Page 8 of 19
CM3.4-5 | CM3.4-5 | Environmental Sanitation and Housing — SDL Guide
Learning Objectives
- Describe the concept of solid waste, classify its types, and describe principles of safe disposal including biomedical waste management rules
- Describe the types of sanitary latrines and the stages of sewage treatment, with BOD as the key measure of effluent quality
- Describe housing standards (floor area, air space, ventilation, services) and the health effects of substandard housing
- Describe the Swachh Bharat Mission and its role in reducing open defecation
INSTRUCTIONS
Sanitation—the safe management of human excreta, solid waste, and sewage—and housing quality are fundamental determinants of health that interact with almost every disease a clinician will encounter. A doctor who does not know the minimum housing standards, cannot identify a family at risk from poor sanitation, or is unaware of their legal responsibilities under biomedical waste rules, is missing core competencies that the NMC considers essential. This module builds those competencies systematically.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., K Park, Ch 13 (Excreta Disposal) and Ch 14 (Solid Waste Management) and Ch 18 (Housing) (textbook)
- Bio-Medical Waste Management Rules 2016 (amended 2018, 2019), MoEFCC (legislation)
- Swachh Bharat Mission — Grameen Phase I & II, Ministry of Jal Shakti (programme)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy in a peri-urban settlement in Patna is admitted for the third time this year with acute diarrhoea and moderate dehydration. His home is a single room shared by 7 family members, with no piped water, no toilet (family practices open defecation in an adjacent field), and a kerosene stove that fills the room with smoke when cooking. The local angan wadi worker notes that three other children in the settlement have similar presentations this week. Meanwhile, at the district hospital, a nurse presents to occupational health with a needlestick injury from a bin-bag containing discarded syringes mixed with general domestic refuse—the hospital ward cleaner had placed them there without segregation. Two public health failures, two entirely preventable harms: absent sanitation infrastructure in the community and absent biomedical waste compliance in the hospital. Both are within your sphere of influence as a physician.
WHY THIS MATTERS
Poor sanitation contributes to approximately 500,000 diarrhoeal deaths in India annually, disproportionately affecting children under five. India has historically accounted for 60% of the global population practising open defecation—a statistic being reversed through the Swachh Bharat Mission. Overcrowded, poorly ventilated housing is a key driver of tuberculosis transmission, with India carrying 28% of the global TB burden. Unsafe biomedical waste disposal creates occupational hazard for healthcare workers and community contamination via sharps injuries and pathogen dispersal. Each of these represents a determinant of disease that you, as a clinician, can identify, quantify, and act on—both for individual patients and for the communities you serve.
RECALL
Recall from Year-1 microbiology: the faecal-oral transmission route—how enteric pathogens move from faeces to a new human host via contaminated soil, water, food, or hands. The central insight of sanitation science is that interrupting this chain at the excreta stage (by safely containing and treating human waste) prevents multiple downstream diseases simultaneously. Also recall from physiology: pulmonary mechanics and how reduced ventilation in a room increases CO2 and pathogen load in the air—relevant to understanding the health effects of overcrowding.
The Burden of Inadequate Sanitation and Poor Housing on Health
Environmental sanitation is defined as the control of all environmental factors that have a deleterious effect on physical, mental, or social wellbeing. In practice, it encompasses the safe management of human excreta, solid waste, and sewage, as well as the provision of adequate housing. The WHO estimates that inadequate WASH (water, sanitation, and hygiene) is responsible for approximately 1.4 million preventable deaths annually, with diarrhoeal diseases the leading cause.
In India, three specific burdens demand your attention as a clinician:
1. Open defecation: Before the Swachh Bharat Mission (SBM) Phase I, India was home to approximately 550 million people practising open defecation (OD)—the largest number in any country. OD contaminates soil, surface water, and food, creating a near-continuous faecal-oral transmission environment for enteric pathogens. SBM Phase I (2014–2019) built approximately 110 million household toilets and declared India Open Defecation Free (ODF) in October 2019, though sustained behaviour change and toilet use remain ongoing challenges.
2. Overcrowded and poorly ventilated housing: India's urban population density, especially in slums (65 million people, Census 2011), creates conditions for airborne pathogen transmission. Tuberculosis is the paradigm disease: the infectious dose for M. tuberculosis is extremely low, and crowded rooms with poor ventilation are ideal transmission environments. One meter of Mycobacterium tuberculosis-laden air inhaled can initiate infection.
3. Unsafe biomedical waste: Inadequate segregation and disposal of healthcare waste creates occupational risk (needlestick injuries) and environmental contamination, particularly in small clinics and primary care settings where compliance with Bio-Medical Waste Management Rules is often poor.
Solid Waste Management: Classification, Disposal, and Biomedical Waste
Solid waste is any discarded material in solid, semisolid, or liquid form (other than sewage or wastewater). Municipal solid waste (MSW) in India is generated at approximately 0.4–0.6 kg per person per day, totalling over 160,000 tonnes/day nationally. The principle of solid waste management is the 3R hierarchy: Reduce (prevent waste generation at source), Reuse (find new uses for discarded items), Recycle (recover materials for reprocessing). Only waste that cannot be reduced, reused, or recycled should go to final disposal.
Final disposal methods include: sanitary landfill (the standard method—engineered site with liner, leachate collection, and gas venting to prevent ground/water contamination); incineration (reduces volume by ~90%, required for specific hazardous/biomedical waste); composting (aerobic decomposition of organic waste to humus—safe for garden/agricultural use); and vermicomposting (using earthworms to accelerate decomposition).
Biomedical waste (BMW) is particularly hazardous and is regulated separately under the Bio-Medical Waste Management Rules 2016 (amended 2018, 2019), enforced by the State Pollution Control Boards. BMW is segregated at the point of generation into colour-coded categories:
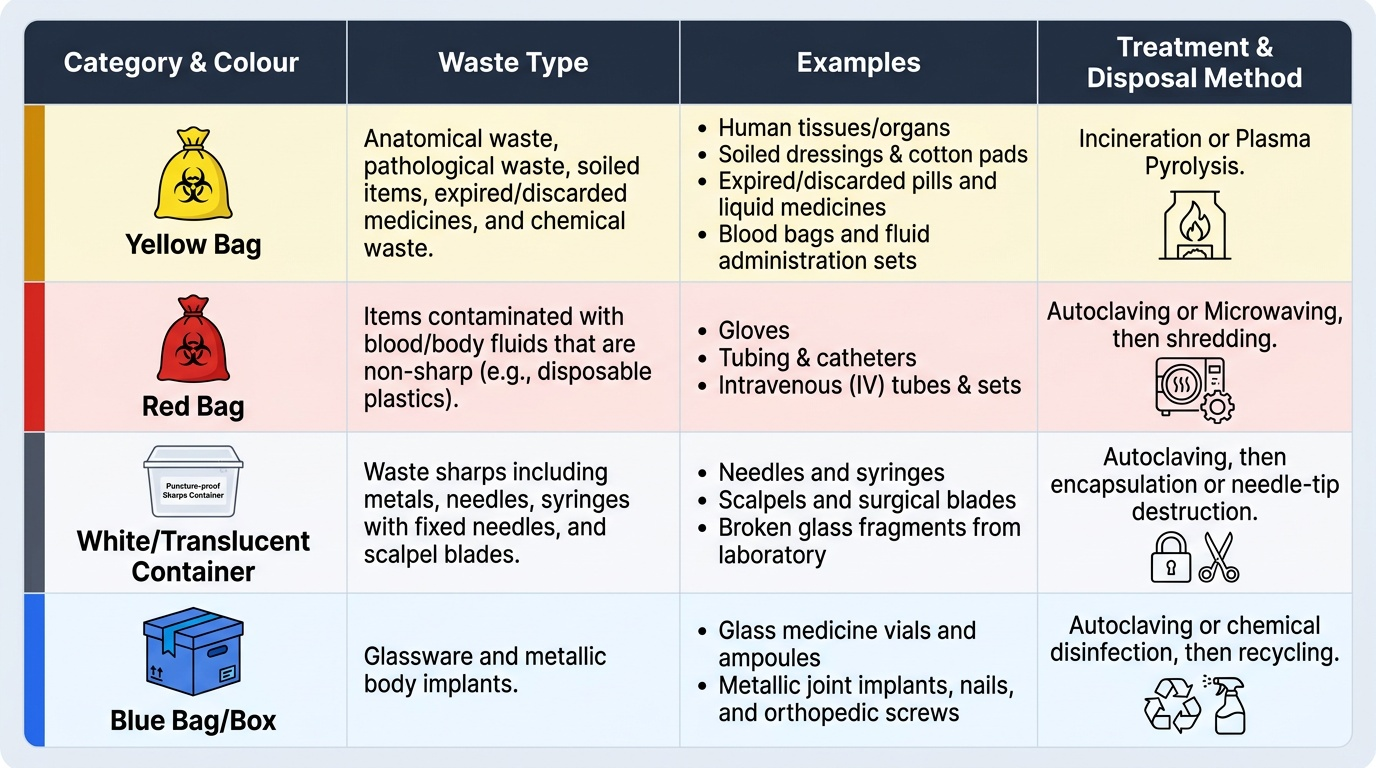
Provided image
The four categories are: Yellow bag—human anatomical waste, soiled dressings, expired medicines, blood bags (incineration or plasma pyrolysis); Red bag—items contaminated with blood/body fluids that are non-sharp (gloves, tubing, IV sets) (autoclave/microwaving then shredding); White/translucent puncture-proof container—sharps (needles, blades, broken glass from lab) (autoclaving then needle-tip cutters or encapsulation); Blue bag/box—glassware, metallic implants (autoclave/chemical disinfection then recycling).
As a doctor, you have a legal duty to ensure correct BMW segregation in your workplace. Mixing sharps with general waste (as in the hook scenario) violates Rule 4 of BMW Rules 2016 and creates occupational and community hazard.
SELF-CHECK
After performing a dressing change, a nurse has: (a) a soiled gauze pad soaked with wound exudate, (b) the used needle from a local anaesthetic injection, (c) an empty glass ampoule. In which bags do these items respectively belong under BMW Rules 2016?
A. All three go into the yellow bag for incineration
B. Soiled gauze → red bag; needle → white puncture-proof container (sharps); glass ampoule → blue box
C. Soiled gauze → yellow bag; needle → red bag; glass ampoule → white container
D. All sharps and bloodstained items go into a single red bag; glass goes in the dustbin
Reveal Answer
Answer: B. Soiled gauze → red bag; needle → white puncture-proof container (sharps); glass ampoule → blue box
Under BMW Management Rules 2016: (a) soiled dressings with blood/body fluids that are non-sharp go into the red bag for autoclave/microwave treatment; (b) sharps (needles, blades) go into the white/translucent puncture-proof container which is ultimately autoclaved and needle-tip-cut or encapsulated; (c) glassware goes into the blue box/bag for autoclave or chemical disinfection followed by recycling. Yellow bags are for anatomical waste, soiled items requiring incineration (e.g. blood bags, expired medicines), not for routine wound dressings. This distinction is frequently violated in practice and is a common exam topic.
Human Excreta and Sewage Disposal
Human excreta disposal is the cornerstone of environmental sanitation. The two major systems are: (a) on-site sanitation (the excreta does not leave the premises—pit latrines, septic tanks, composting toilets), and (b) off-site sanitation (the excreta is conveyed by a sewer network to a treatment facility). The public health priority in India is eliminating open defecation, currently addressed through the Swachh Bharat Mission's promotion of household and community toilet construction.
A sanitary latrine is defined by four essential features: (1) the pit or collection system contains and isolates excreta from human contact; (2) there is no access for flies or other vectors to the pit; (3) there is no contamination of surface or groundwater; (4) there is no odour nuisance. Common sanitary latrine designs in India include the pour-flush latrine (most common household design; water seal prevents flies and odour), the VIP (Ventilated Improved Pit) latrine (screened vent pipe creates airflow that traps and kills flies attracted to the pit), and the twin-pit latrine (SBM-promoted design: two alternating pits—while one fills, the other compostes, producing pathogen-free manure after 18 months).
Where sewers exist, sewage treatment processes the collected wastewater before discharge to water bodies. The stages and their performance are shown in the figure below.
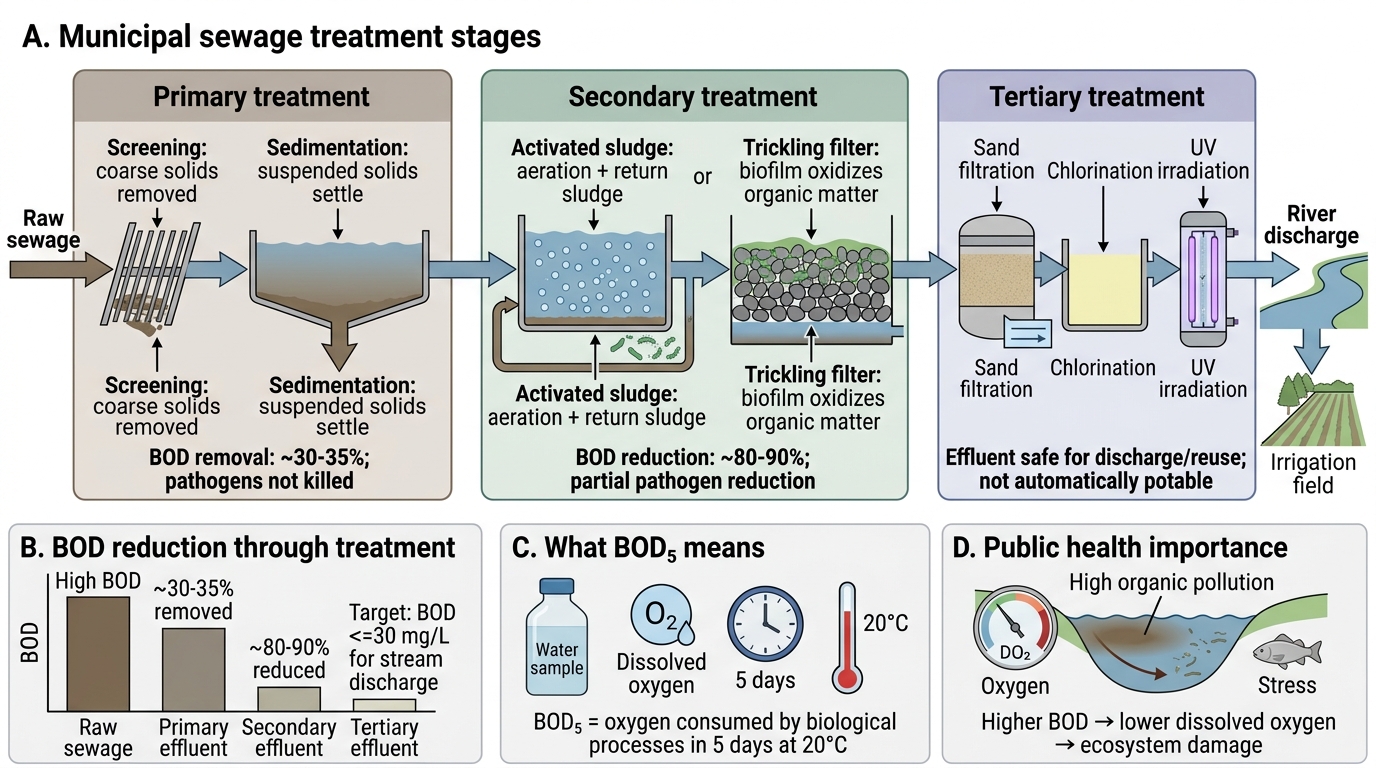
Municipal Sewage Treatment and BOD Reduction
Primary treatment (physical): screening removes coarse solids; sedimentation removes suspended solids. Removes ~30-35% of BOD; does NOT kill pathogens.
Secondary treatment (biological): the activated sludge process aerates sewage in tanks with return sludge containing active microorganisms that oxidise organic matter; or a trickling filter passes sewage over a bed of stones or plastic media coated with a biofilm. Reduces BOD by 80-90%. Some pathogen reduction occurs but effluent is not safe for drinking.
Tertiary treatment (polishing): sand filtration, chlorination, or UV irradiation produce effluent of sufficient quality for safe discharge to sensitive water bodies or even reuse for irrigation. CPCB discharge standards require effluent BOD ≤30 mg/L for general stream discharge.
BOD (Biochemical Oxygen Demand) is the standard measure of organic pollution: the amount of dissolved oxygen consumed by biological processes in a water sample over 5 days at 20°C (BOD5). Higher BOD = higher organic pollution load = greater oxygen depletion of receiving water bodies, causing fish kill and ecosystem damage.