Page 5 of 14
CM17.3-4 | CM17.3-4 | Primary Health Care and Health Policies — SDL Guide (Part 2)
National Health Policies — NHP 2017, NPP 2000, and MDG/SDG Commitments
India's national health policies translate PHC principles into measurable commitments. Understanding three policy generations is essential:
National Population Policy 2000 (NPP 2000): The NPP 2000 addressed India's population and reproductive health agenda, setting immediate, medium-term, and long-term targets:
- Immediate: provide integrated package of services for child survival, maternal health, and contraception
- Medium-term (by 2010): IMR ≤30/1,000 live births; MMR ≤100/100,000 live births; Total Fertility Rate (TFR) 2.1 (replacement level); Universal immunisation of children
- Long-term (by 2045): achieve stable population consistent with sustainable development
Millennium Development Goals (MDGs, 2000–2015): India committed to 8 MDGs; the health-relevant ones include:
- MDG 4: Reduce under-5 mortality rate (U5MR) by two-thirds between 1990 and 2015 (India's 1990 U5MR ~126/1,000; 2015 target ~42)
- MDG 5: Reduce maternal mortality ratio (MMR) by three-quarters between 1990 and 2015 (India's 1990 MMR ~556/100,000; 2015 target ~139)
- MDG 6: Halt and begin to reverse the spread of HIV/AIDS and malaria
- India made substantial progress on MDG 4 and 6 but did not fully achieve MDG 5.
National Health Policy 2017 (NHP 2017): India's most comprehensive health policy, framed around the SDG health goals. Key NHP 2017 targets by 2025:
- IMR ≤28/1,000 live births; U5MR ≤23/1,000; MMR ≤100/100,000
- TFR 2.1 nationally
- Health expenditure increased to 2.5% of GDP (from ~1.15% in 2017)
- Life expectancy at birth ≥70 years
- Progressive achievement of Universal Health Coverage (UHC)
Sustainable Development Goals (SDGs, 2015–2030): SDG 3 is 'Good Health and Well-Being'; specific targets:
- SDG 3.1: MMR <70/100,000 live births by 2030
- SDG 3.2: U5MR ≤25/1,000 by 2030; Neonatal Mortality Rate ≤12/1,000 by 2030
- SDG 3.8: Achieve Universal Health Coverage
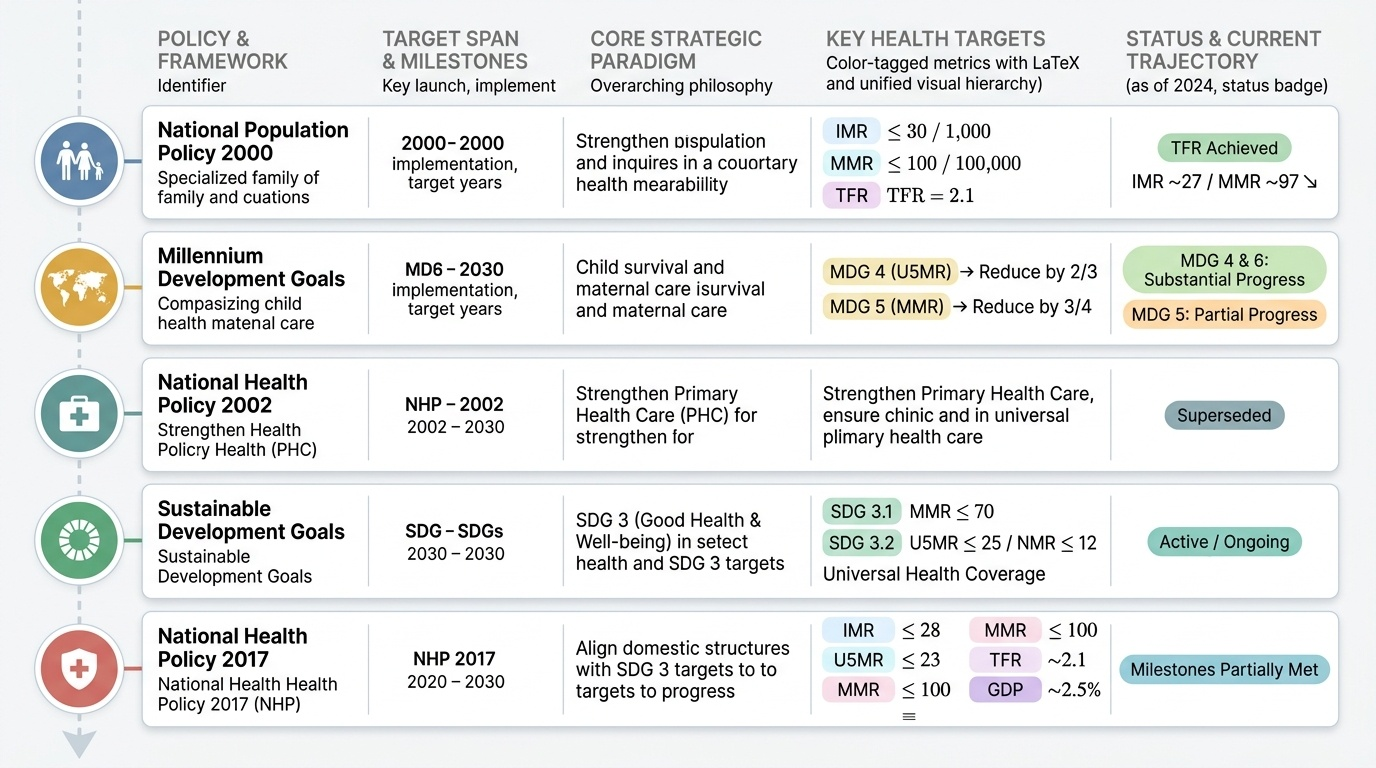
Provided image
| Policy / Framework | Year | Key Health Targets | Status (2024) |
|---|---|---|---|
| National Population Policy | 2000 | IMR ≤30, MMR ≤100, TFR 2.1 by 2010 | TFR achieved; IMR ~27 (near); MMR ~97 (near) |
| National Health Policy | 2002 | Reinforce PHC, eliminate polio/leprosy | Largely achieved |
| Millennium Dev. Goals | 2000–2015 | U5MR ↓2/3, MMR ↓3/4 | MDG 4 nearly achieved; MDG 5 partially |
| National Health Policy | 2017 | IMR ≤28, U5MR ≤23, MMR ≤100, GDP 2.5% | In progress |
| Sustainable Dev. Goals | 2015–2030 | MMR <70, U5MR ≤25, NMR ≤12, UHC | In progress |
SELF-CHECK
The Millennium Development Goal 5 (MDG 5) required India to reduce its Maternal Mortality Ratio (MMR) by what fraction between 1990 and 2015?
A. One-half (50%)
B. Two-thirds (67%)
C. Three-quarters (75%)
D. Four-fifths (80%)
Reveal Answer
Answer: C. Three-quarters (75%)
MDG 5 required countries to reduce the MMR by three-quarters (75%) between 1990 and 2015. India's MMR in 1990 was approximately 556 per 100,000 live births; the MDG target was therefore approximately 139 per 100,000. India's MMR at the MDG deadline was approximately 174 per 100,000 — significant progress but short of the MDG 5 target. (Compare with MDG 4 which required a two-thirds reduction in U5MR — a different fraction; confusing the two is a common exam error.)
Monitoring and Evaluating PHC Programmes — Indicators and India's Progress
PHC programmes are monitored using a set of standardised health indicators that reflect the 8 elements and the outcomes they are intended to achieve. Understanding which indicator measures which PHC element allows a medical officer to rapidly identify programme gaps.
Core PHC monitoring indicators for India:
| Indicator | Reflects PHC Element | India Value (NFHS-5 / SRS 2020) | SDG Target 2030 |
|---|---|---|---|
| IMR (deaths <1 yr/1,000 LB) | MCH + immunisation + safe water | 35.2 (SRS 2020) | ≤12 |
| U5MR (deaths <5 yr/1,000 LB) | MCH + nutrition + sanitation | 41.9 (SRS 2019) | ≤25 |
| NMR (neonatal deaths/1,000 LB) | MCH + skilled birth attendance | 25.5 (SRS 2019) | ≤12 |
| MMR (maternal deaths/100,000 LB) | MCH + skilled birth attendance | 97 (SRS 2018-20) | <70 |
| TFR (births/woman) | Family planning | 2.0 (NFHS-5) | 2.1 (replacement) |
| Full immunisation coverage | Immunisation element | 76.4% (NFHS-5) | 90% |
| Open defecation free status | Sanitation element | ODF declared 2019 (Swachh Bharat) | ODF |
| Stunting (<5 yrs) | Nutritional promotion | 35.5% (NFHS-5) | <10% |
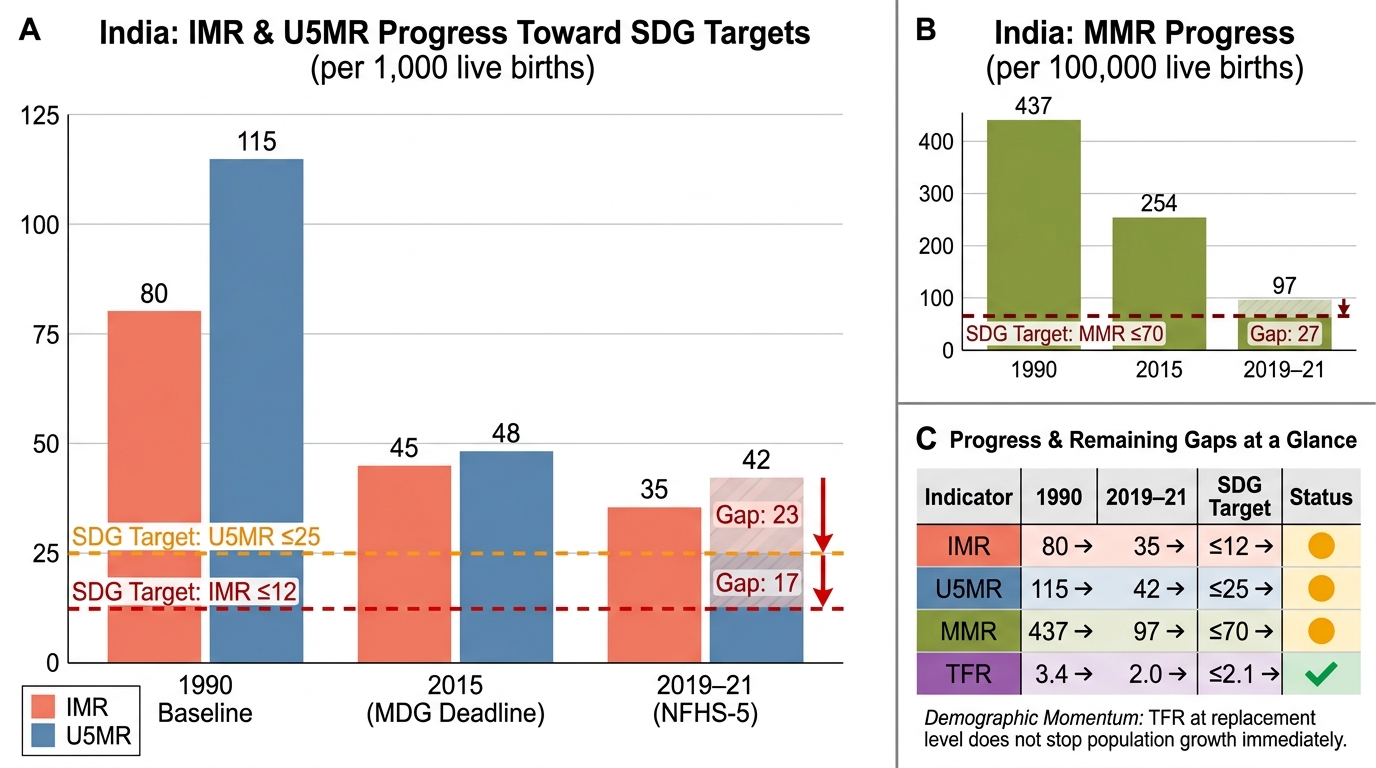
India's Reproductive and Child Health Indicators: Progress and Remaining SDG Gaps (1990–2021)
Interpreting the data: India's TFR has reached replacement level (2.0 per NFHS-5), a historic demographic milestone. IMR has declined dramatically from ~80/1,000 in 1990 to ~35/1,000 but remains above the SDG target of ≤12. Stunting at 35.5% remains a major nutritional public health challenge despite ICDS and POSHAN Abhiyaan. These gaps define the current PHC agenda for India.
Process vs outcome indicators: In programme monitoring, process indicators (immunisation coverage, ANC registration rates, skilled birth attendance %) measure what the health system is doing; outcome indicators (IMR, MMR, TFR) measure what results the system is achieving. Both are needed: high process indicator values with poor outcomes signal quality issues; low process values immediately identify coverage gaps.
CLINICAL PEARL
Pearl: TFR reaching replacement level does not mean the population stops growing immediately. India's TFR of 2.0 (NFHS-5) is at or below replacement level — yet India's population will continue to grow for several decades due to demographic momentum: the large cohort of young people already born will pass through their reproductive years, generating births even at below-replacement fertility. This is why NPP 2000's long-term target extends to 2045 for population stabilisation. Exam questions often conflate 'TFR at replacement level' with 'population stable' — they are different: TFR is the rate of fertility now; population stabilisation depends on the age structure inherited from past high fertility.
Applying PHC Principles to a District Health Scenario
Integrating PHC principles and national policy targets in a real-world scenario requires mapping observed gaps to their Alma-Ata element and the appropriate policy lever.
Scenario: You are the District Health Officer (DHO) of a district in Uttar Pradesh with the following profile (annual HMIS data): IMR = 48/1,000 (state average 43, national 35); full immunisation coverage = 52% (national target 90%); institutional delivery = 61% (national average 89%); open defecation = 22% of households; anaemia in women of reproductive age = 58%; TFR = 3.1.
PHC gap analysis:
| Observed Gap | PHC Element | Policy Lever | Responsible Actor |
|---|---|---|---|
| Immunisation coverage 52% | Immunisation | UIP/Mission Indradhanush | CMHO, ANMs, ASHAs |
| Institutional delivery 61% | MCH | JSY/PMSMA/SUMAN | PHC/CHC medical officers, ANMs |
| High TFR 3.1 | Family planning | NPP 2000/Mission Parivar Vikas | ASHA counselling, spacing methods |
| High anaemia 58% | Nutritional promotion | POSHAN Abhiyaan/IFA supplementation | ICDS, ANMs |
| OD 22% households | Safe water/sanitation | Swachh Bharat Mission | PRIs, Public Health Engineering |
Application of PHC principles:
- Equitable distribution: identify the blocks with lowest immunisation and institutional delivery rates — target outreach specifically there
- Community participation: activate VHSNCs in low-performing villages; involve self-help groups in anaemia reduction
- Intersectoral coordination: convene District-level meetings with Education, PRI, ICDS and Water & Sanitation departments — anaemia and OD gaps cannot be solved by health sector alone
- Appropriate technology: iron-folic acid tablets, ORS, contraceptive spacing methods — all align with appropriate technology criteria
- Political commitment: present gap analysis at District Health Society meeting; seek budget allocation for Mission Indradhanush intensification rounds
This mapping exercise — from observed indicator gap to PHC element to policy programme to responsible actor — is the applied skill that PHC and policy literacy enable.
SELF-CHECK
A district in Bihar has full immunisation coverage of 48% — far below the national target of 90%. Under the Alma-Ata PHC framework, this gap most directly reflects failure in which element of PHC?
A. Provision of essential drugs
B. Education on health problems
C. Immunisation against major infectious diseases
D. Appropriate treatment of common diseases
Reveal Answer
Answer: C. Immunisation against major infectious diseases
The Alma-Ata Declaration identifies 'immunisation against major infectious diseases' as one of the 8 elements of PHC. A full immunisation coverage of 48% against a target of 90% is a direct failure of this PHC element. The national programme responsible for this element is the Universal Immunisation Programme (UIP), supplemented by Mission Indradhanush for catch-up immunisation of unvaccinated and partially vaccinated children. While education about immunisation (element 1) and essential drugs (element 8) are also relevant, the most direct mapping of immunisation coverage is to the immunisation element itself.