Page 1 of 8
CM19.1-4 | CM19.1-4 | Essential Medicine List, Primary Care Requirements and Counterfeit Prevention — SDL Guide
Learning Objectives
- Define essential medicines and explain the purpose and structure of the WHO Essential Medicines List (EML) and India's National List of Essential Medicines (NLEM 2022)
- Describe the role of essential medicines in primary health care, including the P-drug concept and rational drug use principles
- Define counterfeit, substandard, and falsified medicines; describe their public health impact and prevention strategies
- Demonstrate understanding of how to identify essential medicines and calculate medicine requirements at a primary health care facility
INSTRUCTIONS
Every year, millions of patients in low- and middle-income countries receive either no medicines, wrong medicines, or counterfeit medicines. The essential medicines concept — that a carefully selected, evidence-based list of drugs can meet the priority health needs of a population at affordable cost — is one of the most powerful tools in public health pharmacy. As a future medical officer, you will prescribe from the NLEM, manage a PHC drug store, and be the first line of defence against substandard and falsified medicines entering your facility. This module builds the framework that makes all of that possible.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 23 — Essential Drugs and Rational Drug Use (textbook)
- WHO. WHO Model List of Essential Medicines, 28th edition. Geneva: WHO; 2023 (document)
- Ministry of Health and Family Welfare. National List of Essential Medicines 2022. New Delhi: MOHFW; 2022 (document)
- WHO. Substandard and falsified medical products. Fact sheet. Geneva: WHO; 2023 (document)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 60-year-old diabetic woman presents to your PHC in rural Rajasthan. Her blood sugar is uncontrolled on the metformin she purchased from a local pharmacy. She shows you the tablet strip: the embossing is uneven, the packaging is slightly different from what you stock, and the price is suspiciously low. Your pharmacist runs a simple visual inspection. The tablets fail. They are falsified medicines — deliberately mislabelled products with no active ingredient. Meanwhile, your drug store has run out of insulin because the procurement calculation submitted three months ago was wrong. Two crises, one appointment — and both stem from failures in the essential medicines system. This module is about building that system correctly.
WHY THIS MATTERS
The essential medicines framework directly determines what medicines are available at your PHC, how much you order, what you can legally prescribe under government schemes, and how you protect patients from substandard and falsified products. India's NLEM 2022 is the basis for the Jan Aushadhi scheme, the PMJAY drug formulary, and state essential medicine lists used for government procurement. Understanding EML selection criteria is not academic — it explains why some proven drugs are on the list and others are not, and why that matters for equitable care. The counterfeit medicines problem kills tens of thousands annually globally and affects Indian patients directly.
RECALL
Activate prior knowledge before proceeding. From your pharmacology studies, recall the concept of rational drug use — prescribing the right drug, in the right dose, for the right duration, for the right patient, at the right cost. Recall that medicines have a therapeutic window and that subtherapeutic doses (common in counterfeit products) not only fail to treat but actively drive antimicrobial resistance. From your community medicine studies of health planning, recall that drug procurement follows the morbidity profile of the catchment population. From your international health module (CM18), recall that WHO sets global norms — including the EML — which then inform national lists such as India's NLEM.
The Essential Medicines Burden: Why Drug Access Remains a Global Health Crisis
Essential medicines are defined by WHO as those that satisfy the priority health care needs of the population, selected with due regard to disease prevalence, evidence of efficacy and safety, and comparative cost-effectiveness. The concept was operationalised when the WHO Expert Committee on the Selection and Use of Essential Medicines convened in 1977 and produced the first WHO Model List of Essential Medicines, containing 208 medicines for the most prevalent health conditions in low-resource settings.
The burden of inadequate access to essential medicines remains one of the greatest preventable causes of suffering and death worldwide. Approximately two billion people — roughly a quarter of humanity — lack reliable access to essential medicines, predominantly in sub-Saharan Africa and South Asia. In low-income countries, public sector availability of essential generic medicines averages only 38%, compared to 63% in the private sector where prices are substantially higher. A single course of first-line treatment for pneumonia in a child can cost several days of wages for a poor household in an LMIC — translating directly into non-adherence, treatment failure, and preventable death.
In India, the access gap manifests unevenly. Urban tertiary facilities stock hundreds of medicines, while a rural PHC may have only 30–50 medicines available at any time, and stock-outs are endemic. A 2019 survey of Indian public health facilities found that the average availability of medicines on state essential medicines lists was 62% — meaning nearly four in ten prescribed medicines were unavailable at the point of care. Patients forced to purchase from private pharmacies pay out-of-pocket prices that can be 10–40 times higher than the procurement price for the same generic medicine.
The essential medicines concept responds to this crisis not by trying to make all medicines available everywhere — an impossibility — but by ensuring that the medicines most likely to address the actual disease burden of the population are reliably available, affordable, and of assured quality. This is the foundational public health logic that the rest of this module builds on.
Determinants of Medicine Access: Selection, Pricing, and Regulatory Barriers
Medicine access failure is multidetermined — understanding each determinant is necessary to design effective interventions. The WHO framework identifies four access barriers: rational selection, affordable prices, sustainable financing, and reliable health and supply systems. When any one fails, access collapses.
Irrational drug use is both a determinant and a consequence of access failure. WHO's 1985 Nairobi Conference on the Rational Use of Drugs produced the canonical definition: patients receive medicines appropriate to their clinical needs, in doses meeting their individual requirements, for an adequate period of time, and at the lowest cost to them and their community. Studies consistently show that globally, over 50% of medicines are prescribed, dispensed, or sold inappropriately. In India, studies have documented polypharmacy (>4 drugs per prescription) in primary care, overuse of antibiotics for viral infections, underprescribing of essential antihypertensives, and inappropriate use of injectable medicines when oral routes are sufficient. Irrational prescribing is a learned behaviour shaped by medical education, pharmaceutical marketing, patient demand, and the absence of structured prescribing tools — which is why the P-drug concept and essential medicines lists are educational as well as operational tools.
Pricing determinants include patent protection, pharmaceutical market concentration, and the absence of price regulation. Generic competition — the primary mechanism by which essential medicines become affordable — requires that a medicine's patent has expired or been bypassed through TRIPS flexibilities (compulsory licensing, as India has used for antiretrovirals). India's DPCO (Drug Price Control Order) sets ceiling prices for medicines on the NLEM, making affordability a regulatory function directly tied to NLEM inclusion.
Regulatory determinants include the capacity of national medicines regulatory authorities to approve, inspect, and monitor quality. A weak CDSCO means substandard and falsified medicines enter the supply chain. The social determinants of medicine access — income, literacy, distance to facility, gender, and caste — shape who can access even what is theoretically available. A medicine on the NLEM that is only available in the district hospital but not the sub-centre fails a patient who cannot travel two hours with a febrile child.
For the essential medicines framework to succeed, these determinants must be addressed in sequence: rational selection → affordable pricing (DPCO link) → adequate financing (budget allocation) → reliable supply (procurement and logistics) → quality assurance (CDSCO, pharmacovigilance).
SELF-CHECK
WHO defined rational drug use at the Nairobi Conference in 1985. Which of the following elements is included in the WHO definition of rational drug use?
A. Prescribing the newest available drug for a given indication regardless of cost
B. Providing medicines at the lowest cost to the patient and community
C. Selecting medicines based on brand name recognition among patients
D. Prescribing injectable medicines preferentially over oral formulations for faster effect
Reveal Answer
Answer: B. Providing medicines at the lowest cost to the patient and community
The WHO 1985 Nairobi definition of rational drug use specifies that medicines should be appropriate to the clinical need, in doses meeting individual requirements, for an adequate period, and at the lowest cost to the patient and community. Cost-effectiveness is an explicit component. Newest, brand-name, or injectable preferences without clinical justification are examples of irrational use.
WHO EML and India's NLEM 2022: Structure, Selection Criteria, and PHC Role
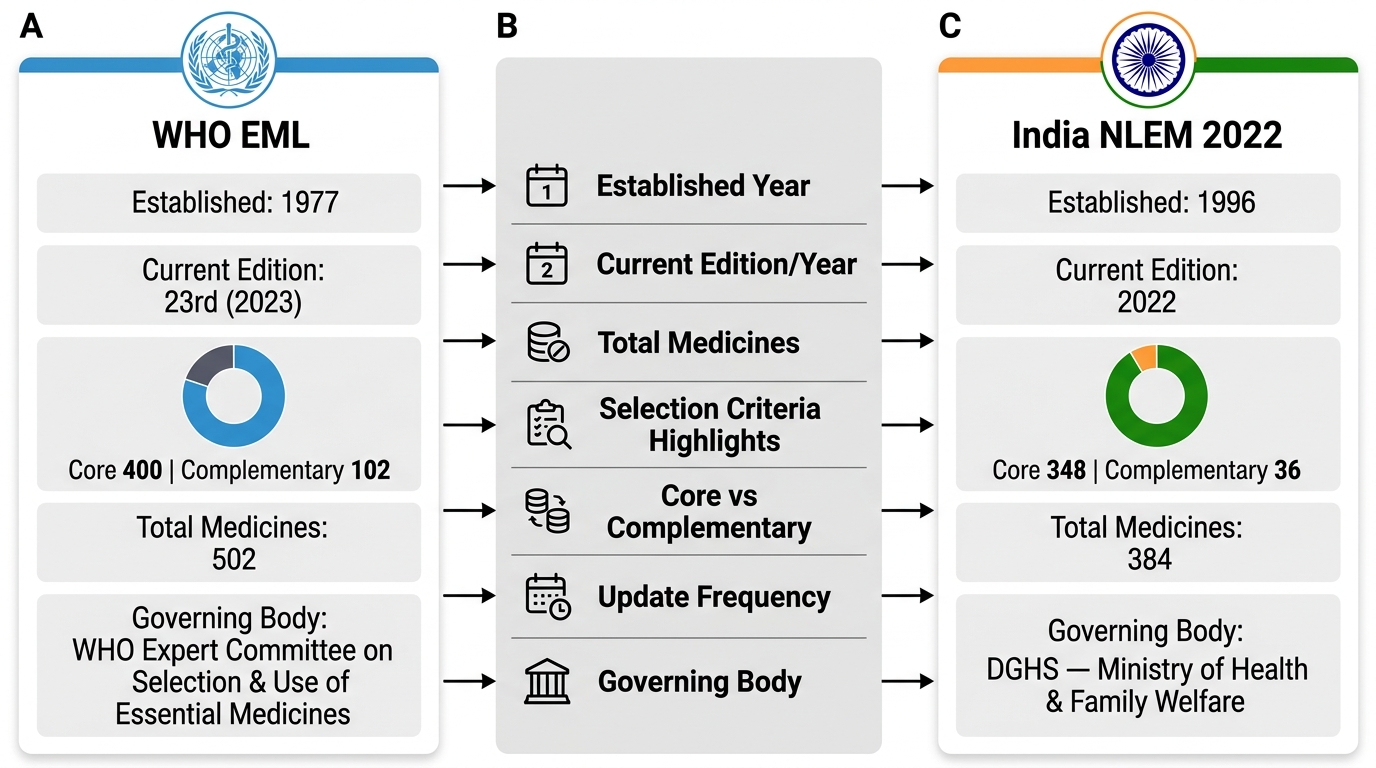
The WHO Model List of Essential Medicines (WHO EML) is now in its 28th edition (2023), containing 502 medicines across a core list and a complementary list. The core list presents minimum medicine needs for a basic health care system; the complementary list includes essential medicines for priority diseases requiring specialist care or more complex management. Both are essential — the complementary list is not a 'second tier' of importance but a set requiring referral infrastructure.
WHO EML selection criteria, applied by the Expert Committee, include: (1) relevance — the medicine addresses a priority health need as defined by epidemiological burden; (2) proven efficacy and safety — based on valid scientific evidence, from randomised controlled trials or established clinical experience; (3) comparative cost-effectiveness — the medicine is not simply cheap but offers best value per health outcome (QALY or similar metric) compared to alternatives for the same indication; (4) quality — assured pharmaceutical quality including stability under local conditions; (5) feasibility — can be used in available health system infrastructure.
INDIA'S National List of Essential Medicines 2022 (NLEM 2022) adapted this framework for India's disease burden, regulatory environment, and health system capacity. NLEM 2022 contains 384 medicines across 27 therapeutic categories, updated from NLEM 2015 (376 medicines). Key changes in NLEM 2022 include: addition of newer antiretrovirals (dolutegravir-based regimens), oral anti-TB drugs (bedaquiline, delamanid), newer antifungals, and removal of obsolete medicines. NLEM inclusion automatically triggers DPCO price regulation — the government sets ceiling prices for NLEM medicines through the National Pharmaceutical Pricing Authority (NPPA), making this list politically and economically consequential, not just clinical.
WHO EML vs India NLEM 2022 — Comparative Overview
Essential medicines in primary health care are operationalised through the PHC formulary, which is typically a state-adapted subset of NLEM aligned with the disease burden of the catchment population. A typical PHC formulary contains 50–80 medicines covering the most common acute and chronic conditions managed at primary level. The P-drug (personal drug) concept, developed at the University of Groningen, operationalises rational selection at the individual prescriber level: for each common clinical problem, the prescriber identifies their preferred drug (P-drug) based on efficacy, safety, suitability, and cost. The P-drug is the prescriber's personal formulary — a practical tool to resist irrational prescribing pressures from pharmaceutical promotion.
Seven steps to rational drug use (WHO guide to good prescribing): (1) define the patient's problem; (2) specify the therapeutic objective; (3) verify that your P-drug is suitable for this patient; (4) start treatment — write prescription; (5) give information, instructions, and warnings; (6) monitor and stop treatment; (7) consider referral if needed. These steps are applicable at every PHC consultation and are the operational translation of the essential medicines concept into clinical practice.
| Framework | Established | Current Version | Medicines Count | Key Feature |
|---|---|---|---|---|
| WHO EML | 1977 | 28th edition, 2023 | 502 (core + complementary) | Model list — each country adapts |
| India NLEM | 1996 | NLEM 2022 | 384 across 27 categories | DPCO pricing trigger; PHC formulary basis |