Page 20 of 32
CM5.{10,20} | CM5.{10,20} | Diet Modification for Metabolic Risk Clinics — SDL Guide (Part 3)
Prescribing a Dietary Plan in a Simulated Setting
The OSCE skill for CM5.10 and CM5.20 is to produce a written one-day diet plan for a specified patient profile, within a 5-10 minute window. The following structured checklist ensures a complete, examinable diet plan.
Provided image
Step 1 — Document patient parameters: Age, sex, weight (kg), height/BMI, physiological state, activity level, condition (T2DM/HTN/obesity), dietary pattern (vegetarian/non-vegetarian), economic constraints.
Step 2 — Set energy target: Calculate using ICMR-NIN 2020 reference or simplified BMR × activity factor. For T2DM with weight reduction: BMR × 1.3 (sedentary) = TEE → subtract 500 kcal for deficit. Example: 55 kg sedentary woman TEE ≈ 1660 kcal → weight loss target 1160 kcal.
Step 3 — Set key nutrient targets: Protein ≥ 0.83 g/kg (46 g for 55 kg woman); sodium <2000 mg/day (HTN); carbohydrate 50-55% of energy with preference for low-GI foods; fat <30% with saturated fat <10%; fibre ≥40 g.
Step 4 — Write the meal plan (breakfast → mid-morning → lunch → evening snack → dinner):
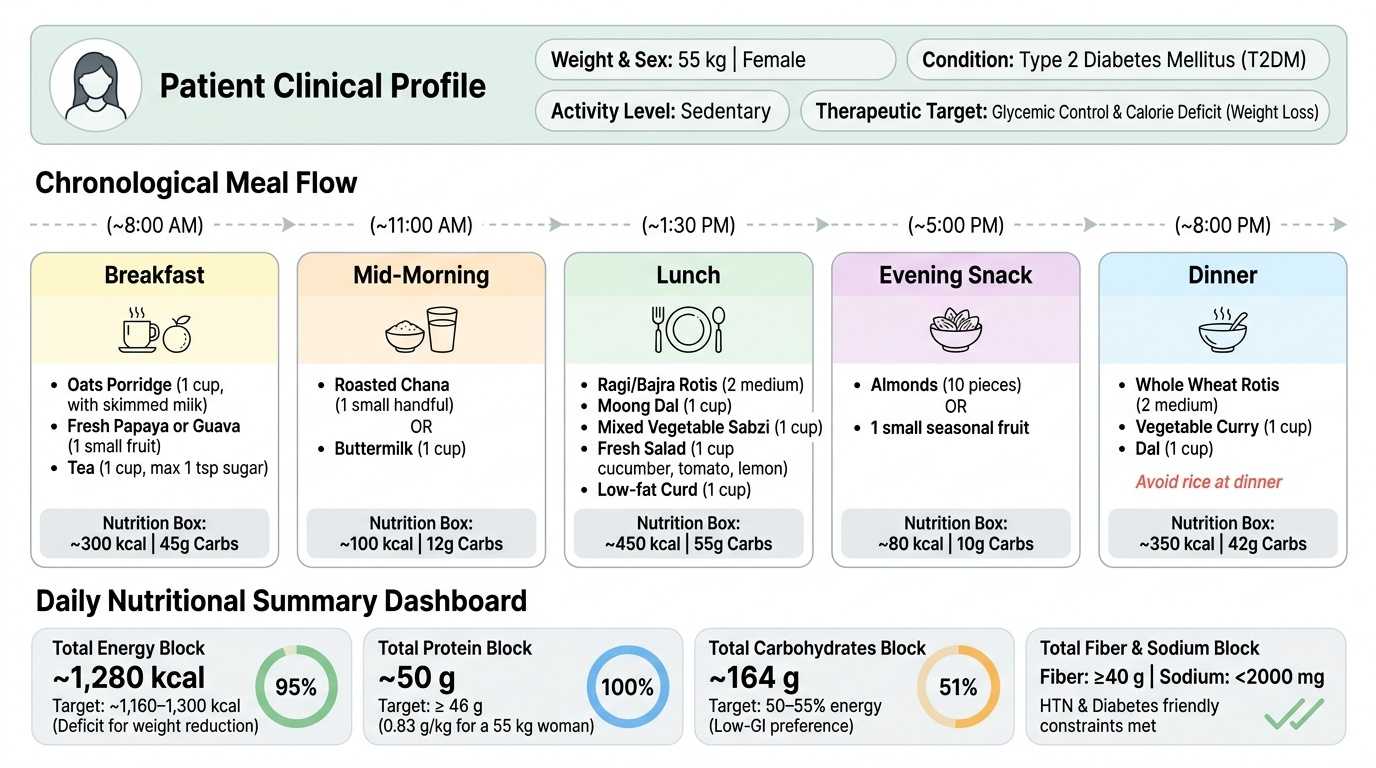
Example for 55 kg sedentary T2DM woman, vegetarian, 1660 kcal target:
- Breakfast: 1 cup oats porridge with skimmed milk + 1 small fruit (guava or papaya); tea with <1 tsp sugar
- Mid-morning: A small handful of roasted chana or 1 cup buttermilk
- Lunch: 2 medium ragi/bajra rotis + 1 cup moong dal + 1 cup mixed vegetable sabzi + 1 cup salad (cucumber, tomato, lemon); 1 cup curd
- Evening: 1 small fruit or 10 almonds
- Dinner: 2 medium rotis (whole wheat) + 1 cup vegetable curry + 1 cup dal; avoid rice at dinner
Step 5 — State counselling points: Replace white rice with millets or parboiled rice; reduce papad/pickle; no sugary beverages; add 30 minutes of brisk walking; follow up in 4 weeks.
SELF-CHECK
A 60-year-old hypertensive and diabetic patient (58 kg, BMI 26.5, sedentary) is seen in the NCD clinic. Her HbA1c is 8.4% and BP is 152/96 mmHg on two antihypertensives. She is vegetarian. Which dietary pattern would simultaneously address both her conditions most effectively?
A. High-fat, low-carbohydrate ketogenic diet — eliminates glycaemic load entirely
B. High-protein diet (1.5 g/kg/day) with low sodium — reduces BP and HbA1c
C. A DASH-aligned diet with low-GI carbohydrates, high fibre, restricted sodium, and reduced saturated fat
D. Fasting every alternate day — calorie restriction to reduce both glucose and BP
Reveal Answer
Answer: C. A DASH-aligned diet with low-GI carbohydrates, high fibre, restricted sodium, and reduced saturated fat
A DASH-aligned, low-GI, high-fibre diet with sodium restriction addresses both conditions through a convergent mechanism: DASH reduces BP (by potassium, magnesium, calcium, sodium restriction, and weight reduction); low-GI carbohydrates and high fibre reduce postprandial glycaemia and HbA1c. Ketogenic diet is not evidence-based as a first-line dietary intervention in T2DM in the community medicine context and poses risks for a hypertensive patient with potentially compromised renal function. A very high protein diet (1.5 g/kg for CKD-risk patients) requires nephrology clearance. Alternate-day fasting lacks robust evidence in older adults with multiple comorbidities and risks hypoglycaemia in a patient on antidiabetic agents.
CLINICAL PEARL
Millets are the metabolic disease physician's best kept secret in India. Ragi (finger millet, Eleusine coracana) has a GI of approximately 68 — medium range — but a significantly lower glycaemic load than polished white rice for an equivalent serving size, AND provides 344 mg calcium per 100 g (the highest of any cereal — valuable in a dairy-restricted diet), 3.9 mg iron per 100 g, and 3.6 g dietary fibre per 100 g. Bajra (pearl millet) GI is approximately 55 (medium-low) and provides 11 mg iron, 3.1 mg zinc, and 1.3 g soluble fibre per 100 g — improving glycaemic control through both GI and fibre mechanisms. Sorghum (jowar) has a GI of 49 — genuinely low — and is a traditional staple in Maharashtra, Karnataka, and Andhra Pradesh. The Government of India's Shree Anna (Millets) initiative (2023) explicitly promotes millets as 'Nutri-cereals' for precisely these reasons. For a diabetic patient who cannot give up rice — a small serving of parboiled red rice blended with 30-40% cooked ragi or bajra reduces the effective GI of the combination meal while maintaining cultural familiarity. This is culturally contextualised, evidence-informed clinical nutrition counselling.