Page 1 of 19
CM3.1 | CM3.1 | Environmental Pollution Hazards — SDL Guide
Learning Objectives
- Classify the major categories of environmental pollutants (air, water, noise, radiation) and their sources
- Describe the health hazards of each pollutant type, linking mechanism to organ-system effect
- Recall India's National Ambient Air Quality Standards (NAAQS) and WHO guideline values for key pollutants
- Identify patients at risk from environmental exposures and describe how to take an occupational/environmental history
INSTRUCTIONS
Environmental pollution is the single largest environmental health risk globally, responsible for an estimated 9 million premature deaths per year. As a frontline clinician in India—where ambient air quality regularly exceeds safe limits in major cities and millions rely on contaminated water sources—you will routinely encounter pollution-attributable illness. This module builds your ability to recognise, explain, and act on environmental hazards affecting your patients.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., K Park, Ch 11 (Environmental Health) (textbook)
- WHO Global Air Quality Guidelines 2021 (guideline)
- India National Ambient Air Quality Standards (NAAQS), CPCB 2009 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old retired welder from Kanpur presents with progressive breathlessness, a persistent productive cough, and chest tightness that is worse on days when the city's air quality index (AQI) reads 'hazardous'. He also reports mild hearing difficulty and is mildly anaemic. His wife mentions that the household uses a kerosene stove for cooking. As you review his spirometry—showing a mixed obstructive-restrictive pattern—you realise that at least three distinct environmental exposures may be converging on this one patient: occupational metal fumes, indoor air pollution, and community-level ambient air pollution. Understanding the sources, mechanisms, and health consequences of each pollutant type is not optional knowledge for an Indian clinician—it is a core clinical competency.
WHY THIS MATTERS
India bears one of the world's highest pollution-attributable disease burdens. In 2019, air pollution alone contributed to 1.67 million deaths in India (State of Global Air 2020). Waterborne diseases from polluted sources cause tens of thousands of deaths annually, disproportionately affecting children under five. Noise-induced hearing loss affects an estimated 16% of disabling adult hearing loss globally. As physicians, you will be required by the NMC to counsel patients on environmental risks, report occupationally or environmentally linked disease, and contribute to public health surveillance—none of which is possible without knowing the specific hazards, their thresholds, and their clinical signatures.
RECALL
Before proceeding, activate your Year-1 physiology knowledge. Recall: (a) how gas exchange occurs across the alveolar membrane and which particle sizes penetrate to the alveoli; (b) haemoglobin's oxygen dissociation curve and how competitive binding by a foreign gas shifts it left; (c) the nephron's role in eliminating or accumulating heavy metals; and (d) the fundamentals of radiation biology—ionising radiation transfers energy to biological tissue, causing direct strand breaks and indirect free-radical damage. These mechanisms underpin every hazard discussed in this module.
The Burden of Environmental Pollution on Human Health
Environmental pollution is defined as the introduction of contaminants into the natural environment at concentrations that cause adverse effects on living organisms. Globally, pollution of all types was responsible for approximately 9 million premature deaths in 2019—16% of all deaths—making it the largest environmental cause of disease and premature death. In India, the picture is even more stark: the country accounts for roughly 18% of the global pollution-attributable mortality, driven by a unique combination of rapid industrialisation, high population density, widespread biomass burning, and inadequate sanitation infrastructure.
The health impact is not uniform across organ systems or populations. Children, the elderly, and those with pre-existing cardiorespiratory or renal disease face disproportionate risk. The mechanisms are diverse: some pollutants (particulate matter, asbestos) cause local respiratory inflammation; others (lead, mercury, arsenic) are systemic toxins accumulating in target organs over years of low-level exposure; and radiation can alter DNA in ways that manifest as cancer decades later.
Four major categories of environmental hazards are covered in this SDL:
- Air pollutants (gaseous and particulate)
- Water pollutants (biological, chemical, radiological)
- Noise (occupational and community)
- Radiation (ionising and non-ionising)
Each category has a distinct epidemiological profile, a set of regulatory standards, and characteristic health effects that you must be able to describe and apply clinically.
Air Pollution: Sources, Pollutants, and Health Hazards
Air pollutants are classified into primary pollutants (emitted directly from a source, e.g. CO, SO2, PM from combustion) and secondary pollutants (formed by atmospheric reactions, e.g. ground-level ozone formed when NOx reacts with volatile organic compounds in sunlight). They are further grouped by physical form: gaseous pollutants and particulate matter (PM). PM is sub-classified by aerodynamic diameter: PM10 (≤10 µm, inhalable—deposited in upper airways) and PM2.5 (≤2.5 µm, fine particulate—penetrates to alveoli and crosses into the bloodstream, driving systemic cardiovascular effects). Ultrafine PM1 can even cross the blood-brain barrier.
The major air pollutants and their health effects are summarised in the figure below.
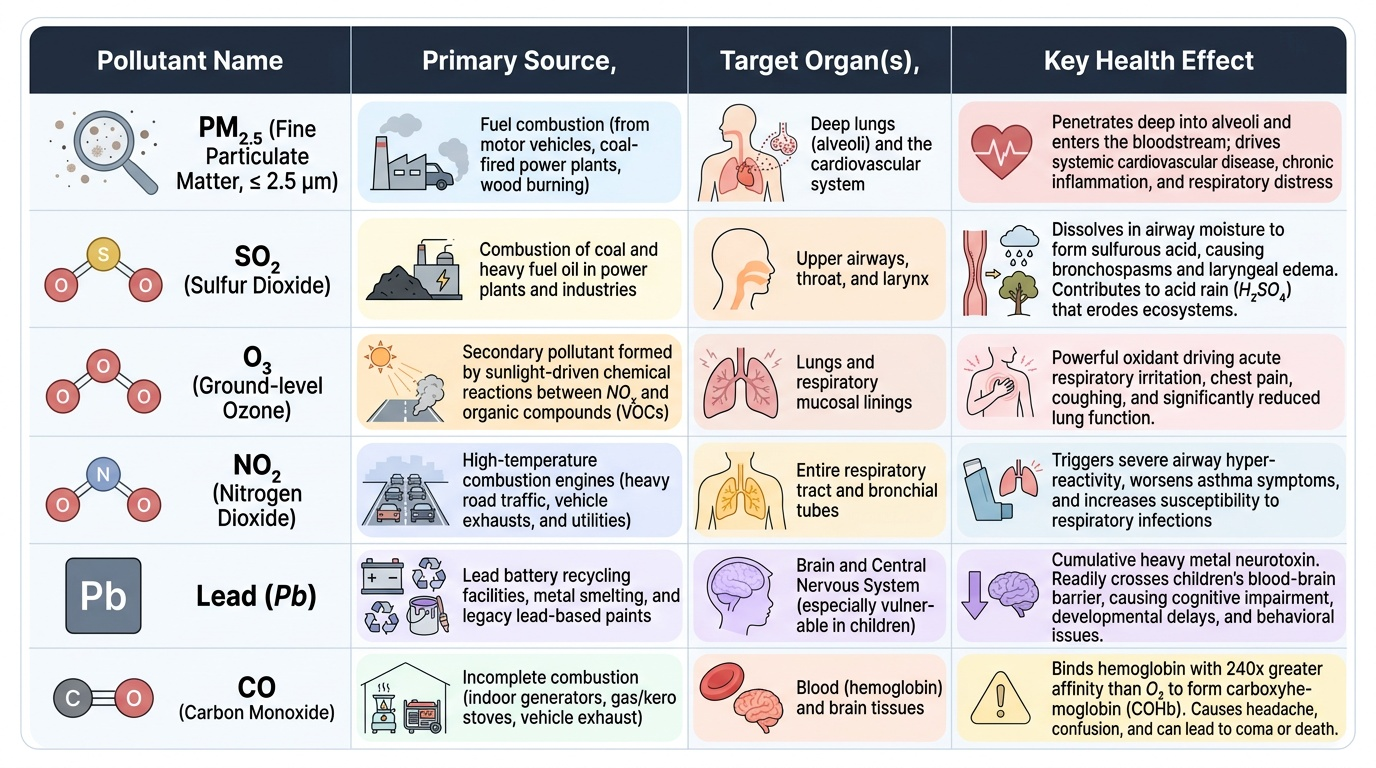
Provided image
Carbon monoxide (CO) deserves special emphasis because it is colourless, odourless, and deadly at concentrations that give no warning. CO binds haemoglobin at the same site as oxygen but with approximately 240 times greater affinity, forming carboxyhaemoglobin (COHb), which cannot carry oxygen. At COHb 10-20%, patients experience headache and confusion; at >60%, coma and death. Indoor sources (kerosene stoves, charcoal burners, generators) are responsible for most fatal CO poisonings in Indian households. Treatment is high-flow 100% oxygen, which competes with CO and accelerates COHb dissociation.
Sulfur dioxide (SO2) is generated by burning coal and heavy fuel oil. It is highly water-soluble: at high concentrations it dissolves in upper-airway moisture to form sulfurous acid, causing bronchospasm and laryngeal oedema. At lower concentrations it contributes to acid rain (when oxidised in the atmosphere to H2SO4), damaging ecosystems and eroding stone monuments.
Lead was once a major air pollutant from petrol (leaded petrol was phased out in India by 2000). Today, occupational exposure (battery recycling, smelting, paint manufacturing) remains significant. Lead is a cumulative heavy metal neurotoxin: children are especially vulnerable because their blood-brain barriers are more permeable and they absorb 50% of ingested lead vs 10% in adults. Blood lead levels ≥5 µg/dL require public health action (CDC 2021 reference value). Lead interferes with haem synthesis (causing anaemia), impairs calcium-dependent neurotransmitter release, and damages proximal renal tubules.
Noise and Radiation Hazards
Noise pollution is measured in decibels (dB) on a logarithmic scale. The ear tolerates brief high-intensity sounds but suffers cumulative damage with sustained high exposures. Noise-induced hearing loss (NIHL) is the most prevalent occupational disease globally: exposure to ≥85 dB(A) for 8 hours/day over years destroys cochlear hair cells irreversibly. India's Central Pollution Control Board (CPCB) sets occupational noise limits at 85 dB(A) for an 8-hour time-weighted average. Community noise standards under the Environment (Protection) Amendment Rules 2000 set daytime limits of 75 dB for industrial zones, 65 dB for commercial, 55 dB for residential areas, and 50 dB for silence zones.
Beyond hearing loss, noise causes non-auditory effects: sustained exposure to community noise >55 dB at night (WHO guidance) disrupts sleep, raises sympathetic tone, and is associated with elevated cortisol, hypertension, and increased cardiovascular event risk.
Radiation is divided into two categories with very different health profiles. Ionising radiation (X-rays, gamma rays, alpha and beta particles, neutrons) carries sufficient energy to eject electrons from atoms, generating free radicals that cause double-stranded DNA breaks. Effects are: (a) deterministic—occur above a threshold dose, severity increases with dose (e.g. radiation sickness at >1 Gy acute, cataract at >0.5 Gy); (b) stochastic—probabilistic, no threshold, severity independent of dose (e.g. radiation-induced cancer, heritable mutations). Occupational exposures from radiology, nuclear medicine, and industrial radiography are regulated under the Atomic Energy (Radiation Protection) Rules 2004 (effective dose limit: 20 mSv/year for radiation workers).
Non-ionising radiation (UV, infrared, microwave, radiofrequency) lacks sufficient photon energy to ionise atoms but causes biological effects through heating and photochemical reactions. UV-B radiation (280-315 nm) causes skin erythema, premature ageing, and is the primary aetiological agent in cutaneous squamous cell carcinoma and basal cell carcinoma, as well as cataracts. Stratospheric ozone depletion by chlorofluorocarbons (CFCs) increases UV-B reaching the earth's surface.