Page 9 of 16
CM16.4-5 | CM16.4-5 | Health Policy, Planning and Economics in India — SDL Guide (Part 2)
From Five-Year Plans to NITI Aayog: India's Health Planning Architecture
India's national health planning does not occur in a policy vacuum — it is embedded in a national planning architecture that has itself evolved significantly. Understanding this architecture is essential for situating health policies within the government's broader resource allocation framework.
From 1951 to 2014, India's national development planning was conducted through Five-Year Plans by the Planning Commission of India (established 1950). The Five-Year Plans allocated central government resources across all sectors including health. Each plan set health-sector targets (e.g., the 9th Plan: health infrastructure expansion, 10th Plan: NRHM-like health system strengthening, 11th Plan: NRHM full implementation) and allocated funds accordingly. The Planning Commission operated in a top-down model: central allocation → state implementation, with states submitting their Annual Plans to the commission for funding approval.
A critical feature of the Five-Year Plan era was the distinction between Plan expenditure (new programmes and capital investments, allocated through the planning process) and Non-Plan expenditure (salaries, maintenance of existing facilities — allocated through the budget). Health departments chronically under-invested in Non-Plan expenditure — salaries and maintenance — while Plan allocations were used for visible capital spending (new buildings, equipment). The result: new sub-centres with no staff, new equipment with no maintenance budget. This structural flaw was a systemic management failure baked into the planning architecture itself.
In 2015, the Planning Commission was abolished and replaced by the NITI Aayog (National Institution for Transforming India). This represented a fundamental shift: NITI Aayog is a think-tank and policy advisory body, NOT a resource-allocating body. It does not control the budget. Resource allocation for health is now entirely through the Ministry of Finance (via the Union Budget) and the Ministry of Health and Family Welfare (through the Centrally Sponsored Scheme framework of NHM, Ayushman Bharat, and national disease control programmes). NITI Aayog produces long-range strategy documents — the 7-year Strategy for New India (2018-2023) and the 15-year Vision for India (2019-2034) — that set health sector targets and recommendations but do not bind budget allocations.
The abolition of the Plan/Non-Plan budget distinction (implemented in 2017-18) was a direct attempt to fix the structural flaw described above — all government spending is now in a single budget framework, theoretically allowing health departments to allocate rationally between capital and recurrent spending without the Plan/Non-Plan straitjacket.
SELF-CHECK
India's Planning Commission was abolished in 2015 and replaced by NITI Aayog. What is the MOST significant functional difference between the two institutions?
A. NITI Aayog has broader sectoral coverage than the Planning Commission, including defence and foreign policy
B. The Planning Commission allocated resources through Five-Year Plans; NITI Aayog is a policy advisory think-tank without resource allocation authority — budget allocation is now entirely through the Finance Ministry and sector ministries
C. NITI Aayog operates on a 10-year planning horizon while the Planning Commission used 5-year cycles
D. NITI Aayog directly manages state health societies, replacing the decentralised NHM model
Reveal Answer
Answer: B. The Planning Commission allocated resources through Five-Year Plans; NITI Aayog is a policy advisory think-tank without resource allocation authority — budget allocation is now entirely through the Finance Ministry and sector ministries
The fundamental difference is in resource allocation authority. The Planning Commission directly allocated central government development expenditure to states and sectors through the Five-Year Plan mechanism — it controlled a significant portion of the national investment budget. NITI Aayog has no such authority; it is an advisory and research body that produces strategy documents and recommendations but does not allocate funds. Budget decisions now rest entirely with the Ministry of Finance (Union Budget) and the sector-specific ministries (like MoHFW for health). This shift means national health planning no longer has a single point of resource authority — it must be negotiated through the budget process and Centrally Sponsored Scheme frameworks annually.
Health Economics Concepts: Financing, Expenditure, and Economic Burden
Health economics applies economic tools to health sector decisions — allocation, financing, efficiency, and equity. For a medical student, the most practically relevant concepts are: sources of health financing, categories of health expenditure, the economic burden of disease, and the distinction between efficiency and equity in health systems. These concepts provide the analytical vocabulary for reading and interpreting health policy.
Sources of health financing — where does the money for health come from? — are conventionally categorised as follows in the National Health Accounts (NHA) framework:
- Government sources: Tax-financed government expenditure through the Union and state budgets (the 'public' component); this is the primary source in most health systems with universal coverage aspirations.
- Social health insurance: Contributions from employers and employees to mandated insurance schemes; in India, the major formal-sector social insurance schemes are ESIC (Employees' State Insurance Corporation, covering formal-sector employees) and CGHS (Central Government Health Scheme, covering central government employees and their families).
- Private insurance: Voluntary commercial insurance, covering approximately 5-6% of Indians (predominantly urban, salaried, and higher-income).
- Out-of-pocket expenditure (OOP): Payments made directly by households at the point of care — the dominant and most inequitable source. India's NHA 2019-20 reports OOP at approximately 48% of total health expenditure (improved from approximately 70% in 2004-05, but still far from the NHP 2017 target of 25%).
- External/donor funding: Contributions from bilateral donors (USAID, DFID/FCDO), multilateral agencies (World Bank, Global Fund, GAVI), and international NGOs; relevant for disease-specific programmes (HIV, TB, malaria).
The economic burden of disease has two components:
- Direct costs: Medical costs (outpatient fees, hospitalisation, drugs, diagnostics, transport to facility).
- Indirect costs: Productivity losses due to illness-related absenteeism, premature mortality, or disability — often measured using human capital or friction-cost approaches. The indirect burden is frequently the larger component for working-age adults; TB, for example, imposes substantial indirect costs through prolonged treatment and work incapacity.
Catastrophic health expenditure (CHE) is defined as health payments exceeding a threshold of household consumption — typically 10% of total household consumption or 25% of non-food consumption. CHE is an equity indicator: it captures the proportion of households pushed into poverty or near-poverty by health spending.
The distinction between efficiency and equity in health systems is fundamental to policy analysis. Efficiency asks: are we getting maximum health output from available inputs? (Technical efficiency = same output with fewer inputs; allocative efficiency = inputs directed to their highest-value uses.) Equity asks: is health care accessible and affordable for all, regardless of income, geography, or social position? Health systems can be efficient in aggregate while being deeply inequitable — a private sector that serves the wealthy efficiently while the poor have no access is efficient but not equitable. NHP 2017's OOP reduction target and PM-JAY's targeting of the poorest 40% are explicit equity interventions.
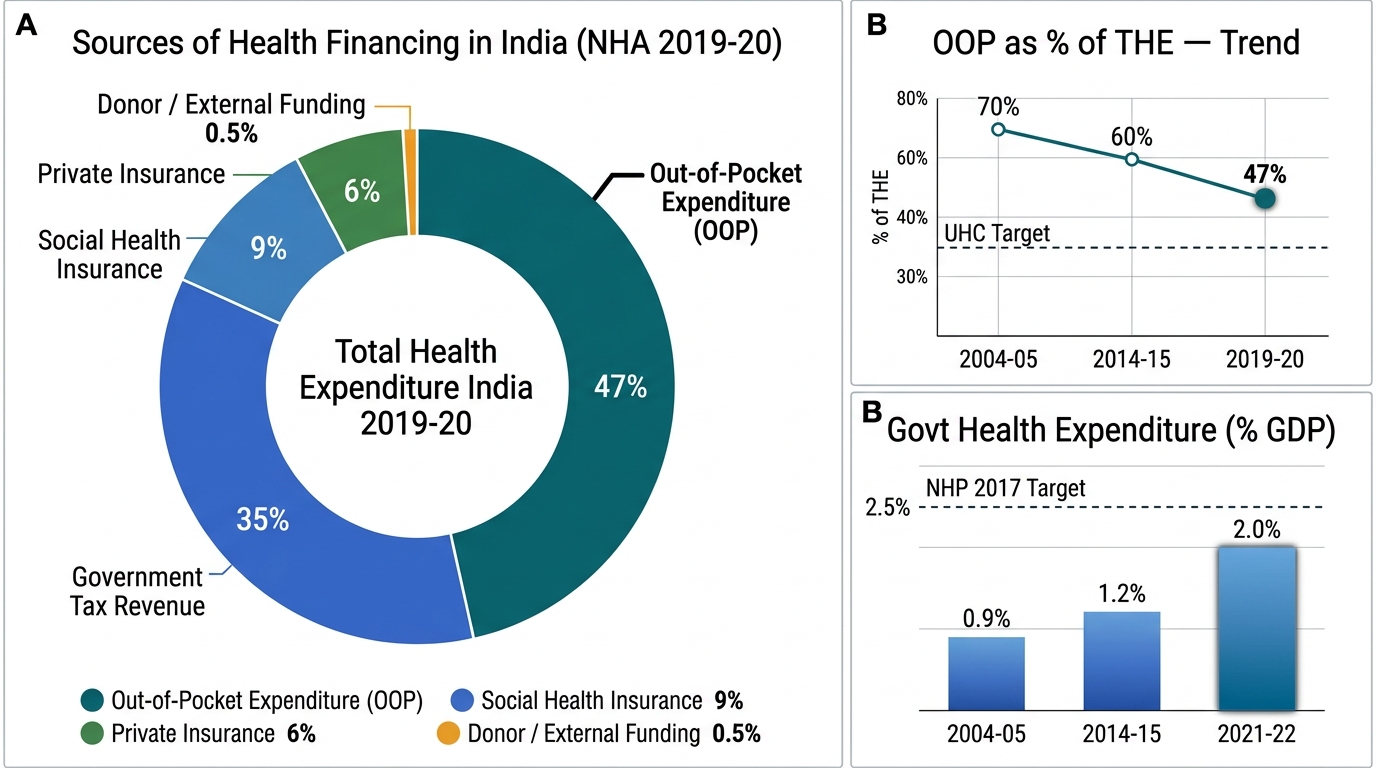
Sources of Health Financing in India — National Health Accounts 2019-20
Evaluating India's Health Financing Performance and Efficiency
Evaluating a health system's financing performance requires comparing actual expenditure patterns against policy targets and international benchmarks. For India, this evaluation reveals both significant progress and persistent gaps — providing a realistic basis for policy advocacy.
Government health expenditure as % of GDP is the headline financing indicator. India's trajectory: approximately 0.9% in 2004-05 → approximately 1.15-1.2% in 2014-15 → approximately 1.9-2.1% in 2021-22 (the COVID-19 pandemic year saw a temporary increase). The NHP 2017 target of 2.5% by 2025 has not yet been met. By comparison, global WHO data: OECD countries average approximately 7-9% of GDP on health (mostly public); even lower-middle-income countries in South-East Asia average approximately 2.5-3%. India's public health expenditure remains structurally low, constraining the government's ability to deliver on UHC commitments without continued reliance on OOP.
OOP expenditure is the equity indicator. National Health Accounts data shows: OOP as a share of total health expenditure fell from approximately 70% (2004-05) to approximately 48% (2019-20) — meaningful progress, but still twice the NHP 2017 target of 25%. The absolute level of OOP has increased (more spending on health overall) even as the share has fallen, meaning households are still spending more on health in real terms. The improvement is partly attributable to the expansion of government programmes (NHM, state-level drug free schemes, Ayushman Bharat) but also partly to the growth of the private insurance market.
Health system efficiency can be evaluated at multiple levels. Allocative efficiency — are resources directed to the highest-burden problems? — India shows mixed performance: TB and child health (high burden, evidence-based interventions) receive disproportionate government attention; NCDs (now the leading cause of mortality) remain under-resourced relative to burden. Technical efficiency — are the same health outcomes being produced at minimum cost? — India's disease-specific programme evaluations (RNTCP, immunisation, malaria) show relatively good technical efficiency for vertical programmes, but integrated primary care delivery at PHC and CHC level shows high inefficiency due to staffing gaps, stock-outs, and suboptimal management.
The health financing transition — moving from predominantly OOP to predominantly government and insurance financing — is the central structural challenge of India's health economics policy. This transition requires simultaneous increases in: (1) public expenditure (taxes → government budget → health allocation); (2) social insurance coverage (particularly for the informal sector, which is excluded from ESIC and CGHS); and (3) efficient use of PM-JAY and state insurance schemes to convert entitlement into actual access.