Page 2 of 16
CM16.1-2 | CM16.1-2 | Health Planning Concepts and Planning Cycle — SDL Guide (Part 2)
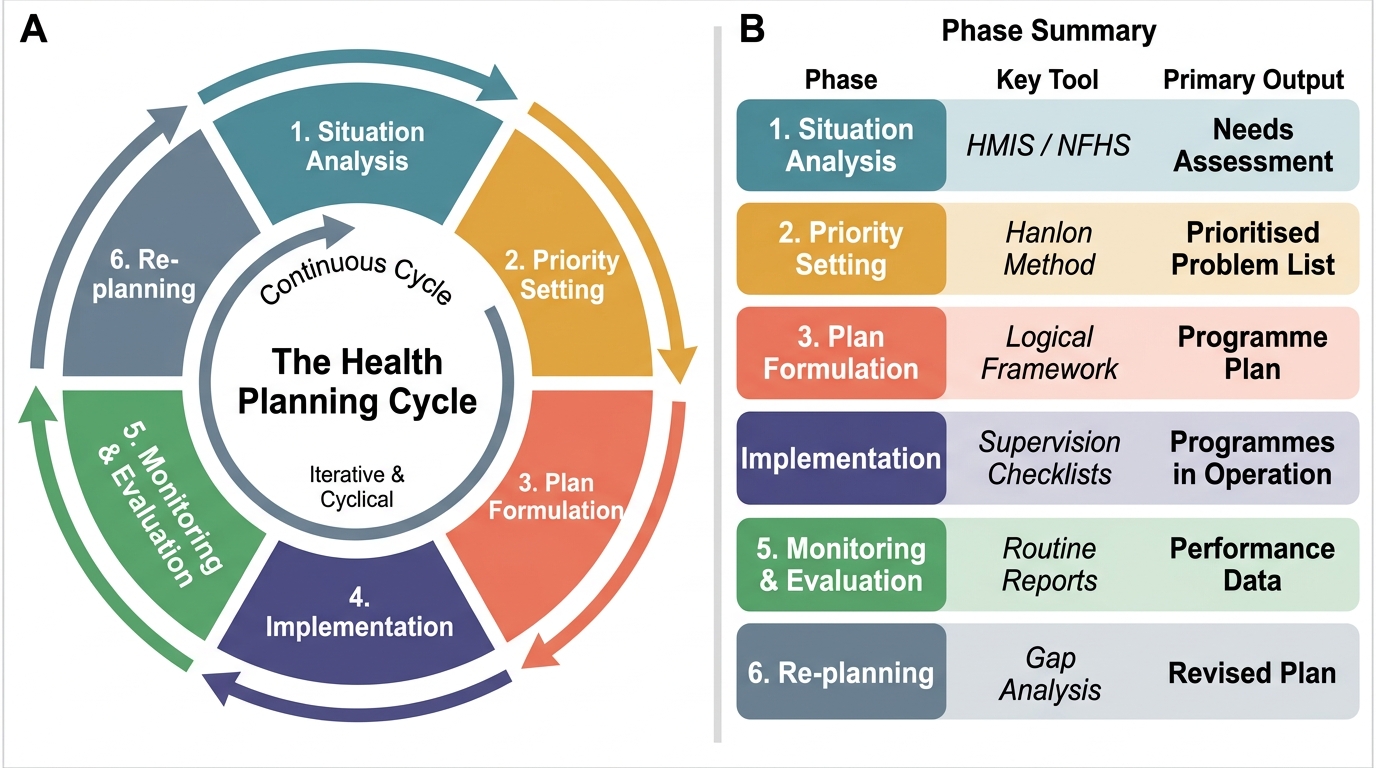
The Health Planning Cycle: Six Phases
The planning cycle is the operational tool through which the concepts of health planning are translated into programmes. It is a six-phase, iterative process — completing one cycle feeds data back into the next, producing continuous improvement. Calling it a 'cycle' (rather than a 'sequence') is deliberate: health planning is never finished; it is perpetually renewed as epidemiological realities shift and programme learning accumulates.
The six phases are as follows:
Phase 1 — Situation Analysis (Needs Assessment): The planner characterises the current health situation: What is the disease burden? Who is affected and where? What resources (staff, facilities, funds, community assets) currently exist? What are the gaps between IPHS norms and actual provision? Tools include: HMIS data, NFHS/DLHS survey data, facility surveys, community needs assessments, rapid appraisals. Output: a situation analysis document that quantifies needs and identifies priority problems.
Phase 2 — Priority Setting: Not all identified problems can be addressed simultaneously. Criteria for prioritisation include: magnitude of the problem (number affected), severity (case fatality, years of life lost), feasibility of intervention (available technology, cost-effectiveness), and community concern. Tools include: criteria-based scoring matrices, the Hanlon method (for quantitative scoring of health problems), the BPRS (Basic Priority Rating System). Output: a ranked priority list of health problems for the planning period.
Phase 3 — Plan Formulation: For each priority problem, the planner defines: (a) long-term goals (e.g., reduce under-5 mortality by 30% in 5 years); (b) short-term objectives — SMART (Specific, Measurable, Achievable, Relevant, Time-bound); (c) strategies (the broad approach — e.g., scale up integrated management of childhood illness); (d) activities (specific actions — e.g., train 500 ASHAs in IMNCI by Q3); (e) inputs (budget, staff, drugs); (f) responsible entities and timelines. Output: a programme implementation plan (PIP) or annual plan of action.
Phase 4 — Implementation: Operationalising the plan — deploying staff, procuring drugs, training health workers, running outreach camps, and managing the supply chain. The key management function here is coordination: across departments (health, ICDS, education), across levels (state → district → block → village), and across implementing agencies (government, NGOs, private sector). The Gantt chart is a commonly used tool for tracking activity timelines.
Phase 5 — Monitoring and Evaluation: Monitoring is the continuous process of tracking programme inputs, activities, and outputs against the plan (e.g., monthly HMIS reports on immunisation coverage). Evaluation is the periodic assessment of whether outcomes and impact targets are being achieved (e.g., a mid-term evaluation of NHM after 3 years). Together, M&E generate the evidence base for the next phase.
Phase 6 — Re-planning: Based on M&E findings, the plan is revised — priorities re-assessed, strategies modified, resource allocations shifted. This closes the loop, converting what might otherwise be a linear sequence into a genuine cycle.
The Health Planning Cycle — Six Iterative Phases
| Phase | Key Activities | Key Tools | Primary Output |
|---|---|---|---|
| 1. Situation Analysis | Assess disease burden, resources, gaps | HMIS, NFHS, DLHS, facility surveys | Needs assessment document |
| 2. Priority Setting | Rank problems by magnitude, severity, feasibility | Hanlon method, BPRS, scoring matrices | Prioritised problem list |
| 3. Plan Formulation | Define goals, objectives, strategies, activities, budget | SMART criteria, logical framework, Gantt chart | Programme Implementation Plan |
| 4. Implementation | Deploy resources, coordinate stakeholders, run activities | Supervision checklists, supply chain tools | Programmes in operation |
| 5. Monitoring & Evaluation | Track outputs; assess outcomes and impact | HMIS dashboards, survey data, process evaluations | M&E report with recommendations |
| 6. Re-planning | Revise plan based on evidence | Stakeholder review meetings, updated situation analysis | Revised/new plan |
SELF-CHECK
A district health officer observes that monthly HMIS reports show immunisation coverage at 78%, but the annual evaluation finds actual full immunisation coverage is only 62% (corrected by household survey). Which phase of the planning cycle does the household-survey-based evaluation belong to, and what is the most appropriate next step?
A. Phase 3 (Plan Formulation); the officer should revise the programme implementation plan
B. Phase 5 (Monitoring and Evaluation); the officer should document the gap and use it to inform re-planning
C. Phase 2 (Priority Setting); the officer should move immunisation up the priority list
D. Phase 4 (Implementation); the officer should immediately hire more vaccinators
Reveal Answer
Answer: B. Phase 5 (Monitoring and Evaluation); the officer should document the gap and use it to inform re-planning
A household survey assessing actual full immunisation coverage is an evaluative activity — it measures the outcome of the immunisation programme, going beyond the routine HMIS tracking of inputs/outputs. This belongs to Phase 5 (Monitoring and Evaluation). The HMIS figure of 78% reflects reported outputs (doses given), while the survey-based 62% reflects true coverage at the population level — a critical discrepancy that exposes HMIS data quality issues and/or dropout rates. The documented gap then drives Phase 6 (re-planning): strategy revision (e.g., focus on second-dose defaulter tracking, community outreach, HMIS data quality improvement). Jumping to Phase 4 (hiring vaccinators) without evaluating why coverage is low would be premature and likely ineffective.
Monitoring and Evaluation in the Planning Cycle
Monitoring and evaluation (M&E) deserves its own treatment because it is the feedback mechanism that converts a static plan into a learning system. Without rigorous M&E, planners have no way of knowing whether their interventions are working, whether resources are being used as intended, or whether the epidemiological situation has shifted in ways that render the original plan obsolete.
Monitoring is the routine, continuous process of tracking programme implementation. It answers: Is the programme being implemented as planned? Are inputs arriving on time (drugs, staff, funds)? Are activities happening at the expected scale (outreach camps conducted, ASHAs trained)? Are the intended outputs being generated (immunisations delivered, ante-natal care visits conducted)? The primary data source for monitoring in India's health system is the HMIS (Health Management Information System), which aggregates facility-reported data monthly. Limitations of HMIS include: incomplete reporting from private facilities, data-entry errors, and an inability to capture demand-side barriers (why patients did not come). The MCTS/RCH portal (Mother and Child Tracking System) adds individual-level tracking for ante-natal and immunisation services.
Evaluation is the periodic, systematic assessment of a programme's achievement of its stated objectives and its broader impact on health outcomes. It answers: Did the programme achieve its targets? Did it improve health outcomes? Was it efficient? Was it equitable? Evaluation types include:
- Process evaluation — was the programme implemented as designed?
- Outcome evaluation — were the immediate health outcomes (e.g., coverage rates) achieved?
- Impact evaluation — did the programme change the underlying health status (e.g., reduced mortality)?
- Efficiency evaluation — was the outcome achieved at an acceptable cost?
Key data sources for evaluation in India:
- NFHS (National Family Health Survey): Household survey conducted approximately every 4-5 years; provides nationally representative data on coverage indicators (immunisation, ante-natal care, institutional delivery), nutritional status, and demographic indicators. NFHS-5 (2019-21) is the most recent.
- DLHS (District Level Household Survey): More granular, district-level data; less frequent than NFHS.
- Annual Health Survey (AHS): Covers high-focus states with high disease burden; annually updated.
- CES (Coverage Evaluation Survey): Specific to immunisation programme evaluation.
- Verbal Autopsy and MCCD data: For cause-of-death attribution at district level.
The key distinction between monitoring and evaluation is frequency and purpose: monitoring is continuous and operational (tracks fidelity to the plan); evaluation is periodic and strategic (assesses whether the plan was worth doing and how to improve the next one). Both feed into the re-planning phase — monitoring identifies implementation problems in real time, while evaluation informs structural revisions to strategy.
Applying the Planning Cycle: India's NHM as a Case Study
The National Health Mission (NHM), launched in 2013 (building on the National Rural Health Mission established in 2005), is India's largest public health programme and one of the most consequential applications of the planning cycle in the country's history. Examining NHM through the planning cycle lens illustrates how each phase functions in practice at national scale.
Phase 1 — Situation Analysis: The NRHM's founding was preceded by a major situational diagnosis — the Bulletin of Rural Health Statistics, NFHS-2 and DLHS data revealed dramatic gaps in rural health infrastructure: 8% of PHCs functioning without any doctor, 39% without adequate drug supply, infant mortality rates above 70 per 1,000 live births in the EAG (Empowered Action Group) states (Bihar, UP, Rajasthan, MP, Odisha, Jharkhand, Uttarakhand, Chhattisgarh). The situation analysis defined both the geographic and programmatic priorities.
Phase 2 — Priority Setting: NHM prioritised: (a) the eight EAG states and the north-eastern states, (b) maternal and child health, (c) communicable disease control, and (d) infrastructure upgrading to IPHS norms. The RCH (Reproductive and Child Health) and Disease Control programme components reflect this prioritisation.
Phase 3 — Plan Formulation: NHM used a State Programme Implementation Plan (SPIP) mechanism — each state submits its SPIP to the national NHM Mission Steering Group for approval and funding. SPIPs include state-specific targets, strategies, activity calendars, and budgets. The introduction of the ASHA (Accredited Social Health Activist) — one per 1,000 rural population — was the central strategy innovation: a community-based health worker trained to bridge the household-health system gap.
Phase 4 — Implementation: Implemented through a decentralised structure: a National Mission Director → State Health Societies → District Health Societies → Block-level programme managers. The untied funds mechanism (a fixed annual grant to sub-centres, PHCs, and CHCs for locally-determined needs) was a notable implementation innovation that gave front-line facilities planning autonomy within the national framework.
Phase 5 — Monitoring and Evaluation: NHM monitoring uses HMIS (consolidated at national level), MCTS, and periodic programme evaluations. The NHM Common Review Mission (CRM) — annual joint government-partner field visits to sampled states — is a structured evaluation mechanism. External evaluations (by IIPS, NHSRC, and independent researchers) feed into the national picture. NFHS-4 (2015-16) provided the major mid-term impact assessment.
Phase 6 — Re-planning: NHM has undergone multiple re-planning cycles: the 2012 extension revised targets based on DLHS-3 findings; the launch of NHM 2.0 (2017-2020) integrated NUHM (urban) more fully and responded to the emerging NCD burden; the Ayushman Bharat transformation (2018) — adding Health and Wellness Centres (1.5 lakh target) and PM-JAY (the PM's Jan Arogya Yojana, providing Rs. 5 lakh/year health cover to 50 crore people from the poorest 40% of the population) — represents the largest single re-planning adjustment, responding to evidence that primary care infrastructure and financial protection were the two biggest remaining gaps.
NHM's trajectory — from the initial NRHM design in 2005 to the Ayushman Bharat architecture of 2018-present — is a real-world demonstration of the planning cycle in action: iterative, evidence-driven, and responsive to evolving needs and capabilities.
SELF-CHECK
Which of the following accurately describes the role of ASHA workers within the National Health Mission's planning framework?
A. ASHAs were introduced in Phase 1 (situation analysis) to collect district-level health data
B. ASHAs are a Phase 3 (plan formulation) strategy innovation — community-based workers to bridge the household-health system gap
C. ASHAs function primarily in Phase 5 (monitoring) by submitting monthly HMIS data
D. ASHAs were added in Phase 6 (re-planning) after mid-term evaluation showed poor immunisation coverage
Reveal Answer
Answer: B. ASHAs are a Phase 3 (plan formulation) strategy innovation — community-based workers to bridge the household-health system gap
The ASHA (Accredited Social Health Activist) was the central strategy innovation at the plan formulation phase of the NRHM/NHM. ASHAs are community health workers — 1 per 1,000 rural population — trained to facilitate access to health services (accompanying women to institutional deliveries, mobilising immunisation, promoting WASH practices) and to serve as a demand-side bridge between the community and the formal health system. While ASHAs do collect and report some data that feeds into monitoring, their core design role is as a strategy to address the identified situation-analysis finding that rural communities lacked a trusted community-level health interface.
CLINICAL PEARL
The planning cycle is not chronological — it is concurrent. In a district health office, Phase 5 (M&E of the current year's plan) and Phase 6 (re-planning for the next year) are occurring simultaneously. The SPIP for the next financial year is being drafted by October-November while the current year's implementation is still ongoing and being monitored. Understanding this overlap is critical: a medical officer who waits for 'evaluation' to finish before 'planning' begins will always be planning last year's response to last year's problem. Proactive planners use real-time HMIS data to make mid-cycle corrections while simultaneously feeding the same data into next-year's situation analysis.