Page 5 of 19
CM3.2-3 | CM3.2-3 | Safe Water and Waterborne Disease — SDL Guide
Learning Objectives
- Define 'safe' and 'wholesome' water and classify sanitary sources of water
- Describe the steps of conventional municipal water purification and the principles of household water treatment
- Recall BIS IS 10500:2012 standards for physical, chemical, and bacteriological quality of drinking water
- Classify waterborne diseases by pathogen type and describe the aetiology and pathogenic basis of cholera, typhoid, hepatitis A, hepatitis E, amoebiasis, and guinea worm disease
- Describe the concepts of water conservation and rainwater harvesting
INSTRUCTIONS
Access to safe water is one of the most powerful determinants of child survival and community health. In India, despite major improvements under the Jal Jeevan Mission, millions still depend on unprotected sources, and waterborne disease outbreaks continue to claim lives—many of them preventable. This module gives you the conceptual and factual foundation to assess water safety, understand how waterborne pathogens cause disease, and respond appropriately as a clinician and public health practitioner.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., K Park, Ch 12 (Water and Health) (textbook)
- BIS IS 10500:2012 — Indian Standard Drinking Water Specification (standard)
- WHO Guidelines for Drinking-water Quality, 4th ed. 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During the monsoon season, a district hospital in rural Rajasthan admits 47 patients over five days with acute watery diarrhoea, severe dehydration, and rice-water stools. The district CMO traces the outbreak to a single overhead tank that serves a slum colony—after heavy rains, sewage seeped into the tank through a cracked inlet pipe. Stool culture confirms Vibrio cholerae O1 El Tor. Meanwhile, three pregnant women in the same cluster are admitted with jaundice and acute liver failure—rapid serology confirms hepatitis E. Two water-related pathogens, one contaminated source, two very different diseases with very different severity profiles. Understanding how water becomes unsafe, what organisms it can carry, and how those organisms cause illness is the foundation of every outbreak investigation and water safety decision you will ever make.
WHY THIS MATTERS
Waterborne diseases kill approximately 485,000 people per year globally from diarrhoea alone (WHO 2019). In India, the burden is enormous: diarrhoeal diseases remain a leading cause of death in children under five, and viral hepatitis A and E cause epidemic jaundice across states with inadequate water infrastructure. The Government of India's Jal Jeevan Mission (2019) aims to provide piped water supply to every rural household by 2024—a programme that will save hundreds of thousands of lives if sustained. As a physician, you are the last clinical safety net when the water system fails. You must know what makes water safe, how to investigate outbreaks, and when to initiate public health action.
RECALL
Activate your Year-1 knowledge before proceeding. Recall: (a) the gastrointestinal absorptive and secretory physiology—specifically cAMP-mediated chloride secretion in enterocytes, which is hijacked by cholera toxin; (b) immune response to viral hepatitis—how hepatocellular inflammation raises transaminases and impairs bilirubin conjugation; (c) the concept of faecal-oral transmission from microbiology—why the infective dose matters (100 Vibrio cholerae vs 10–100 Salmonella typhi for typhoid); and (d) basic concepts of filtration and disinfection from chemistry.
The Burden of Waterborne Disease: Why Safe Water Matters
Waterborne diseases are illnesses caused by the ingestion of water contaminated with pathogenic microorganisms or toxic chemicals. The global burden is staggering: unsafe water, sanitation, and hygiene (WASH) together account for approximately 1.4 million preventable deaths per year (WHO 2019), with diarrhoeal diseases making up the largest share. Globally, 2 billion people lack access to safely managed drinking water services.
In India, the picture reflects both the scale of the problem and the ongoing transformation through national programmes. The Jal Jeevan Mission, launched in 2019, aims to provide functional household tap connections to all 192 million rural households by 2024, targeting a shift from unprotected well and surface water to treated piped supply. Yet urban slums, peri-urban settlements, and flood-prone districts remain highly vulnerable. During the 2019 cholera outbreak in Hyderabad and the annual monsoon-season hepatitis E epidemics in northern India, contaminated water was the confirmed vehicle.
The disease burden is not just from acute gastroenteritis. Chronic exposure to chemically contaminated water—arsenic in Bengal, fluoride in Rajasthan, nitrates in agricultural districts—produces insidious long-term harm that presents in outpatient clinics years after initial exposure. A physician practicing in India must understand the full spectrum of water-related hazards, from the acute cholera cluster to the chronic fluorosis patient.
Concepts of Safe and Wholesome Water: Sources and Standards
Safe water is defined as water that does not contain any pathogen at concentrations capable of causing disease. Wholesome water is a broader concept: it is water that is safe, palatable (acceptable colour, taste, and odour), and free from chemical constituents likely to cause harm on long-term consumption. Park's Textbook defines the attributes of wholesome water as: (1) free from pathogenic organisms; (2) free from harmful chemical substances; (3) pleasant to taste, odourless, colourless; (4) cool; and (5) free from suspended impurities.
Sanitary sources are classified from most to least protected:
1. Piped treated water supply (most protected): treated municipal supply delivered under pressure; risk of contamination mainly at the consumer end if pipes are old or cross-connected with sewage lines.
2. Protected dug wells and boreholes: sealed, covered, with a sanitary apron and hand pump; no open top through which surface run-off can enter.
3. Rainwater collected from clean rooftops into sealed cisterns.
4. Unprotected dug wells: open-topped, susceptible to faecal contamination.
5. Surface water (rivers, ponds, canals): highest risk; almost always requires treatment.
Quality standards for drinking water in India are set by BIS IS 10500:2012, which specifies acceptable limits (the standard to aim for) and permissible limits (the maximum allowed in the absence of an alternative source) across three domains:
- Physical: turbidity ≤1 NTU (acceptable), ≤5 NTU (permissible); colour ≤5 Hazen units (acceptable); no objectionable taste or odour; temperature ideally ≤25°C.
- Chemical: pH 6.5–8.5; total dissolved solids (TDS) ≤500 mg/L (acceptable), ≤2000 mg/L (permissible); key ions and chemicals each with specified limits (fluoride 1.0/1.5 mg/L, arsenic 10/50 µg/L, nitrate 45 mg/L).
- Bacteriological: the gold standard is zero E. coli per 100 mL in treated piped water; coliform count must be nil per 100 mL in any treated water supply. A residual free chlorine of ≥0.2 mg/L at the consumer tap is required as evidence of effective disinfection.
SELF-CHECK
A routine water sample from a municipal tap is tested. The results show: turbidity 3 NTU, residual chlorine 0.15 mg/L, E. coli: nil per 100 mL, TDS: 450 mg/L. Which finding represents a non-conformance with BIS IS 10500:2012 and what is the public health concern?
A. TDS 450 mg/L — exceeds the BIS acceptable limit of 300 mg/L
B. Turbidity 3 NTU — exceeds the BIS acceptable limit of 1 NTU but is within the permissible limit of 5 NTU; no public health concern
C. Residual chlorine 0.15 mg/L — below the BIS minimum of 0.2 mg/L at tap; this indicates inadequate disinfection, even though current bacteriological quality appears acceptable
D. E. coli nil per 100 mL — this should be positive for the water to be considered 'wholesome'
Reveal Answer
Answer: C. Residual chlorine 0.15 mg/L — below the BIS minimum of 0.2 mg/L at tap; this indicates inadequate disinfection, even though current bacteriological quality appears acceptable
The residual chlorine of 0.15 mg/L is below the BIS minimum of 0.2 mg/L required at the consumer end. Although the current bacteriological sample shows zero E. coli, residual chlorine serves as a buffer against post-treatment contamination (e.g. from pipe cross-connections, intermittent supply). Its absence means the water offers no protection against contamination occurring between the treatment plant and the consumer's tap—a critical safety margin in a system with intermittent supply and ageing pipes. TDS of 450 mg/L is within the acceptable limit (500 mg/L). Turbidity 3 NTU is above the acceptable limit (1 NTU) but within the permissible limit (5 NTU)—it should be flagged but does not represent a bacteriological hazard by itself.
Water Purification Processes
Conventional municipal water treatment follows a sequence of physical and chemical steps, each targeting a different category of impurity. The treatment sequence and its logic are shown in the figure below.
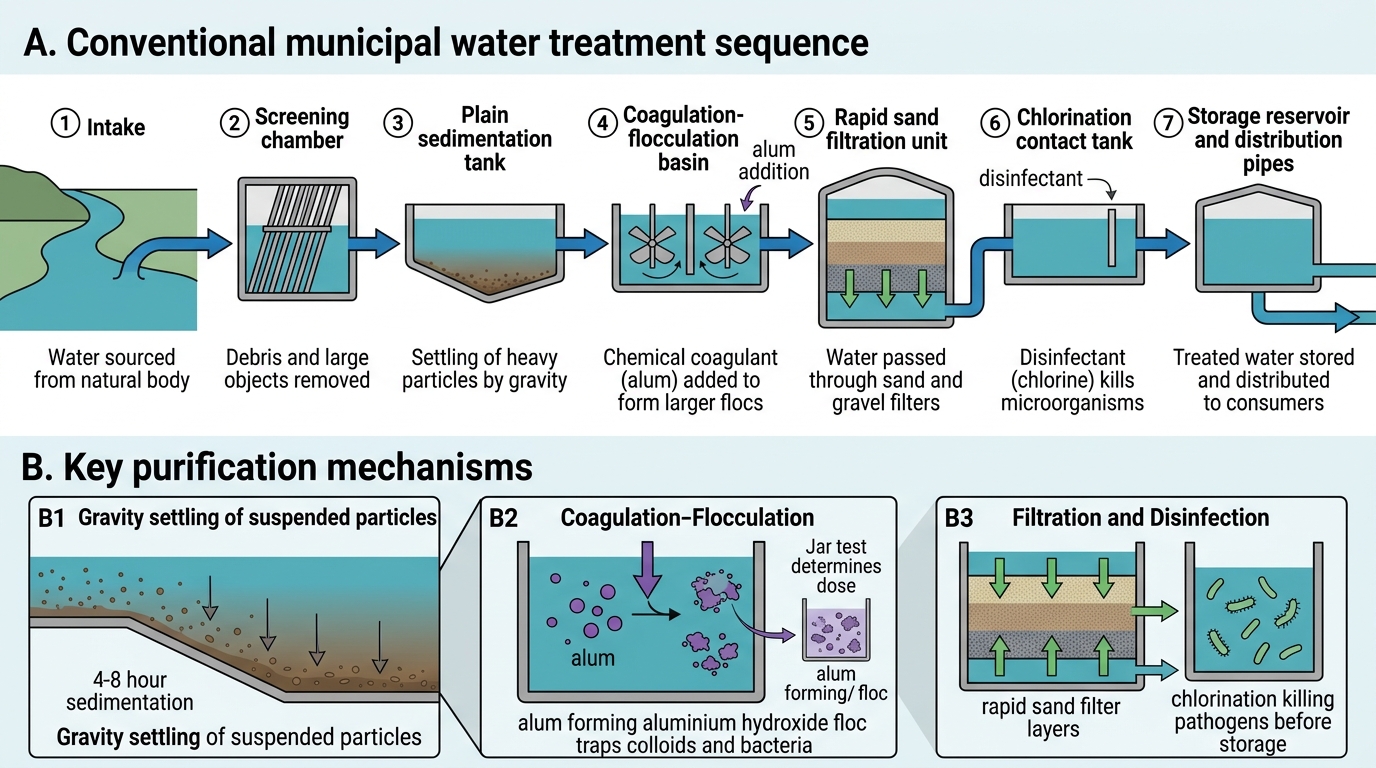
Conventional Municipal Water Treatment Sequence
Step 1 — Screening: coarse screens remove large debris (leaves, fish, garbage) at the intake.
Step 2 — Sedimentation (plain sedimentation): water rests in sedimentation tanks for 4–8 hours, allowing heavier suspended particles to settle by gravity. This reduces turbidity but does not remove fine colloidal particles or microorganisms effectively on its own.
Step 3 — Coagulation-flocculation: a coagulant—most commonly alum (aluminium sulfate)—is added. Alum reacts with bicarbonate in water to form aluminium hydroxide floc, a gelatinous precipitate that traps fine particles, colloids, and some bacteria. The mass then settles, greatly reducing turbidity and bacterial load. The optimal dose of alum is determined by a jar test.
Step 4 — Filtration: filtered through rapid sand filters (after coagulation) or slow sand filters (without prior coagulation). Slow sand filtration relies on a biological layer at the sand surface—the Schmutzdecke (German: 'dirty layer')—which is an active biofilm of bacteria and protozoa that degrade organic matter and remove pathogens with 99.99% efficiency; it is the most effective single-step water treatment for small communities. Rapid sand filtration is a physical process (smaller sand, faster flow) and requires pre-treatment with coagulation.
Step 5 — Disinfection (chlorination): the final and most critical step. Chlorine gas or calcium hypochlorite is added to achieve a contact time sufficient to kill residual bacteria and viruses. The key outcome measure is residual chlorine ≥0.2 mg/L at the consumer's tap—this is the WHO and BIS standard. Break-point chlorination is the technique of adding chlorine until all oxidisable material has been consumed and a stable residual is achieved.
Household water treatment options include boiling (most reliable—destroys all pathogens at 100°C), chemical disinfection (chlorine tablets, sodium hypochlorite solution), solar disinfection (SODIS—UV-A in sunlight inactivates pathogens in clear plastic bottles over 6 hours), and ceramic candle or activated carbon filters. Boiling is the standard recommendation for household use when supply reliability is in doubt.