Page 7 of 21
CM7.4 | CM7.4 | Morbidity and Mortality Measures — SDL Guide
Learning Objectives
- Define, calculate, and interpret morbidity indicators — incidence rate, attack rate, secondary attack rate, point and period prevalence — from a given dataset (CM7.4)
- Define, calculate, and interpret mortality indicators — crude death rate, cause-specific death rate, case fatality rate, IMR, NMR, U5MR, MMR — from a given dataset (CM7.4)
- Explain why standardisation is needed when comparing rates across populations with different age structures
- Interpret trends in India's key health indicators (IMR, MMR, U5MR) and their policy implications
INSTRUCTIONS
Numbers without denominators are meaningless in public health — 100 diarrhoea deaths sounds alarming, but whether it represents a crisis or a baseline depends entirely on the population at risk and the timeframe. Morbidity and mortality measures are the standardised tools that make disease counts comparable across populations, places, and time. This module teaches you to calculate these measures correctly, interpret them accurately, and use them to generate actionable public health insights.
References
- Park's Textbook of Preventive and Social Medicine, 27th edition — Chapter 2: Epidemiology (Rates and Ratios) (textbook)
- Gordis L. Epidemiology, 5th edition — Chapter 3: Measuring the Occurrence of Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2000, a newspaper reported that 'malaria killed 500 people in State X last year.' In 2001, it reported 'malaria killed 650 people in State Y.' Which state had the bigger malaria problem? You cannot answer this question without knowing the population of each state, the proportion of the population that was exposed, and whether the two years were comparable in terms of climate and vector density. Raw numbers — absolute counts — tell us almost nothing for public health decision-making. Rates — numbers expressed per unit of population and time — are the language of epidemiology. Without them, we cannot prioritise, allocate resources, or measure progress. This module teaches you to calculate rates correctly, interpret them accurately, and avoid the common errors that distort public health judgement.
WHY THIS MATTERS
India's health policy rests on a set of tracked indicators: the Infant Mortality Rate, the Maternal Mortality Ratio, the Under-5 Mortality Rate, and (for morbidity) incidence rates of tuberculosis, malaria, and HIV. These numbers determine which states receive priority funding, which programmes are scaled up, and which interventions are judged successful. As a community medicine practitioner — and as a doctor who will generate case notifications and contribute to health records — you are part of the system that produces these numbers. Understanding how they are calculated, and where they can be distorted, makes you a more reliable contributor to that system.
RECALL
From basic statistics in Year 1, recall: (1) A proportion is a ratio in which the numerator is a subset of the denominator (e.g. 20 cases / 200 persons = 0.10 = 10%). (2) A rate is a proportion that additionally includes a time dimension (e.g. 20 new cases per 200 persons per year = 10 per 100 per year). (3) A ratio compares two quantities that may not have the same denominator (e.g. sex ratio = males / females). Many measures called 'rates' in medicine are actually proportions (case fatality rate, attack rate) — the terminology is historically entrenched, but the mathematical distinction matters for interpretation.
Why Health Systems Count: The Burden of Morbidity and Mortality
Every health programme begins with measurement: how many people are affected, at what rate, and with what consequences? The magnitude of a health problem is quantified through morbidity measures (illness, disease occurrence) and mortality measures (death). Raw counts — absolute numbers of cases or deaths — are useful for logistics (how many beds, how many treatment courses) but not for comparison across populations of different size. A district with 1,000 diarrhoea deaths in a population of 500,000 has a death rate of 2 per 1,000, which is half the rate of a district with 500 deaths in a population of 100,000. Without standardising to population size and time, inter-district and inter-state comparisons are misleading.
India's health system uses these measures to track progress toward national goals. The National Health Policy 2017 set targets including: IMR ≤28 per 1,000 live births, MMR ≤100 per 100,000 live births, and U5MR ≤23 per 1,000 live births by 2025. NFHS-5 (2019-21) reported IMR of approximately 35 and U5MR of approximately 32 at the national level, and SRS (2018-20) reported MMR of approximately 97 — indicating substantial progress from the 2005 baseline (IMR ≈58, MMR ≈254) but with considerable state-level variation. These numbers drive where Mission Indradhanush focuses, where conditional cash transfers for delivery care are expanded, and where skilled birth attendance programmes are intensified. Knowing how to generate and interpret them is an operational skill, not a theoretical exercise.
Incidence and Prevalence: Measuring Morbidity
Incidence measures the rate at which new disease events occur in a population at risk during a defined time period. The formula is:
Incidence rate = (Number of new cases in time period) / (Population at risk at midpoint of period) × multiplier (1,000 or 100,000 per year)
The denominator must be the population at risk — individuals who could develop the disease. Persons who already have the disease or are immune are excluded. This distinction matters: in calculating the incidence of a second heart attack, the denominator is only those who have already had one first heart attack — not the general population.
Two special forms of incidence are used in outbreak investigation:
- Attack rate: the proportion of a defined exposed group that develops illness during a specific outbreak. Formula: attack rate = (cases) / (exposed persons) × 100. It is not a true rate (no time unit), but a proportion used only in outbreak contexts where the exposure event and susceptible population are clearly delimited (e.g. food-poisoning outbreak at a wedding: cases / persons who attended × 100).
- Secondary attack rate (SAR): the proportion of susceptible household (or group) contacts who develop illness within the maximum incubation period of the disease after exposure to a primary case. SAR = (new cases among susceptible contacts) / (susceptible contacts of primary case) × 100. SAR measures transmissibility within close contact groups and is high for measles (~90%) and low for leprosy (~5–10%).
Prevalence measures the proportion of a defined population with the disease (new and old cases) at a specified time.
- Point prevalence: proportion of population with disease at a single time point. Formula: (existing cases at time T) / (total population at T) × 100 (or 1,000).
- Period prevalence: proportion of population that had disease at any time during a defined period; numerator includes both old cases (pre-existing) and new cases (incident) during that period.
The critical relationship linking the two is:
Prevalence ≈ Incidence × Mean duration of disease (Neyman's formula, for stable conditions)
This relationship has important implications: a disease with low incidence but long duration (e.g. Type 1 diabetes, epilepsy) has a prevalence far exceeding its incidence. A disease with high incidence but short duration (e.g. common cold, acute diarrhoea) has lower prevalence at any point in time. It also explains why effective treatment reduces prevalence even if incidence stays the same (by shortening mean duration).
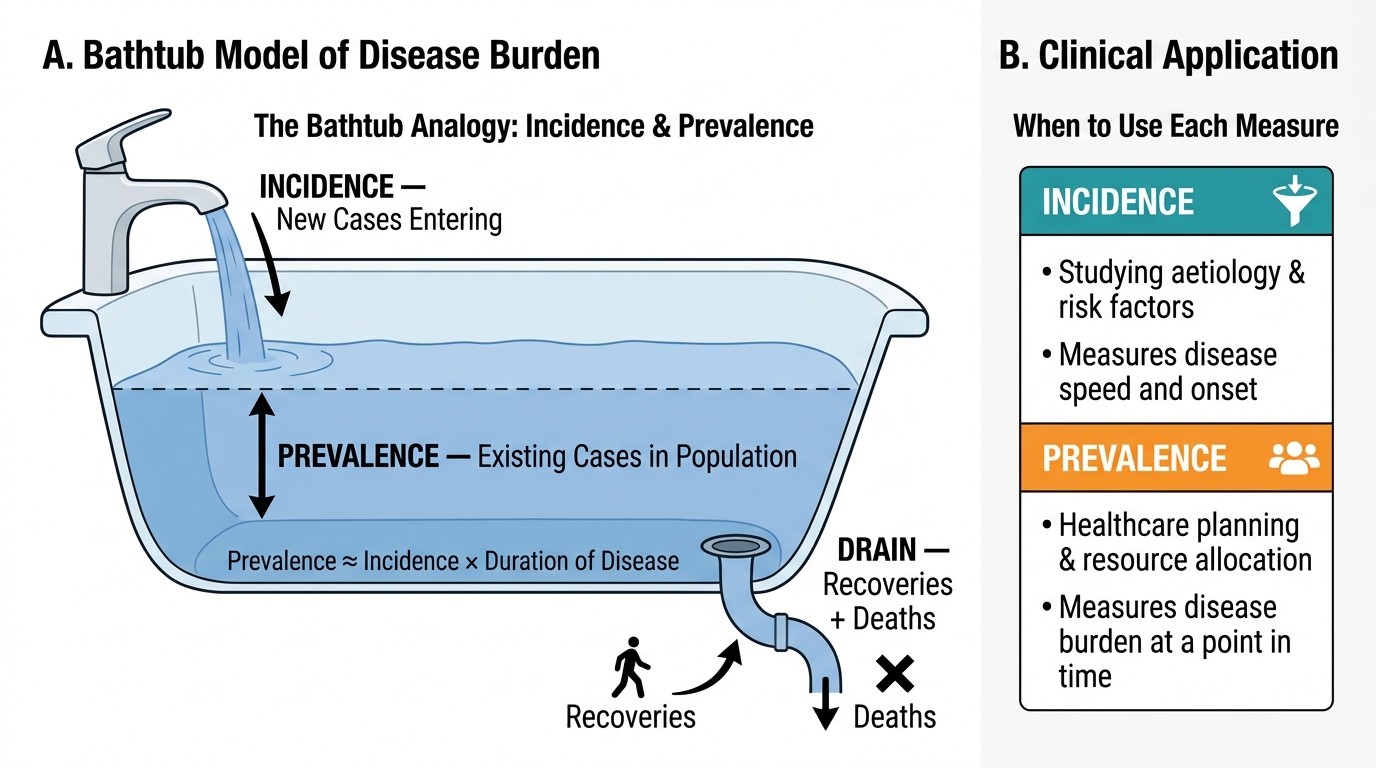
Bathtub Analogy: Incidence, Prevalence, and Disease Burden
When to use incidence vs prevalence:
- Incidence is the measure for studying aetiology and risk factors — it tells you how fast disease is occurring and in whom.
- Prevalence is the measure for healthcare planning and resource allocation — it tells you how many persons in the population need care at any given time.
SELF-CHECK
In a village of 1,000 persons, 50 had diabetes at the start of 2023. During 2023, 20 new cases of diabetes were diagnosed. All 50 existing cases and 15 of the new cases were alive and had diabetes at the end of 2023. What is the point prevalence of diabetes at the end of 2023?
A. 5% (50/1,000)
B. 7% (70/1,000)
C. 6.5% (65/1,000)
D. 2% (20/1,000)
Reveal Answer
Answer: C. 6.5% (65/1,000)
Point prevalence at the end of 2023 = (existing cases surviving + new cases surviving) / total population = (50 + 15) / 1,000 = 65/1,000 = 6.5%. The 5 new cases who died during 2023 are excluded from end-of-year point prevalence. The 20 new cases is the incidence during 2023. The 5/50 at start of year is the starting point prevalence (5%). Option C (6.5%) is correct.
Mortality Measures: From Crude to Cause-Specific
Mortality measures quantify death occurrence in populations. They differ from morbidity measures in that the outcome (death) is unambiguous and permanent — though cause-of-death attribution remains a major data quality issue in India.
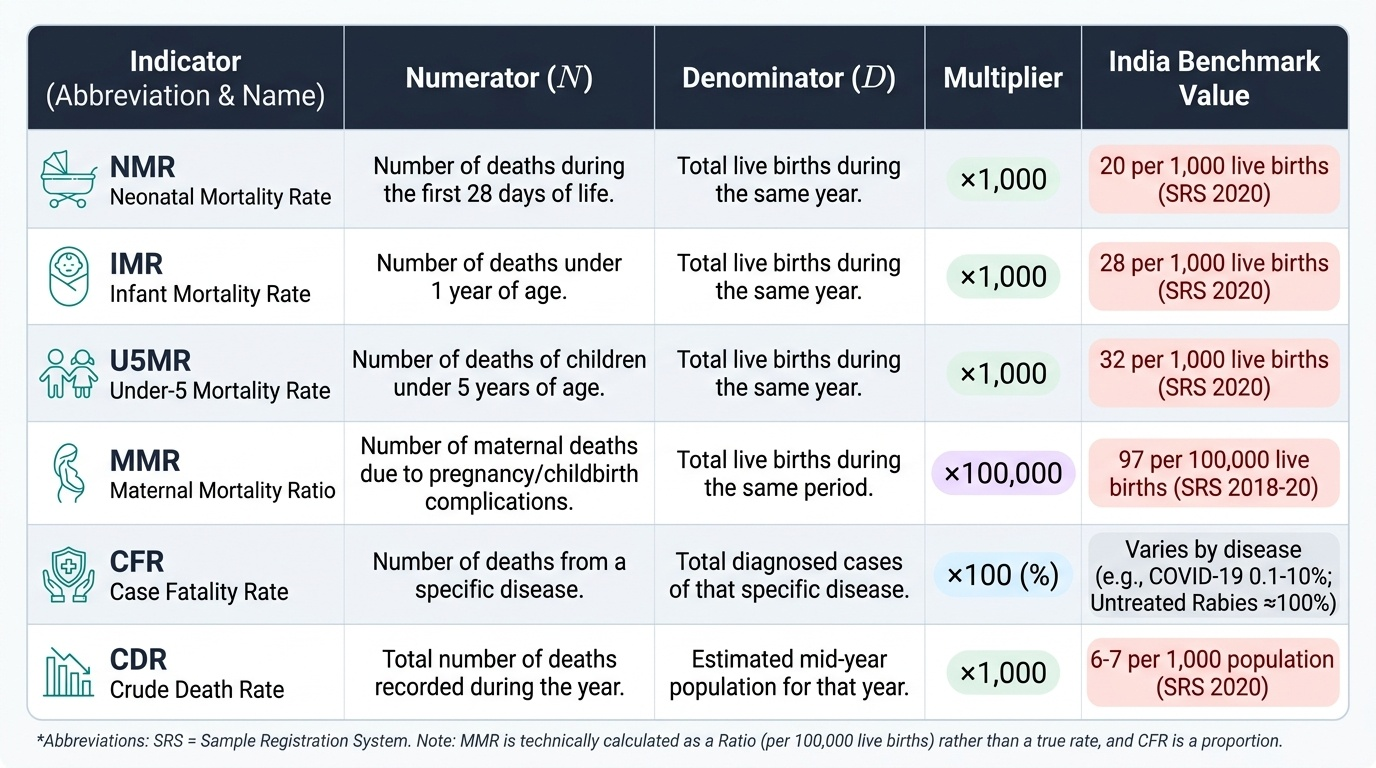
Crude Death Rate (CDR) = Total deaths / Mid-year population × 1,000. 'Crude' indicates it is not adjusted for age — populations with older age structures will have higher CDRs simply because old age is associated with higher mortality, not because they have worse health systems. India's CDR is approximately 6–7 per 1,000 (SRS 2020).
Cause-specific death rate = Deaths from a specific cause / Mid-year population × 100,000 per year. This allows comparison of mortality burdens across causes (tuberculosis: ~36 per 100,000; cardiovascular disease: ~272 per 100,000 in India).
Proportional mortality rate (PMR) = Deaths from a specific cause / Total deaths × 100. Unlike cause-specific death rates, PMR does not use the living population in the denominator — it tells you the proportion of deaths attributable to a cause. Useful when population data are unavailable (e.g. hospital deaths). Limitation: a high PMR for one cause may simply reflect a low burden of other causes in a population, not a high absolute mortality from that cause.
Case Fatality Rate (CFR) = Deaths from a disease / Total cases of that disease × 100. Measures the killing power or lethality of a disease. A high CFR indicates severe disease in clinical populations (COVID-19 CFR varied from <0.1% in young adults to >10% in elderly; untreated rabies CFR ≈100%). Technically a proportion, not a rate.
Infant Mortality Rate (IMR) = Deaths in infants <1 year / Live births in the same year × 1,000. IMR is the most widely used summary indicator of child health and is strongly correlated with socioeconomic development. It is disaggregated into:
- Neonatal Mortality Rate (NMR) = Deaths in first 28 days / Live births × 1,000
- Post-neonatal Mortality Rate = Deaths from 28 days to <1 year / Live births × 1,000
Under-5 Mortality Rate (U5MR) = Deaths in children <5 years / Live births × 1,000. Captures mortality in both infancy and the 1–4 year age group (when diarrhoeal and pneumonia deaths remain high).
Maternal Mortality Ratio (MMR) = Maternal deaths (deaths during pregnancy or within 42 days of termination of pregnancy, from causes related to or aggravated by the pregnancy) / 100,000 live births. Note: the denominator is live births, not the total pregnant women population — making it technically a ratio (not a rate), but universally called the MMR. India's MMR has fallen from 254 in 2004-06 to approximately 97 in 2018-20 (SRS).
Standardised Mortality Ratio (SMR) = Observed deaths in study population / Expected deaths × 100, where expected deaths are calculated using age-specific rates from a standard reference population applied to the study population's age distribution. An SMR >100 indicates higher-than-expected mortality; <100 indicates lower. This is indirect standardisation.
Provided image
SELF-CHECK
During a cholera outbreak in a district, 250 persons are diagnosed with cholera and 18 die. The district population is 200,000. Which measure correctly quantifies the lethality of cholera in this outbreak?
A. Crude death rate = 18/200,000 × 1,000 = 0.09 per 1,000
B. Attack rate = 250/200,000 × 100 = 0.125%
C. Case fatality rate = 18/250 × 100 = 7.2%
D. Cause-specific death rate = 250/200,000 × 100,000 = 125 per 100,000
Reveal Answer
Answer: C. Case fatality rate = 18/250 × 100 = 7.2%
The Case Fatality Rate (CFR) = Deaths from the disease / Cases of the disease × 100 = 18/250 × 100 = 7.2%. The CFR specifically measures the killing power (lethality) of a disease in a defined case series — it answers: 'of those who got the disease, what proportion died?' The crude death rate uses the whole population (not just cases) and is not the measure of lethality. The attack rate measures incidence in the exposed group. The cause-specific death rate uses the whole population and a longer time denominator.