Page 18 of 25
CM1.9-10 | CM1.9-10 | Communication in Doctor-Patient Relationships — SDL Guide (Part 2)
Active Listening and the Structured Consultation — Calgary-Cambridge Framework
Active listening is the disciplined skill of attending to another person's verbal and non-verbal communication with the intention of understanding, not merely waiting to respond. It is the foundation of therapeutic communication and requires deliberate practice because the natural cognitive tendency in clinical encounters is to begin formulating diagnostic hypotheses as soon as key words are heard — at the cost of hearing the patient's full account.
Active listening behaviours include:
- Attending: Physical orientation toward the patient, appropriate eye contact, and absence of interruption signal genuine attention.
- Reflecting and paraphrasing: Repeating or rephrasing key elements of what the patient said ('So you're saying the pain starts in the morning and gets better as the day goes on — is that right?') confirms understanding and signals that the patient has been heard.
- Summarising: Periodically recapping the main points gathered ('Let me make sure I've understood — you've had chest pain for three weeks, mainly on exertion, and you've noticed some shortness of breath as well') demonstrates active listening and gives the patient an opportunity to correct errors.
- Facilitating silence: Brief periods of silence after the patient speaks allow them to add information they might otherwise withhold — a common error is for the doctor to speak immediately after the patient pauses, cutting off potentially important elaboration.
Empathy and validation are closely related skills: empathy involves recognising and appropriately acknowledging a patient's emotional state ('I can see this has been really worrying for you'); validation confirms that the emotional response is understandable given the circumstances ('It makes complete sense that you'd be anxious about these symptoms'). Empathy does not require the doctor to share the patient's emotion — it requires only that the emotion be acknowledged before moving forward.
The Calgary-Cambridge Communication Skills Guide (Silverman, Kurtz, and Draper) provides a structured map of the clinical consultation, identifying 71 specific communication skills organised across five phases:
1. Initiating the session: Greeting, establishing rapport, clarifying the agenda ('Is there anything else you wanted to discuss today?')
2. Gathering information: Exploring the patient's symptoms using the disease framework (biomedical) AND the illness framework (patient's experience, ideas, concerns, expectations — ICE)
3. Physical examination: (Communication continues: explain what you're doing, maintain dignity)
4. Explanation and planning: Sharing findings, explaining in plain language, checking understanding, presenting options, reaching shared decisions
5. Closing the session: Summarising, safety-netting ('If the pain gets worse before your next appointment, please come in immediately'), confirming the plan
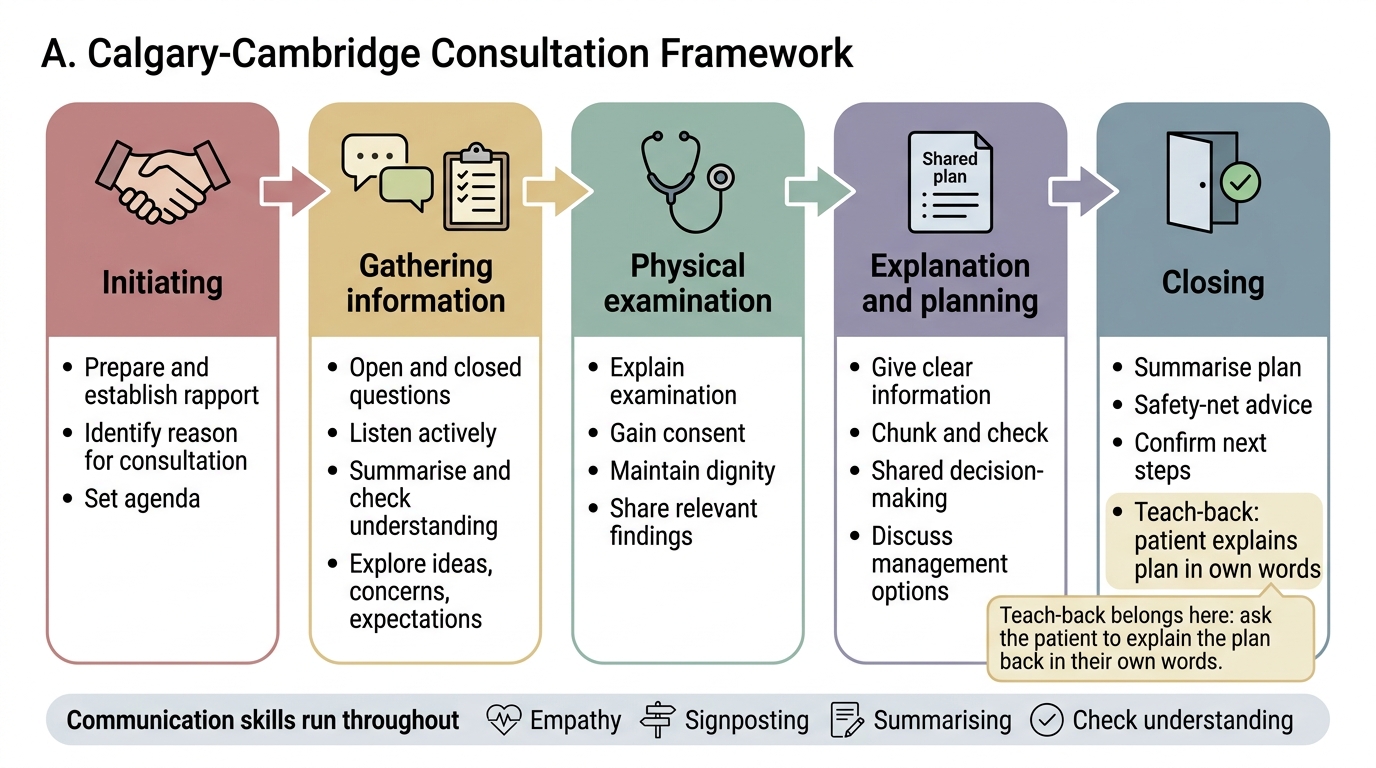
Calgary-Cambridge Consultation Framework
The teach-back technique — asking the patient to explain the plan back in their own words — is one of the most evidence-based single communication interventions. It is placed at the 'closing the session' phase in the Calgary-Cambridge model. Studies show that teach-back reduces 30-day readmission rates and substantially improves medication adherence when systematically applied.
SELF-CHECK
During a consultation, a doctor says: 'So if I've understood correctly, the pain started about two weeks ago, it's mostly in your upper abdomen, it gets worse after eating fatty food, and you've had some nausea but no vomiting — is that a fair summary?' This communication behaviour is BEST described as:
A. Closed questioning
B. Paraphrasing / summarising to confirm understanding
C. The teach-back technique
D. Motivational interviewing
Reveal Answer
Answer: B. Paraphrasing / summarising to confirm understanding
The doctor is recapping the key elements of what the patient has reported and inviting correction — this is active listening behaviour described as summarising (or paraphrasing with checking). Teach-back involves asking the PATIENT to repeat back what the doctor has explained. Motivational interviewing addresses ambivalence about behaviour change. Closed questioning would be a yes/no question about a specific symptom.
Specific Communication Skills — Breaking Bad News, Motivational Interviewing
Beyond the general consultation framework, certain clinical situations require specific communication skill sets. Two of the most important for Indian MBBS graduates are breaking bad news and motivational interviewing.
Breaking bad news is one of the most emotionally demanding communication tasks in medicine. The SPIKES protocol (Baile et al., 2000, widely used internationally) provides a structured approach:
- S — Setting: Private, comfortable setting; patient not alone if possible (support person present); doctor sitting, unhurried.
- P — Perception: Assess what the patient already knows or suspects ('What have you been told about your test results so far?') — never assume.
- I — Invitation: Establish how much detail the patient wants to receive ('Some patients prefer to know everything; others prefer me to discuss primarily with their family — what would work best for you?').
- K — Knowledge: Deliver the information in clear, simple language, in small pieces, with pauses to check understanding. Avoid medical jargon. Begin with a 'warning shot' ('I'm afraid the results show something more serious than we hoped').
- E — Empathy and Emotions: Acknowledge and respond to the patient's emotional reaction before proceeding. Do not rush past emotion to reach the 'management plan.' 'This is clearly very difficult to hear — how are you feeling right now?'
- S — Strategy and Summary: Once emotions are somewhat settled, discuss the plan and next steps. Confirm understanding. Provide written information where possible. Arrange follow-up.
Cultural considerations in breaking bad news in India: In many Indian families and communities, the family rather than the patient is the traditional information-recipient — family members may request that the patient not be told a serious diagnosis. This creates a tension between the patient's legal right to information (informed consent, autonomy) and cultural family norms. The NMC Code of Ethics requires that competent adult patients be informed; however, the clinician must navigate this sensitively and should not simply override the family's request without discussion. The question 'How much information would you like to receive about your test results, and who else should I speak to?' — asked at the outset — is the most ethically and culturally safe approach.
Motivational Interviewing (MI) is a patient-centred, directive communication method designed to help patients resolve ambivalence about behaviour change. Developed by Miller and Rollnick, MI is particularly useful when patients know they should change (smoking cessation, diet, alcohol reduction, medication adherence) but are ambivalent about actually doing so — the most common clinical scenario for lifestyle-related diseases. The four core principles of MI are: (1) Express empathy — use reflective listening to understand the patient's perspective without judgment; (2) Develop discrepancy — help the patient see the gap between their current behaviour and their own values or goals; (3) Roll with resistance — avoid direct persuasion or argumentation when a patient pushes back; (4) Support self-efficacy — reinforce the patient's confidence in their ability to change. MI is not confrontational; it is collaborative and draws on the patient's own motivation rather than imposing the clinician's.
Evaluating Communication Quality — Measurement and Feedback
Communication skills can be measured, and measurement is the foundation of improvement. Several validated assessment methods are used in medical education and clinical practice to evaluate communication quality.
Structured observation and objective assessment:
- OSCE (Objective Structured Clinical Examination): Standardised simulated patient encounters with observer-rated performance using validated communication checklists (e.g. the Calgary-Cambridge OSCE mark sheet). Each station tests a defined skill set (e.g. 'history-taking and empathy,' 'breaking bad news,' 'patient education with teach-back'). OSCEs are the NMC-mandated formative and summative assessment method for communication skills in MBBS.
- Mini-CEX (Mini Clinical Evaluation Exercise): Brief, directly observed clinical encounters (15–20 minutes) rated by a supervisor using a structured rating form covering history, physical, communication, and professionalism. Used in workplace-based assessment.
- DOPS (Direct Observation of Procedural Skills): Primarily for procedural skills, but includes a communication component (explaining the procedure, obtaining consent).
Patient-reported measures:
- Patient-Reported Experience Measures (PREMs): Standardised questionnaires completed by patients after a clinical encounter, measuring their experience of communication quality — 'Did the doctor listen to you?', 'Did the doctor explain things in a way you could understand?', 'Did you feel involved in decisions about your care?' PREMs are used in quality improvement in hospitals and health systems.
- Patient satisfaction surveys: Broader than PREMs, these measure overall satisfaction including communication, waiting time, facility quality, and outcome — useful for system-level monitoring.
Feedback in clinical teaching: Effective feedback on communication requires: (1) specific, behavioural observation ('You asked three closed questions in a row — try starting with an open question to let the patient tell their story'); (2) immediate or near-immediate timing; (3) a two-way dialogue rather than one-way critique. Pendleton's feedback model (tell me what went well → tell me what could be improved, with learner going first) is widely used in clinical communication teaching.
SELF-CHECK
A medical student completed a consultation with a standardised patient. The faculty observer now invites the student to first identify what went well, then what they would do differently, before the faculty offers their observations. This feedback approach is BEST described as:
A. Mini-CEX assessment
B. Patient-Reported Experience Measure (PREM)
C. Pendleton's feedback model
D. The teach-back method applied to clinical teaching
Reveal Answer
Answer: C. Pendleton's feedback model
Inviting the learner to self-assess first (what went well, then what to improve) before the observer adds their observations is the characteristic feature of Pendleton's feedback model — designed to promote self-reflection, reduce defensiveness, and make feedback a two-way dialogue rather than a one-way critique. Mini-CEX is a structured clinical encounter with observer rating; PREMs are patient-completed questionnaires; teach-back applies to patient communication, not to feedback on teaching.