Page 7 of 13
CM12.3-5 | CM12.3-5 | Prevention, Early Needs Identification and Elderly Programme — SDL Guide (Part 3)
Early Identification of Health Needs in the Elderly
Early identification of health needs in the elderly — the skill competency CM12.5 — is operationalised through standardised screening tools applied at first contact and at regular intervals. The concept here is not mass population screening in the traditional sense but case-finding: actively offering testing to high-risk individuals who present to services for any reason.
The key domains of early identification and the tools for each:
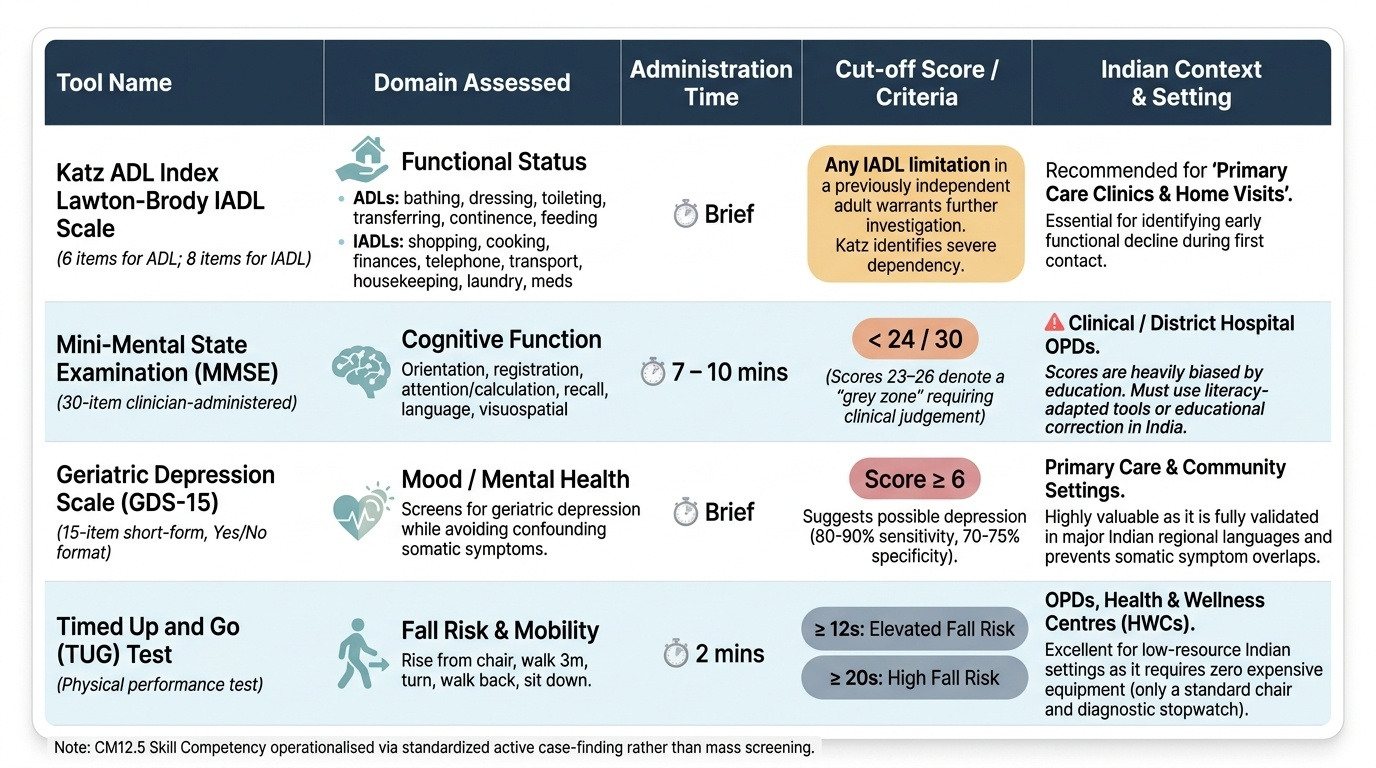
Functional status (ADL/IADL): The Katz ADL Index (6 items: bathing, dressing, toileting, transferring, continence, feeding) identifies severe dependency. The Lawton-Brody IADL Scale (8 items: shopping, cooking, finances, telephone, transport, housekeeping, laundry, medications) is more sensitive to early decline. Any IADL limitation in a previously independent elderly person warrants investigation and intervention.
Cognitive function — MMSE: The Mini-Mental State Examination (MMSE) is a 30-item clinician-administered tool assessing orientation, registration, attention/calculation, recall, language, and visuospatial function. A score of <24/30 is the standard cut-off suggesting possible cognitive impairment (though 23–26 is a grey zone; full diagnostic evaluation requires clinical judgement). It takes 7–10 minutes to administer. Important caveat: MMSE scores are affected by education level — illiterate elderly may score low on the MMSE purely due to literacy barriers, not cognitive impairment. Educational correction or literacy-adapted tools are essential in India.
Mood — Geriatric Depression Scale (GDS): The original GDS is a 30-item self-report questionnaire with yes/no answers. The GDS-15 (short form) — 15 items — is more practical in primary care settings, with a cut-off of ≥6 suggesting possible depression (sensitivity ~80–90%, specificity ~70–75%). It is validated in Indian languages. Unlike the PHQ-9, the GDS avoids somatic items that overlap with medical illness symptoms in the elderly — making it more specific for this population.
Fall risk — Timed Up and Go (TUG) test: The patient rises from a standard chair, walks 3 metres, turns, walks back, and sits down. Time ≥12 seconds identifies elderly at elevated fall risk; ≥20 seconds indicates high fall risk requiring targeted intervention. It requires no equipment and takes 2 minutes.
Nutritional status — Mini Nutritional Assessment (MNA): An 18-item tool assessing weight loss, mobility, acute illness, neuropsychological problems, BMI/calf circumference, dietary intake, and self-assessment. Scores <17 indicate malnutrition; 17–23.5 indicates risk of malnutrition. An MNA-SF (short form) allows screening in under 3 minutes.
Provided image
| Tool | Domain | Items | Administration Time | Key Cut-off | Setting |
|---|---|---|---|---|---|
| Katz ADL Index | Basic self-care function | 6 | 5 min | Dependence on ≥1 item = impairment | All levels |
| Lawton-Brody IADL | Complex daily activities | 8 | 5 min | Any item impairment = early decline | PHC, community |
| MMSE | Cognitive function | 30 | 7–10 min | <24/30 = possible impairment | PHC, district |
| GDS-15 | Depression (mood) | 15 | 5–7 min | ≥6 = possible depression | All levels |
| Timed Up and Go | Fall risk / mobility | Performance | 2 min | ≥12 sec = elevated risk | PHC, community |
| MNA-SF | Nutritional status | 6 | 3 min | <11 = at risk of malnutrition | PHC, district |
Applying Needs Identification at Community and PHC Level
The practical application of early identification begins with recognising that most elderly individuals in India will not self-present with a complaint of 'I am at risk of functional decline.' They present with specific symptoms or not at all. The skill lies in building systematic identification into every contact — not as an add-on, but as a standard part of the interaction with elderly patients.
At the community level (ASHA/ANM): The NPHCE Tier-1 mandate for house-to-house surveys should use a brief, validated screening bundle. A practical community-level screen includes: (i) three brief IADL questions ('Can you go to the market alone?', 'Can you manage your own medicines?', 'Can you cook your own meal?'); (ii) one depression question from GDS-15 ('Are you basically satisfied with your life?'); (iii) a memory complaint question ('Do you feel you are having more trouble with memory recently than most people your age?'); (iv) observation of gait — does the person move safely without assistance?; and (v) polypharmacy check — how many medicines are you taking daily? Any positive screen on ≥2 of these prompts referral to the PHC elderly OPD.
At the PHC level: Every elderly patient attending for any reason should receive a rapid 3-step screen: (i) GDS-15 for depression; (ii) three MMSE orientation questions ('What year is it? What month? Where are we?') as a rapid cognitive flag; and (iii) TUG test if mobility complaint. This takes under 5 minutes and identifies individuals requiring full CGA. The PHC doctor should also review the medication list at every visit — a medication list of ≥5 drugs triggers a polypharmacy review.
Red flags for urgent referral to district hospital: Any of the following warrant expedited referral from the PHC to the district geriatric unit: GDS-15 ≥10 (severe depression risk, suicidality must be asked); MMSE <20 (significant cognitive impairment); acute confusion (delirium) with an unclear cause; TUG >20 seconds in someone who has already fallen; evidence of elder abuse; weight loss >5% in 3 months with no clear cause.
Integrating elderly identification into existing village health days (VHNDs): The monthly VHND is the most consistent community touchpoint in rural India. Adding a dedicated 'elderly corner' with an ANM trained in the brief screening bundle takes 30 additional minutes per VHND and captures the elderly who will not walk to the PHC. The case of the 78-year-old widow from our opening hook — found at a community camp — is the archetype of this approach. She would have been invisible to the health system without proactive outreach.
CLINICAL PEARL
The MMSE education trap: The Mini-Mental State Examination has one major vulnerability in the Indian context — it was designed for and validated in educated, literate populations. Elderly individuals who never attended school score lower on the MMSE not because of cognitive impairment but because of literacy barriers (writing a sentence, copying a figure). An illiterate 80-year-old who independently manages her household, keeps track of her medicines, and navigates the village market without assistance is NOT cognitively impaired — but may score 14/30 on the MMSE. Always interpret MMSE scores in the context of education level. In illiterate elderly, the clock-drawing test and the IADL-based cognitive screen are more valid alternatives, or use education-adjusted MMSE norms. The same caution applies to any language-dependent test: always use the validated version in the patient's primary language.
SELF-CHECK
An ANM is conducting a house-to-house survey of elderly individuals in a village under NPHCE. She identifies a 70-year-old man who scores ≥6 on the GDS-15 short form. What is the MOST appropriate next step?
A. Start antidepressant medication immediately
B. Reassure the family that depression is normal in old age
C. Refer to the PHC elderly OPD for comprehensive assessment
D. Refer directly to the regional geriatric centre for psychiatric evaluation
Reveal Answer
Answer: C. Refer to the PHC elderly OPD for comprehensive assessment
A GDS-15 score ≥6 suggests possible depression but is a SCREENING result, not a diagnosis. The appropriate next step is referral to the PHC elderly OPD for comprehensive assessment (full clinical evaluation, MMSE, physical examination, medication review, and decision on management). Antidepressants should never be started based on a screening score alone (option A — incorrect). Reassuring that depression is 'normal' is incorrect and harmful — depression in the elderly is a disease, not a normal ageing change, and it is treatable (option B — incorrect). Direct referral to a regional centre bypasses the PHC (option D) — this would only be appropriate if the PHC assessment reveals severe or complex cases.