Page 6 of 25
CM1.3-5 | CM1.3-5 | Determinants and Natural History of Disease — SDL Guide (Part 2)
Levels of Prevention — Primordial, Primary, Secondary, Tertiary
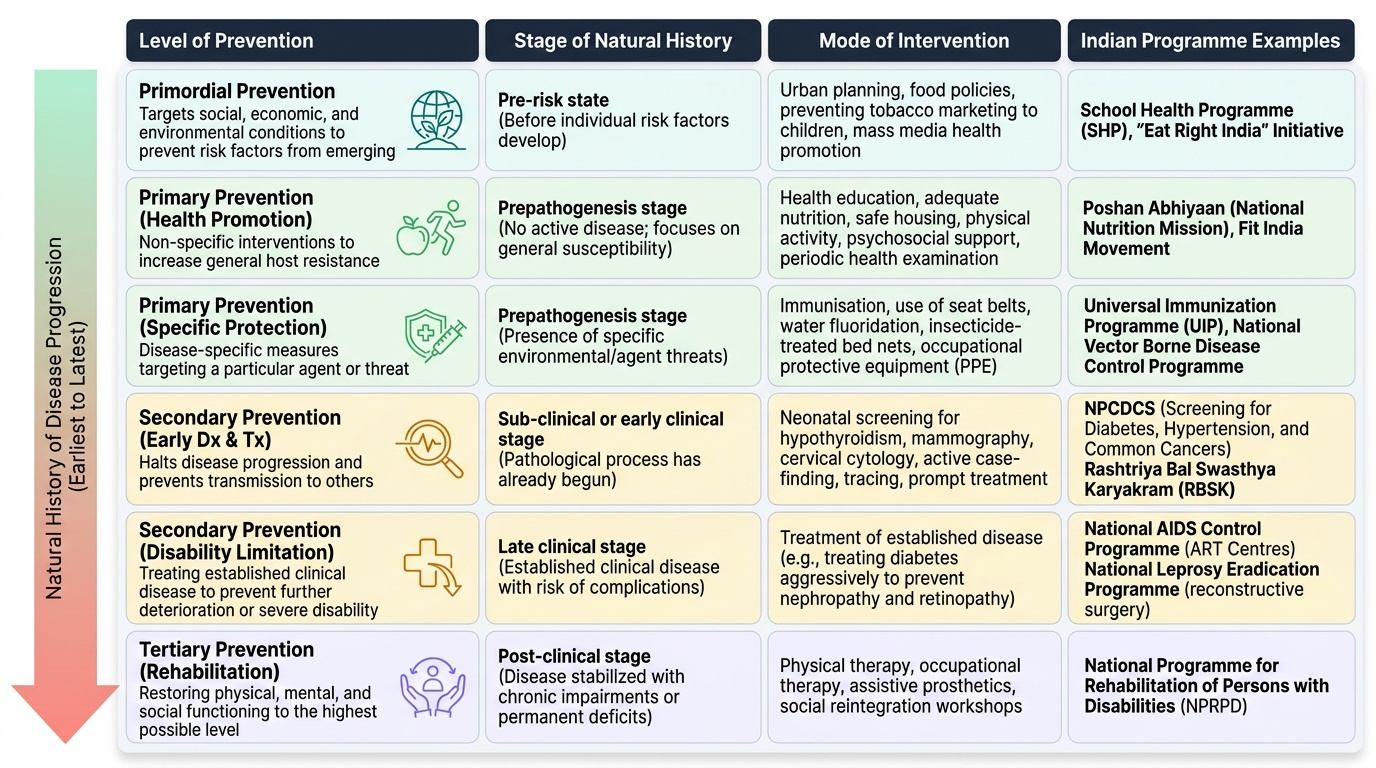
Leavell and Clark (1965) introduced the classical framework of three levels of prevention — primary, secondary, and tertiary — which has since been extended by adding primordial prevention to address the social and environmental conditions that give rise to risk factors before the risk factors themselves emerge. The four levels, from earliest to latest in the natural history, are:
Primordial Prevention targets the social, economic, and environmental conditions that allow risk factors to establish themselves in a population. It acts even earlier than primary prevention — before individuals have developed individual risk factors. Examples: preventing the adoption of sedentary lifestyles and high-fat diets in rapidly urbanising populations through urban planning, food policy, and mass media; preventing tobacco marketing to children. India's School Health Programme includes primordial components.
Primary Prevention acts during the prepathogenesis stage to prevent disease from developing. It has two distinct modes:
- Health promotion (non-specific): increases general host resistance without targeting a specific disease. Includes health education, adequate nutrition, safe housing, physical activity, psychosocial support, periodic health examination. These measures benefit the host against a wide range of potential agents.
- Specific protection (disease-specific): targets a particular agent or disease mechanism. Includes immunisation (measles vaccine prevents measles), use of seat belts (trauma prevention), fluoridation of water supplies (dental caries prevention), insecticide-treated bed nets (malaria prevention), and occupational protective equipment.
Secondary Prevention acts once the pathological process has begun — specifically in the sub-clinical or early clinical stage — to halt disease progression and prevent complications. It has two modes:
- Early diagnosis and treatment: screening programmes (neonatal screening for hypothyroidism, mammography, cervical cytology), case-finding, contact tracing; followed by prompt treatment to limit spread and severity.
- Disability limitation: treating established clinical disease to prevent further deterioration, complications, or the transition to severe disability. For example, treating diabetes aggressively to prevent nephropathy and retinopathy; treating hypertension to prevent stroke.
Tertiary Prevention acts at the stage of advanced disease or established disability to restore maximum possible function and reduce suffering:
- Rehabilitation: physical (physiotherapy after stroke), vocational (occupational therapy after limb loss), social (reintegration support), and psychological (counselling for PTSD). Rehabilitation does not reverse the underlying pathology but minimises its impact on quality of life.
Provided image
> Key exam trap: Disability limitation is classified under SECONDARY prevention (Leavell & Clark), NOT tertiary. Tertiary prevention = rehabilitation only. Many students misplace disability limitation.
SELF-CHECK
A polio-affected child receives physiotherapy to improve muscle function and is enrolled in a vocational training programme. This intervention belongs to which level of prevention?
A. Primordial prevention
B. Primary prevention — specific protection
C. Secondary prevention — disability limitation
D. Tertiary prevention — rehabilitation
Reveal Answer
Answer: D. Tertiary prevention — rehabilitation
Physiotherapy and vocational training for an already-disabled child aim to restore maximum function and social participation — this is rehabilitation, which is tertiary prevention. Disability limitation (secondary prevention) would be treating the acute polio to prevent the disability from occurring or worsening while still reversible. Once established, restoring function = tertiary.
Mapping Prevention to Natural History — The Intervention Logic
The power of combining the natural history framework with the levels of prevention classification lies in creating a clear logic of WHEN each preventive intervention is appropriate and WHY. The two frameworks map onto each other precisely, making clinical and public health decision-making more systematic.
During the prepathogenesis stage, the host is susceptible but not yet pathologically affected. This is the window for primordial prevention (remove societal risk conditions) and primary prevention (health promotion to strengthen host resistance; specific protection to block agent transmission or host susceptibility). A TB patient's contacts who are tuberculin-negative, well-nourished, and living in adequately ventilated housing are in the prepathogenesis stage — the appropriate intervention is isoniazid preventive therapy (specific protection) plus nutrition counselling (health promotion).
During early pathogenesis (sub-clinical disease), the biological process has started but the patient has not presented clinically. This is the window for secondary prevention — early diagnosis and treatment via screening, contact tracing, or case-finding. The same TB contacts who are tuberculin-positive on skin test but smear-negative are in early pathogenesis — the appropriate intervention is X-ray screening and, if progressive, treatment initiation.
During advanced pathogenesis (clinical disease), the appropriate secondary prevention mode shifts to disability limitation — treating the established disease to prevent complications. An active TB case on DOTS therapy that is managed to prevent drug resistance, empyema, or pericarditis exemplifies disability limitation.
Finally, a TB patient who develops residual bronchiectasis after completing treatment and is enrolled in pulmonary rehabilitation is receiving tertiary prevention. This systematic mapping makes the levels of prevention not merely classificatory but predictive: given a disease and its stage, the appropriate prevention level follows logically.
Evaluating Prevention Strategies — Effectiveness and Metrics
Knowing the correct preventive level to target is necessary but not sufficient — public health also requires evaluating whether interventions actually work, using measurable outcomes. The choice of metric depends on the level of prevention being evaluated.
For primary prevention, the key metric is incidence reduction — fewer new cases arising in the population. Vaccine programme effectiveness, for example, is measured by comparing incidence rates in vaccinated vs unvaccinated populations, or by tracking disease-specific incidence trends before and after programme introduction. India's success in polio eradication (achieved in 2014) is measured by incident polio case counts reaching zero.
For secondary prevention, the key metrics are case-fatality rate (CFR) reduction (screening finds cases earlier, when treatment is more effective, so fewer die from the disease) and complications prevented (e.g. reduced blindness rates from diabetic retinopathy screening). Early detection of cervical cancer through the cervical cytology programme aims to shift the stage distribution toward earlier, more curable stages.
For tertiary prevention, metrics include disability rates, functional independence scores, and quality of life measures — which require different tools from mortality statistics. India's National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke (NPCDCS) incorporates rehabilitation metrics alongside incidence data.
India's surveillance infrastructure for monitoring these metrics includes the Integrated Disease Surveillance Programme (IDSP) for communicable diseases, the National Cancer Registry Programme (NCRP) for cancer incidence, and periodic surveys such as NFHS and LASI (Longitudinal Ageing Study in India) for non-communicable and functional outcomes. A community physician must be familiar with these sources to critically appraise prevention programme effectiveness.
SELF-CHECK
A national programme introduces universal neonatal hearing screening and fitting of hearing aids for infants with congenital deafness within 3 months of birth. This primarily exemplifies which level of prevention?
A. Primordial prevention
B. Primary prevention — health promotion
C. Secondary prevention — early diagnosis and treatment
D. Tertiary prevention — rehabilitation
Reveal Answer
Answer: C. Secondary prevention — early diagnosis and treatment
Universal neonatal screening followed by prompt intervention (hearing aids) is early diagnosis and treatment — acting during the sub-clinical stage to catch the condition early and institute treatment that limits its impact on language development. This is secondary prevention. Fitting hearing aids to an adult with established deafness from a prior missed diagnosis would be tertiary (rehabilitation). The key discriminator is the timing: early (sub-clinical) detection = secondary.