Page 18 of 32
CM5.{10,20} | CM5.{10,20} | Diet Modification for Metabolic Risk Clinics — SDL Guide
Learning Objectives
- Recommend a dietary plan for a person with type 2 diabetes mellitus, hypertension, or obesity in a simulated environment or clinical posting
- Counsel patients on diet modification for diabetic, hypertensive, and obese individuals using evidence-based dietary principles
- Apply glycaemic index concepts to select appropriate Indian staple foods for diabetic patients
- Document a structured dietary plan using ICMR-NIN 2020 RDA targets and local food availability
INSTRUCTIONS
Medical Nutrition Therapy (MNT) is a frontline intervention for Type 2 diabetes, hypertension, and obesity — often more powerful than medication at the same stage of disease. This module equips you to prescribe a specific dietary plan and counsel patients on the rationale behind each recommendation.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health; Ch. 6 — Non-Communicable Diseases (textbook)
- ICMR-NIN 2020 — Recommended Dietary Allowances for Indians (guideline)
- American Diabetes Association Standards of Medical Care in Diabetes, 2024 — Nutrition Therapy (guideline)
- WHO 2023 — Guideline: Sodium intake for adults and children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At an NCD clinic at a Community Health Centre in urban Tamil Nadu, three patients arrive in succession. The first is a 48-year-old software engineer with HbA1c 9.2%, weight 88 kg, BMI 31.2 — already on metformin. He asks: 'What should I eat? My wife says rice is bad for diabetes.' The second is a 55-year-old housewife with blood pressure 158/96 mmHg — she is worried about taking antihypertensives and asks if diet can help. The third is a 35-year-old delivery driver with BMI 34.5, central obesity, fasting glucose 108 mg/dL (prediabetes), and dyslipidaemia — not yet on medication. All three have a common denominator: diet is both the primary cause and the primary modifiable factor in their metabolic trajectory. You have 10-15 minutes per patient. This module prepares you to use that time well.
WHY THIS MATTERS
India is facing an epidemic of metabolic disease driven by dietary transition. The ICMR-India Diabetes Study 2023 estimates T2DM prevalence at 11.4% and prediabetes at 15.3% of adults — together 26.7% of the adult population, or over 250 million people. NFHS-5 records hypertension in 28.4% of adults and overweight/obesity in 24%. Dietary management is the cornerstone of primary prevention and a WHO-recommended first-line intervention for newly diagnosed T2DM and Stage-1 hypertension. CM5.10 explicitly requires prescribing a 'dietary plan' in a simulated environment — an OSCE-testable clinical skill. CM5.20 requires counselling competence for diabetic, hypertensive, and obese individuals. This is applied nutrition — where the RDA values and food knowledge from earlier modules translate into a clinical prescription.
RECALL
From cm-nutrition-requirements: recall that carbohydrates yield 4 kcal/g (AMDR 50-60%), proteins yield 4 kcal/g (RDA 0.83 g/kg/day), and fats yield 9 kcal/g (AMDR 20-30%). Recall that dietary fibre is recommended at 40 g/day (ICMR-NIN 2020) and that saturated fat should be <10% of total energy. From cm-nutrition-food-safety: recall that sodium restriction to <5 g salt/day (WHO) is the primary dietary target for hypertension. From cm-nutrition-assessment: recall the 5-step diet planning framework — assess needs → set targets → select food groups → plan meal pattern → validate. You will now apply all of this to three specific clinical conditions: T2DM, hypertension, and obesity.
The Burden of Metabolic Disease and Dietary Risk Factors in India
The scale of metabolic disease in India reflects decades of dietary transition — a shift from traditional high-fibre, pulse-rich diets toward refined carbohydrates, processed foods, and sedentary urban lifestyles. The ICMR-India Diabetes Study 2023 — the most comprehensive national diabetes survey to date — estimates T2DM prevalence at 11.4% and prediabetes at 15.3% of Indian adults, with significant urban-rural and regional variation. NFHS-5 (2019-21) records hypertension in 28.4% of adults aged 15+. Overweight and obesity (BMI ≥25 at Indian cut-offs ≥23) affect approximately 30-35% of urban adults.
The dietary drivers of this epidemic are well-characterised. India's average sodium consumption is 10-12 g salt/day — double the WHO recommended maximum of 5 g/day — driven by high consumption of pickles, chutneys, papad, salty snacks, processed foods, and generous use of table salt. Refined carbohydrate consumption (polished white rice, refined wheat flour, sugar-sweetened beverages, ultra-processed snacks) has risen dramatically, contributing to the high glycaemic load of the average Indian diet. Dietary fibre intake has declined as traditional millet consumption has fallen and polished cereals have replaced millets in many households.
The 'thin-fat Indian' phenotype — characterised by normal or near-normal BMI with excess visceral adiposity (abdominal fat), insulin resistance, and early-onset metabolic risk — means that standard BMI-based thresholds underestimate metabolic disease risk in Indians. Waist circumference (Indian thresholds: men >90 cm, women >80 cm) and waist-to-height ratio provide better metabolic risk screening tools for the Indian context.
The clinical opportunity is significant: structured dietary intervention in newly diagnosed T2DM and pre-hypertension can delay or avoid pharmacological treatment. A 5-10% body weight reduction in an obese diabetic patient improves insulin sensitivity, reduces HbA1c by 0.5-1.0%, and lowers systolic BP by 5-20 mmHg. This is the clinical rationale for community medicine physicians to spend time on dietary counselling — it is not adjunctive care, it is primary treatment.
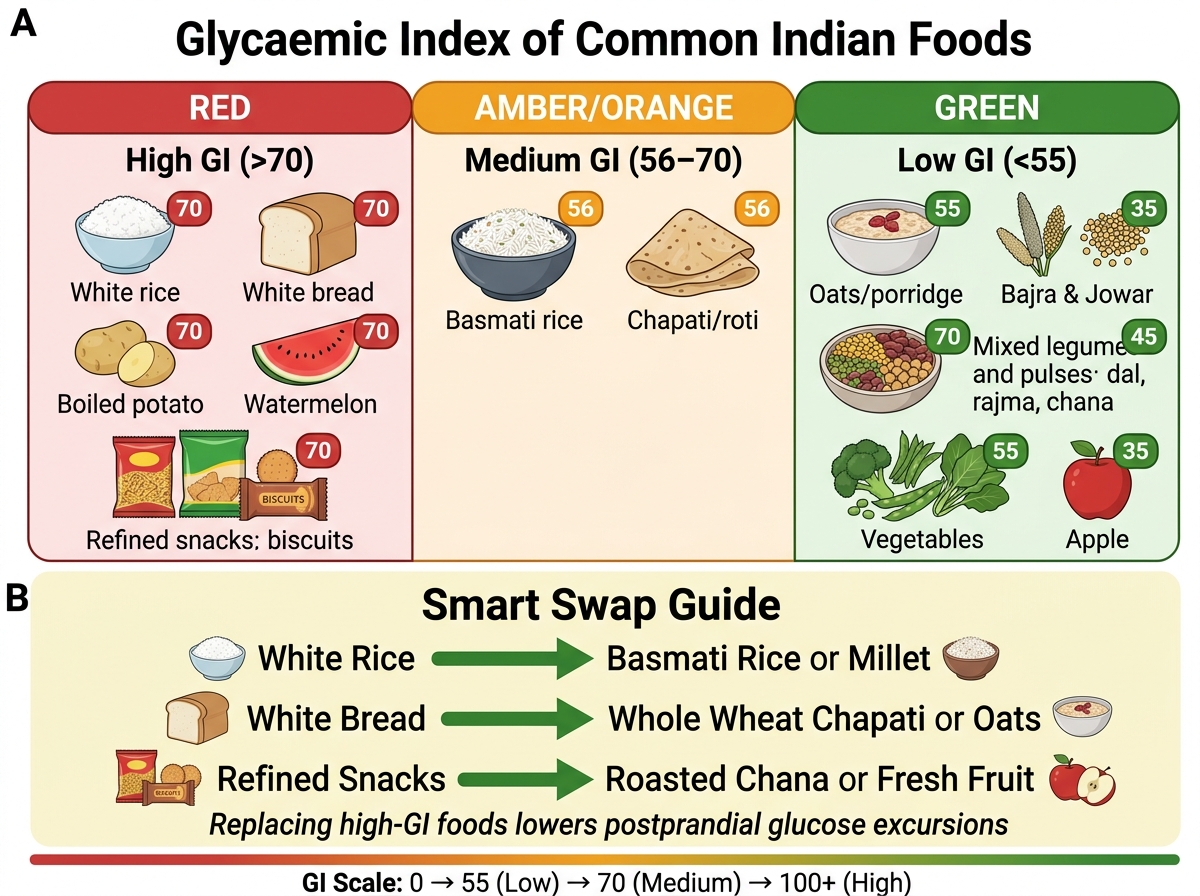
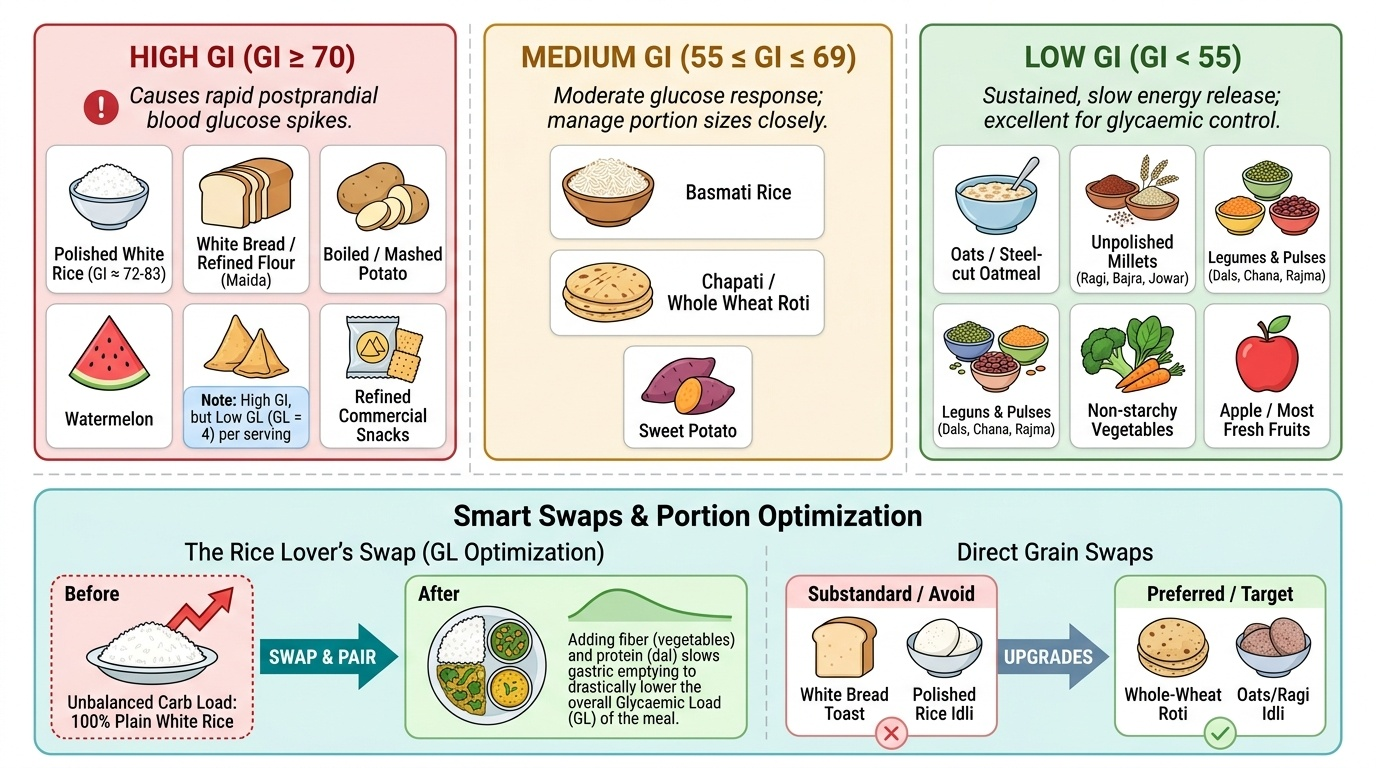
Glycaemic Index Categories of Common Indian Foods and Practical Swap Guide
Dietary Principles for Type 2 Diabetes — Glycaemic Management
Provided image
Dietary management of T2DM targets glycaemic control (reducing postprandial glucose excursions and HbA1c), weight management (energy balance), and cardiovascular risk reduction (fat quality, sodium, fibre). There is no single universally prescribed 'diabetic diet'; the evidence base (ADA 2024, ICMR guidelines) supports multiple evidence-based dietary patterns, all of which share common principles.
Carbohydrate management: Total carbohydrate quantity and distribution across meals is the primary glycaemic control lever. Key principles:
- Distribute carbohydrates across 3 main meals and 1-2 small snacks; avoid large single-meal carbohydrate loads (which produce spike-and-crash glucose profiles)
- Glycaemic Index (GI): A ranking of foods from 0-100 based on their postprandial blood glucose response relative to glucose or white bread. Low GI (<55): oats, millets (ragi, bajra, jowar), most legumes (dal, chana, rajma), non-starchy vegetables, most fruits. Medium GI (55-69): basmati rice, chapati (wheat), sweet potato. High GI (≥70): polished white rice (plain cooked: GI ~72-83), white bread, refined snacks, cornflakes, watermelon, dates.
- Glycaemic Load (GL) = GI × grams of available carbohydrate per serving ÷ 100. GL accounts for both the quality AND the quantity of carbohydrate per serving — a more clinically relevant metric than GI alone. Example: watermelon has high GI (~72) but low GL per typical serving (95g watermelon = GL ~4) because its carbohydrate content per serving is low.
- Practical Indian application: Replace polished white rice with parboiled/red/brown rice, millet-rice combinations (ragi-rice idli, bajra rotis), or reduce portion size and pair with legumes/vegetables to lower the effective GL of the meal. For the patient who 'cannot give up rice' — reducing portion by 25%, adding a large serving of vegetable curry or dal (fibre and protein slow gastric emptying → lower postprandial glucose), and switching from plain boiled rice to parboiled rice achieves meaningful GI reduction within culturally acceptable constraints.
Protein: Maintain ICMR-NIN RDA of 0.83 g/kg/day. Do NOT restrict protein in T2DM without CKD — protein improves satiety, preserves lean muscle mass during weight loss, and has minimal direct effect on blood glucose (unlike carbohydrates). For CKD with T2DM: protein restriction to 0.6-0.8 g/kg/day may be appropriate — refer to a nephrologist and dietitian.
Dietary fat: Prioritise unsaturated fats (nuts, seeds, olive oil, mustard oil) over saturated fats (ghee, coconut oil, processed meats, full-fat dairy). Saturated fat target <10% of total energy. Eliminate trans fats (vanaspati, partially hydrogenated oils in bakery products). Omega-3 fatty acids (flaxseed, walnuts, fatty fish) reduce triglycerides and improve cardiovascular risk profile — important given the cardiovascular risk overlap in T2DM.
Dietary fibre: Target ≥40 g/day (ICMR-NIN 2020); soluble fibre (oats, legumes, vegetables) specifically slows glucose absorption and reduces postprandial glycaemic excursions. Each 10 g/day increase in dietary fibre is associated with a ~0.2% reduction in HbA1c in T2DM populations.
Energy balance: For overweight/obese diabetic patients, a 500-750 kcal/day energy deficit achieves 5-10% body weight reduction, which independently improves insulin sensitivity and may allow dose reduction of antidiabetic medications.
SELF-CHECK
A diabetic patient (60 kg, sedentary, BMI 28) eats 300 g of white rice for lunch (GI ≈ 72, 72 g carbohydrate per 300 g cooked rice). Which food combination, added to the same meal, would most effectively reduce the glycaemic load and postprandial glucose response?
A. A glass of orange juice (adds Vitamin C)
B. A tablespoon of ghee (adds fat which slows carbohydrate absorption)
C. A cup of cooked dal (lentils) and a bowl of mixed vegetable curry
D. A ripe banana (high potassium, good for metabolic health)
Reveal Answer
Answer: C. A cup of cooked dal (lentils) and a bowl of mixed vegetable curry
Adding dal (legumes) and vegetable curry achieves three glucose-blunting mechanisms simultaneously: (1) high dietary fibre from vegetables and legumes slows gastric emptying; (2) protein in dal (plant protein) has minimal direct glycaemic effect while reducing the carbohydrate proportion of total meal energy; (3) the lower GI of legumes reduces the average GI of the combined meal. Ghee (fat) does slow carbohydrate absorption but adds saturated fat calories — not the preferred strategy for a patient with BMI 28. Orange juice and banana both add significant carbohydrate loads and would worsen postprandial glucose. This is the biochemical basis of the traditional Indian rice + dal + vegetable meal pattern as a glycaemic management strategy.
Dietary Principles for Hypertension — Sodium, DASH and Potassium
Dietary management of hypertension has the strongest evidence base of any lifestyle intervention for a non-communicable disease. The DASH diet (Dietary Approaches to Stop Hypertension) in its landmark 1997 trial reduced systolic blood pressure by an average of 8 mmHg in adults and 11 mmHg in hypertensive adults — an effect comparable to a single antihypertensive medication at standard dose, without adverse effects.
Sodium restriction is the single most important dietary intervention for hypertension. WHO recommends <5 g salt/day (<2000 mg sodium/day); the American Heart Association targets <1500 mg sodium/day for high-risk patients. Indian adults consume on average 10-12 g salt/day — achieving 50-60% reduction requires deliberate effort. Practical strategies:
- Remove the salt shaker from the dining table (reduces intake by ~0.5-1 g/day)
- Reduce or eliminate pickles (achar: 1 tsp = ~500-800 mg sodium), papad (one papad = ~300-500 mg sodium), and salty namkeens
- Choose low-sodium salt substitutes (KCl-based 'lo-salt') with caution in patients with CKD or on potassium-sparing diuretics (ACE inhibitors, ARBs) — risk of hyperkalaemia
- Read food labels for sodium content (see cm-nutrition-food-safety module)
- Flavour food with herbs (coriander, cumin, turmeric, garlic, ginger) instead of salt — achieves equivalent palatability with lower sodium
The DASH dietary pattern for Indian patients:
- Increase: Fruits (2-3 servings/day: banana, guava, papaya, amla); vegetables (4-5 servings/day: tomatoes, spinach, methi, capsicum); whole grains (millets, brown/parboiled rice, whole wheat chapati); low-fat dairy (1-2 cups skimmed or low-fat milk/curd per day — calcium and potassium source); nuts and legumes (weekly serving of rajma, chana, moong — potassium, magnesium, protein).
- Reduce: Red and processed meats; sugary beverages (packaged juices, cola, chai with sugar); full-fat dairy; high-sodium condiments (soy sauce, MSG-containing seasonings, ready-to-eat soups).
Potassium blunts the pressor effect of sodium by increasing urinary sodium excretion and directly relaxing vascular smooth muscle. Target: ≥3500 mg potassium/day (WHO). Rich sources in the Indian diet: banana (358 mg/100 g), coconut water (250 mg/100 mL), potato (unpeeled, 535 mg/100 g cooked), spinach (558 mg/100 g), tomato (237 mg/100 g), dal and legumes (700-900 mg/cup cooked). Magnesium and calcium also contribute to blood pressure reduction — sources overlap with the DASH pattern (dairy for calcium, nuts/legumes/green vegetables for magnesium).
Alcohol: Excessive alcohol raises blood pressure; recommend <1 standard drink/day for women, <2 for men (if drinking at all). Each standard drink contains approximately 14 g ethanol.
Weight reduction for overweight hypertensive patients: each 1 kg of weight loss reduces systolic BP by approximately 1 mmHg — a 10 kg weight loss (achievable with 500-750 kcal/day deficit over 3-4 months) can lower systolic BP by ~10 mmHg, potentially achieving hypertension control without medication in Stage-1 hypertension.
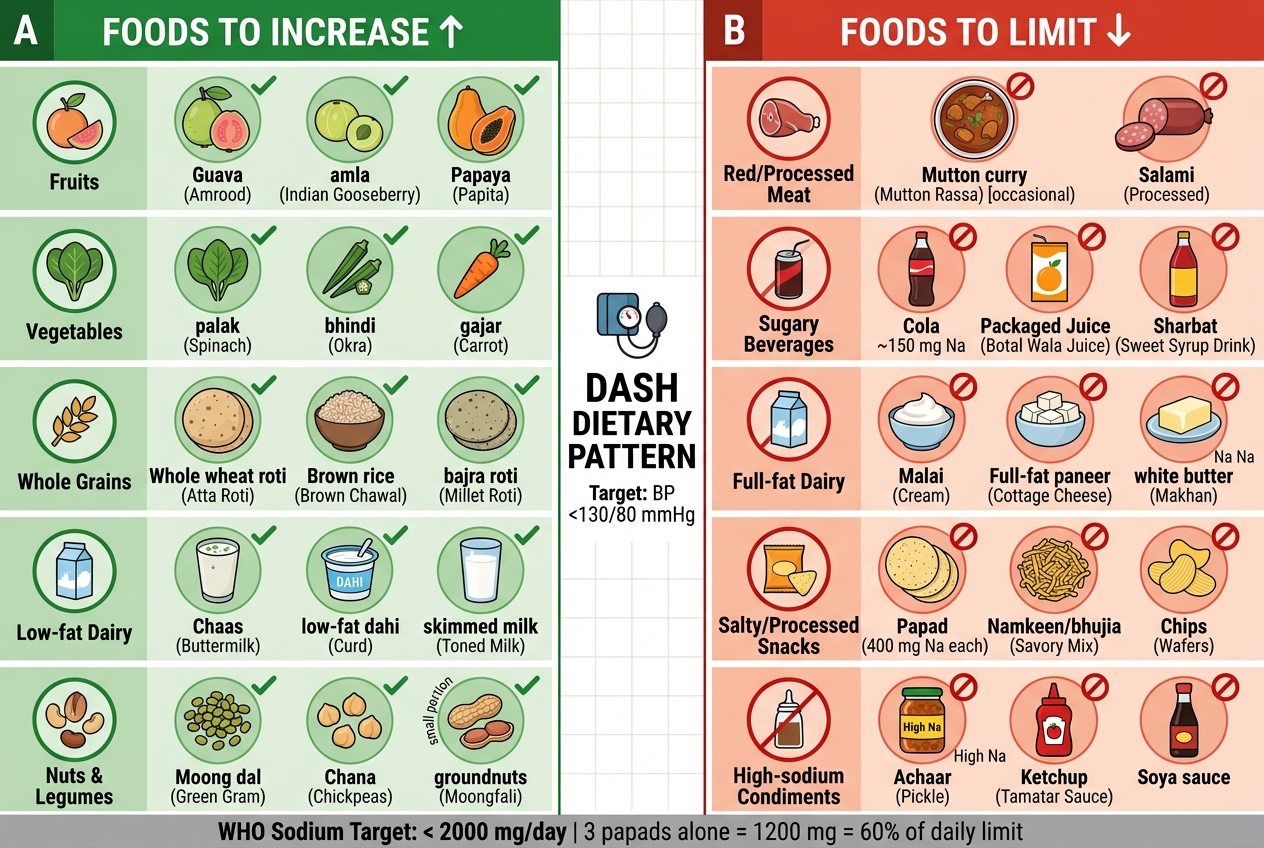
DASH Dietary Pattern: Foods to Increase and Limit — Indian Food Examples
SELF-CHECK
A 52-year-old hypertensive patient (BP 146/92 mmHg on a single antihypertensive medication) reports eating papad with every meal. Each papad contains approximately 400 mg sodium. If he eats 3 papads daily, what proportion of his WHO recommended daily sodium limit does this contribute, and what is the most practical single substitution you would recommend?
A. 600 mg = 15% of 4000 mg WHO limit; substitute with low-fat yoghurt
B. 1200 mg = 60% of 2000 mg WHO limit; substitute roasted cumin + lemon as a table condiment
C. 400 mg = 8% of 5000 mg WHO limit; no substitution needed
D. 1200 mg = 60% of 2000 mg WHO limit; substitute with salted butter on chapati instead
Reveal Answer
Answer: B. 1200 mg = 60% of 2000 mg WHO limit; substitute roasted cumin + lemon as a table condiment
Three papads × 400 mg sodium = 1200 mg sodium. WHO recommends <2000 mg sodium/day. Therefore, papad contributes 1200/2000 = 60% of the daily sodium limit from a single condiment — leaving only 800 mg sodium for all meals and other food sources. The most practical substitution is roasted cumin (jeera) powder with a squeeze of lemon on dal or food — it provides flavour intensity, supports digestion (jeera's traditional role), and contributes negligible sodium. Low-fat yoghurt is a good general addition but does not specifically replace the flavour role of papad. Salted butter adds more sodium and saturated fat.