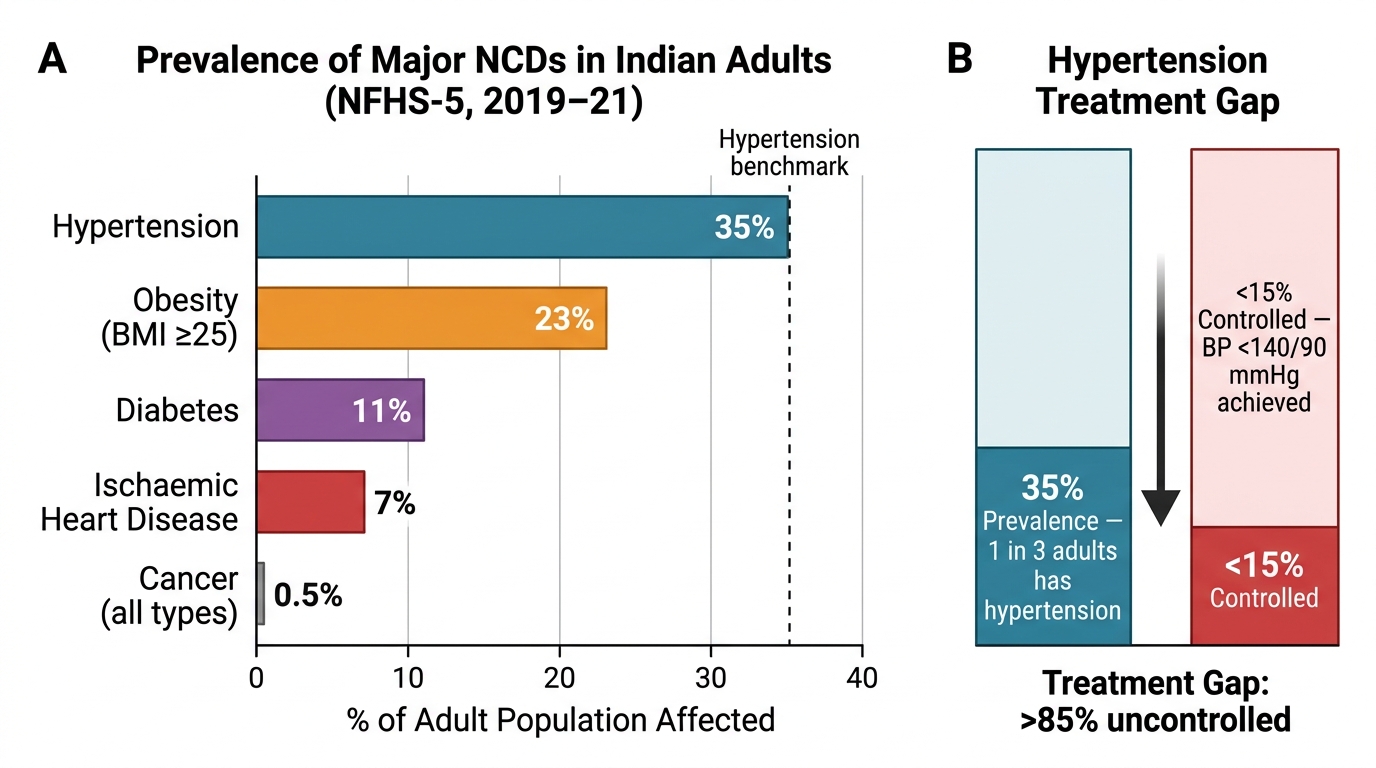
NCD Burden in India: Prevalence and the Hypertension Treatment Gap (NFHS-5, 2019–21)
SELF-CHECK
According to NFHS-5 (2019-21), approximately what percentage of adults in India meet diagnostic criteria for hypertension?
A. 8%
B. 20%
C. 35%
D. 55%
Reveal Answer
Answer: C. 35%
NFHS-5 data indicates approximately 35% of adults aged 15 and above in India have hypertension. Despite this high prevalence, the blood pressure control rate (achieving BP <140/90 mmHg among those with hypertension) remains below 15%, representing a major treatment gap that PHC physicians can address.
Determinants of NCDs: Modifiable Risk Factors and Social Context
The WHO identifies four major modifiable behavioural risk factors that collectively account for the vast majority of NCD burden globally and in India: (1) tobacco use (smoking, smokeless tobacco, beedis) — the single largest preventable cause of cancer and cardiovascular disease; (2) unhealthy diet (excess salt, saturated fat, refined carbohydrates, low fruit and vegetable intake); (3) physical inactivity — urbanisation and mechanisation have dramatically reduced daily energy expenditure even in populations that were formerly agricultural; and (4) harmful use of alcohol — a risk factor for hypertension, liver disease, and several cancers.
These four behavioural risk factors act through intermediate or metabolic risk factors: raised blood glucose, raised blood pressure, raised lipids (LDL cholesterol, triglycerides), and overweight/obesity. This is the conceptual basis of the common risk factor approach — one intervention (e.g. tobacco cessation counselling) simultaneously reduces risk of cardiovascular disease, several cancers, stroke, and COPD. This principle makes PHC-based NCD prevention cost-effective: you are not running separate programmes for each disease.
Social and environmental determinants amplify these risks in powerful ways. Urbanisation shifts food environments toward processed and energy-dense foods while reducing opportunities for physical activity. Poverty paradoxically increases NCD risk in India through: (a) food insecurity leading to calorie-dense but micronutrient-poor diets; (b) high tobacco and alcohol consumption as stress-coping mechanisms; (c) reduced access to preventive care and health literacy; (d) exposure to indoor air pollution (biomass fuel). Epigenetic programming from early nutritional deprivation — the developmental origins of health and disease (DOHaD) hypothesis — makes South Asian populations disproportionately prone to insulin resistance and abdominal obesity at lower BMI values than European populations, explaining why Asian cut-offs (BMI ≥25 for overweight, ≥30 for obesity; waist circumference >90 cm in men, >80 cm in women) differ from standard WHO thresholds.
Non-modifiable risk factors — age, sex (men at higher CVD risk at younger age; postmenopausal women's risk equalises), family history, and ethnicity — cannot be changed but are important for risk stratification that guides management intensity.
NPCDCS and PHC-Level Interventions: Screening, Diagnostics, and Treatment
The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) is India's umbrella NCD programme, launched in 2010 and now operating in all districts. Its PHC-level mandate includes:
- Population-based opportunistic screening of all persons aged ≥30 years attending PHC for any reason — for hypertension, diabetes, and three cancers (oral, breast, cervical)
- Treatment initiation for screen-positive/diagnosed cases within the primary care setting
- Referral pathways to District NCD Clinics and Cardiac Care Units (CCU) for complications or treatment-refractory cases
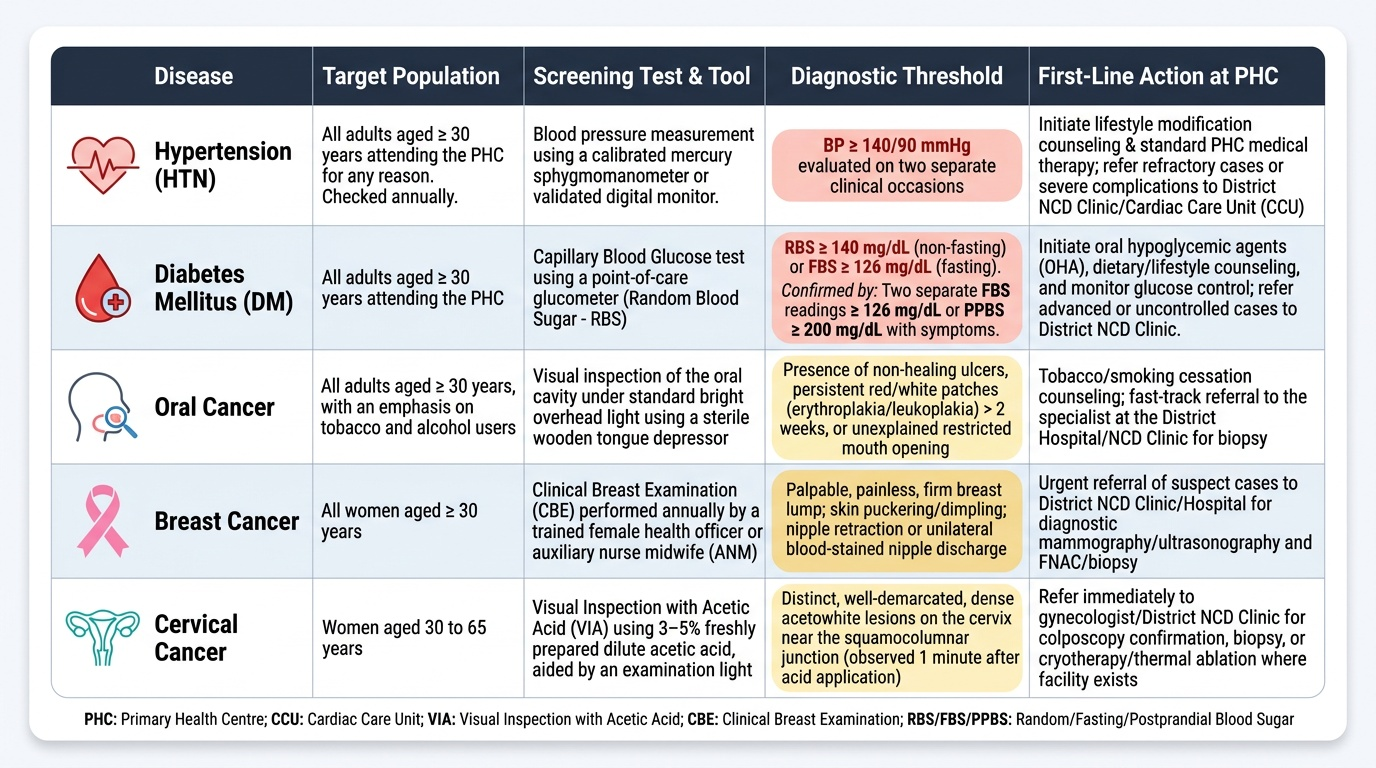
Essential PHC-level tests and their thresholds:
- Hypertension: Blood pressure measurement with calibrated mercury sphygmomanometer or validated digital device. Diagnostic threshold: BP ≥140/90 mmHg on two separate occasions. All adults ≥30 years should have BP checked annually.
- Diabetes: Random blood sugar (RBS) by glucometer as initial screen; if RBS ≥140 mg/dL (non-fasting) or ≥126 mg/dL (fasting), proceed to confirmation. Diagnostic thresholds: fasting blood sugar (FBS) ≥126 mg/dL on two occasions, or postprandial blood sugar (PPBS) ≥200 mg/dL with symptoms, or HbA1c ≥6.5% (laboratory test — PHC with lab access). Symptomatic patient with RBS ≥200 mg/dL can be diagnosed on a single test.
- Cervical cancer: VIA (Visual Inspection with Acetic Acid) — application of 3–5% acetic acid to cervix; acetowhite plaques indicate high-grade dysplasia or cancer. Women aged 30–65 years screened every 5 years. VIA is PHC-feasible (no colposcope or microscopy needed); Pap smear requires laboratory. VILI (Visual Inspection with Lugol's Iodine) is an alternative.
- Oral cancer: Visual inspection of oral cavity — lips, tongue, buccal mucosa, floor of mouth, palate, oropharynx — for suspicious lesions (leukoplakia, erythroplakia, non-healing ulcer >2 weeks). PHC-feasible with a torch and gloves. Tobacco/betel nut users and older men are the high-risk group.
- Breast cancer: Clinical breast examination (CBE) at PHC; teach self-breast examination (SBE) to all women 30+; mammography only available at secondary/tertiary centres.
Treatment at PHC level:
- Hypertension: first-line antihypertensives (amlodipine, atenolol, or thiazides per NPCDCS protocol) initiated by PHC physician
- Diabetes: metformin (if no contraindication) ± sulfonylurea; insulin initiation for newly detected Type 1 or severe hyperglycaemia
- Lifestyle counselling: SNAP approach — Salt restriction, No tobacco, Activity (150 min/week moderate exercise), Prudent diet — for all NCD patients
Provided image
SELF-CHECK
A 45-year-old woman presents to the PHC for routine follow-up. Under NPCDCS, which cervical cancer screening test should be offered at the PHC level?
A. Pap smear
B. HPV DNA test
C. VIA (Visual Inspection with Acetic Acid)
D. Colposcopy
Reveal Answer
Answer: C. VIA (Visual Inspection with Acetic Acid)
VIA (Visual Inspection with Acetic Acid) is the PHC-feasible screening test for cervical cancer under NPCDCS. It requires only acetic acid solution, a good light source, and a trained provider — no laboratory or colposcope needed. Pap smear requires cytology laboratory capability. Women aged 30–65 should be screened every 5 years.