Page 7 of 14
CM17.5-6 | CM17.5-6 | Healthcare Delivery and Health System Functioning — SDL Guide
Learning Objectives
- Describe the multi-tier public healthcare delivery system in India (Sub-Centre to Medical College)
- State the population norms, staffing, and functions of each level of the healthcare delivery hierarchy
- Describe the roles and functions of ASHA, ANM, and MPW in community health delivery
- Apply the WHO six health system building blocks to the Indian health system
- Use system-level indicators to evaluate health system functioning and identify gaps
- Trace a patient through the referral pathway and identify system failure points
INSTRUCTIONS
India spends approximately 1.5% of GDP on public health — one of the lowest among comparable countries — yet serves 1.4 billion people through a network of over 1.7 lakh Sub-Centres, 26,000 Primary Health Centres, and 5,600 Community Health Centres. Understanding how this system is organised, how it is supposed to function, and where it currently falls short is the essential applied knowledge for every medical officer, public health professional, and health policy advocate. This module maps the delivery architecture and applies the global WHO framework for health system assessment to India's context.
References
- Park's Textbook of Preventive & Social Medicine, 27th ed., Ch. 29 (Health Planning and Administration in India) (textbook)
- Indian Public Health Standards (IPHS), MoHFW, Government of India, 2012 (revised) (policy)
- WHO, Everybody's Business: Strengthening Health Systems to Improve Health Outcomes, 2007 (six building blocks) (framework)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ramu, a 35-year-old farmer in a remote tribal block of Odisha, develops chest pain at 2 AM. The nearest Sub-Centre is 4 kilometres away — its ANM is off-duty overnight. The nearest PHC with a doctor is 18 kilometres away on an unpaved road. The CHC that can handle a potential myocardial infarction is 45 kilometres away, and the District Hospital with a cardiologist is 90 kilometres away — a two-hour journey on a good day. By the time Ramu reaches care, his opportunity for thrombolysis has passed. This is not an unusual story in India; it is the everyday reality for hundreds of millions of people living beyond the reach of functional primary healthcare. Understanding why this gap exists — the system architecture, the workforce shortfalls, the financing failures — is the first step toward designing solutions. That is what this module gives you.
WHY THIS MATTERS
NMC competencies CM17.5 and CM17.6 test your knowledge of healthcare delivery architecture and health system functioning in India. This knowledge is directly applied in: (1) your internship rural health posting, where you will work within the PHC/CHC hierarchy; (2) your future role as Medical Officer responsible for the catchment population served by your centre; (3) district health administration, where the MO must coordinate across tiers and sectors; and (4) examinations — health system organisation and the WHO building blocks are high-frequency NEET-PG topics. The ability to diagnose health system failures (not just patient diseases) is a competency the NMC expects at the point of MBBS graduation.
RECALL
From earlier CM modules, recall:
- PHC principles (SDL2): equitable distribution, community participation, intersectoral coordination, appropriate technology, political commitment — these principles should be visible in the design of each tier of the delivery system.
- Sub-Centre, PHC, CHC were introduced in SDL2 as India's three-tier PHC delivery structure. This module provides the full hierarchy with detailed population norms, staffing, and functions, and adds the WHO analytical framework.
- ASHA was introduced as a community link worker in SDL2 (one per 1,000 rural population). This module describes ASHA's specific functions alongside ANM and MPW.
The Burden of Healthcare Inaccessibility — India's Coverage Gaps
India's healthcare access problem has three interacting dimensions that together define the burden a functional delivery system must overcome.
Geographic inaccessibility remains severe in tribal, hilly, and remote rural areas. According to the Rural Health Statistics (MoHFW 2023), there are substantial shortfalls in Sub-Centres (12% deficit), PHCs (9% deficit), and CHCs (30% deficit) relative to population norms — with the worst deficits concentrated in the highest-need areas. Physical distances, poor road connectivity, and absence of public transport mean that even existing facilities are functionally inaccessible to many.
Financial inaccessibility — out-of-pocket expenditure is India's most significant health system failure. Out-of-pocket expenditure (OOP) constitutes approximately 47–50% of India's total health expenditure — among the highest rates in Asia. OOP is the primary driver of catastrophic health expenditure, pushing an estimated 55–60 million people below the poverty line annually due to health costs. This financial barrier is a direct consequence of underfunding: India's public health expenditure at ~1.5% of GDP (2021-22) falls far short of the NHP 2017 target of 2.5% of GDP.
Quality inaccessibility compounds geographic and financial barriers. Even when facilities exist and are reachable, many lack essential equipment, medicines, or adequately trained staff. The 30% CHC shortfall means that the specialist referral level — surgeon, physician, gynaecologist, paediatrician — is systematically absent in many districts, forcing bypassing behaviour where patients skip PHC and CHC entirely to seek district hospital or private care.
This three-dimensional burden — geographic, financial, quality — defines the system design problem. Every tier of the delivery hierarchy and every element of the WHO building blocks must be understood in relation to these access barriers.
India's Multi-Tier Public Healthcare Delivery System
India's public sector healthcare delivery is organised as a five-tier referral pyramid, from the village-level Sub-Centre at the base to tertiary Medical Colleges at the apex. Each tier has defined population norms, bed capacity, staffing standards, and functional mandates specified in the Indian Public Health Standards (IPHS).
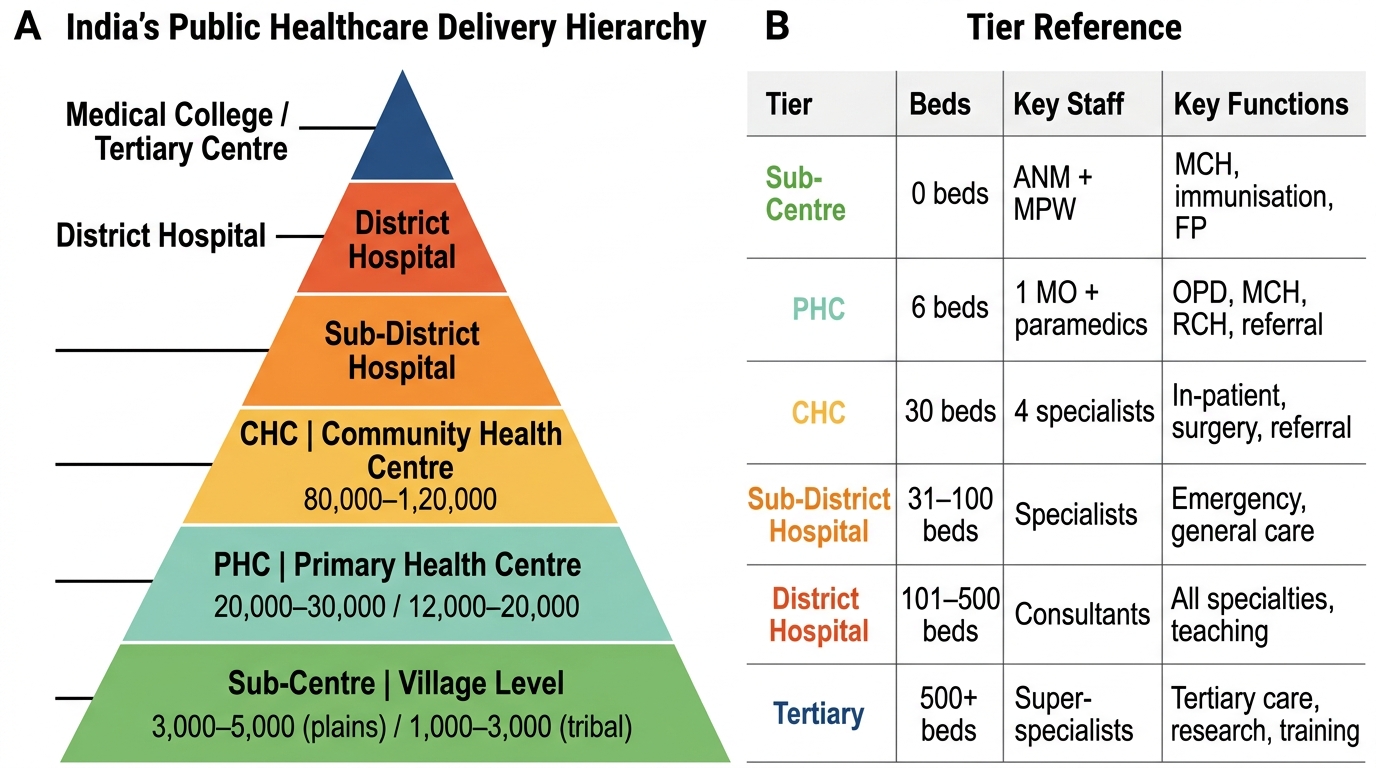
India's Public Healthcare Delivery System: Six-Tier Referral Pyramid
| Tier | Population Served (plains) | Population (tribal/hilly) | Beds | Key Staff | Key Functions |
|---|---|---|---|---|---|
| Sub-Centre | 3,000–5,000 | 1,000–3,000 | 0 (no inpatient) | ANM + MPW | MCH, immunisation, FP, basic curative |
| PHC | 20,000–30,000 | 12,000–20,000 | 6 | 1 MO + paramedics | OPD, MCH, RCH, disease control, referral |
| CHC | 80,000–1,20,000 | 40,000–60,000 | 30 | 4 specialists + MOs | Specialist OPD, surgery, delivery, 24×7 |
| Sub-District/Taluka Hospital (SDH) | 5–6 lakh | — | 31–100 | Specialists | Secondary referral, surgery, blood bank |
| District Hospital (DH) | District level | — | 75–500+ | Full specialist team | Tertiary referral, teaching (some) |
| Medical College Hospital | Regional/state | — | 500+ | Consultants + residents | Quaternary, research, postgraduate teaching |
Sub-Centre is the first contact point between the community and the health system. It is staffed by one ANM (Auxiliary Nurse Midwife) and one MPW (Male Health Worker / Multipurpose Health Worker Male), supported by ASHAs. The ANM holds monthly Village Health and Nutrition Days (VHNDs), maintains health records, administers immunisation, provides antenatal and postnatal care, and manages family planning services. Sub-Centres do not have inpatient beds.
Primary Health Centre (PHC) is led by a medical officer and provides outpatient care, a 6-bed inpatient ward for observation and delivery, laboratory services, and is the operational unit for all national health programmes (UIP, RNTCP, NVBDCP, NCD screening). The PHC serves as the first referral level for Sub-Centres.
Community Health Centre (CHC) is the first specialist-care referral point, staffed by four specialists: general surgeon, physician, obstetrician-gynaecologist, and paediatrician. The CHC has 30 beds, an operation theatre, X-ray facility, and blood storage. Under NRHM, CHCs are designated as First Referral Units (FRUs) where emergency obstetric care must be available 24×7.
Sub-District/Taluka Hospital and District Hospital provide secondary and tertiary care, surgical and specialist services, and serve as the apex of the public referral chain before Medical College hospitals.
SELF-CHECK
A Community Health Centre (CHC) in a plains district of Maharashtra is found to have no obstetrician-gynaecologist on duty for the past 3 months. Under IPHS standards, this represents a failure at which level of the referral system?
A. Sub-Centre level — the ANM should have handled obstetric emergencies
B. PHC level — the medical officer should have provided specialist-equivalent obstetric care
C. CHC level — the CHC must have four mandatory specialists including a gynaecologist to function as a First Referral Unit
D. District Hospital level — obstetric care is not mandated at CHC
Reveal Answer
Answer: C. CHC level — the CHC must have four mandatory specialists including a gynaecologist to function as a First Referral Unit
The CHC is mandated under IPHS to have four specialist cadres: general surgeon, physician, obstetrician-gynaecologist, and paediatrician. The CHC is designated as a First Referral Unit (FRU) under NRHM, specifically required to provide Comprehensive Emergency Obstetric Care (CEmOC) 24×7. Absence of the gynaecologist for 3 months means the CHC cannot function as an FRU — a critical system failure that exposes the served population of 80,000–1,20,000 people to maternal mortality risk from unmanaged obstetric emergencies.
Community Health Workers — ASHA, ANM, and MPW
India's community health worker (CHW) cadre forms the human bridge between the household and the formal health system. Three frontline cadres operate at this interface, each with a distinct role, training, and accountability structure.
ASHA (Accredited Social Health Activist) was introduced under the National Rural Health Mission (NRHM) in 2005 as a community health activist, not a medical worker. Key features:
- One ASHA per 1,000 rural population; selected from and by the village community
- Minimum 8th grade education; trained in a modular 23-day curriculum on MCH, immunisation, sanitation, disease prevention
- Incentive-based (not salaried) — paid performance incentives for specific tasks (institutional delivery facilitation, antenatal registration, TB treatment follow-up, immunisation)
- Functions: demand generation (motivating community to use services), accompaniment to facility, first aid, VHND facilitation, record-keeping
- Accountable to ANM and PHC medical officer
ANM (Auxiliary Nurse Midwife) is a government employee (not incentive-based), with formal nursing and midwifery training (18-month diploma). One ANM per Sub-Centre:
- Provides antenatal, intrapartum (for normal deliveries), and postnatal care
- Administers immunisation at Sub-Centre and through outreach
- Manages family planning services (distribution of contraceptives, IUD insertion)
- Holds monthly VHND at the village, supported by ASHAs
- Maintains health registers for the Sub-Centre catchment
- Supervisory responsibility for ASHAs in her area
MPW / Health Assistant Male (HAM) is the male counterpart at the Sub-Centre:
- Responsible for environmental sanitation, malaria surveillance, vector control
- Conducts household visits for communicable disease surveillance
- Supports disease notification and outbreak investigation
- Coordinates with Panchayati Raj Institutions on sanitation and water supply
The three cadres operate as a coordinated team: ASHA mobilises the household, ANM provides first-contact care and clinical services at the Sub-Centre, MPW manages the environmental health portfolio. This team is the operational expression of Alma-Ata's community participation principle at the ground level.