Page 6 of 32
CM5.{2,4,9,11} | CM5.{2,4,9,11} | Nutritional Assessment and Diet Planning — SDL Guide (Part 2)
Principles of Diet Planning — From Needs to Food Choices
Diet planning is a structured clinical process — not an intuitive suggestion of 'eat more vegetables.' The ICMR-NIN five-step framework converts nutritional assessment findings into a practical, locally feasible dietary prescription.
Step 1: Assess nutritional needs. Gather key parameters: age, sex, weight, height, physiological state (pregnancy, lactation), activity level, health conditions (diabetes, hypertension, anaemia), and dietary preferences (vegetarian, cultural restrictions). This step uses the ABCD assessment from the previous section.
Step 2: Set energy and nutrient targets. Using ICMR-NIN 2020 RDA, calculate daily energy requirement (BMR × activity factor) and determine targets for protein, iron, calcium, and other nutrients relevant to the individual. Example: a 25-year-old sedentary woman, 55 kg, non-pregnant — energy target ~1660 kcal/day; protein target 46 g/day (0.83 × 55).
Step 3: Select food groups. The ICMR-NIN food groups model provides five core groups: (1) cereals and millets, (2) pulses and legumes, (3) dairy and animal products, (4) fruits and vegetables, (5) oils and fats. Each group contributes specific nutrients: cereals = energy + B vitamins; pulses = protein + iron + zinc; dairy = calcium + protein; fruits and vegetables = vitamins, minerals, fibre; oils = fat-soluble vitamin carrier + essential fatty acids. Diversity within and across groups is the practical principle — no single food provides all nutrients adequately.
Step 4: Plan the daily meal pattern. Distribute food group servings across meals (breakfast, mid-morning snack, lunch, evening snack, dinner) to achieve the nutrient targets from step 2. Use locally available and affordable foods — a diet plan that includes foods the patient cannot access or afford will not be followed. For example, in Bihar, sattu (roasted chana flour) is an affordable, high-protein local food; in Tamil Nadu, ragi (finger millet) provides both energy and calcium.
Step 5: Validate against targets. Calculate the approximate nutrient content of the planned diet using standard food composition tables (IFCT 2017 — Indian Food Composition Tables, NIN) and compare to the step-2 targets. Adjust serving sizes or food choices if gaps remain. This is the quality-assurance step that distinguishes a scientifically planned diet from a guess.
Protein Planning — Vegetarian, Ovo-vegetarian and Non-vegetarian Diets
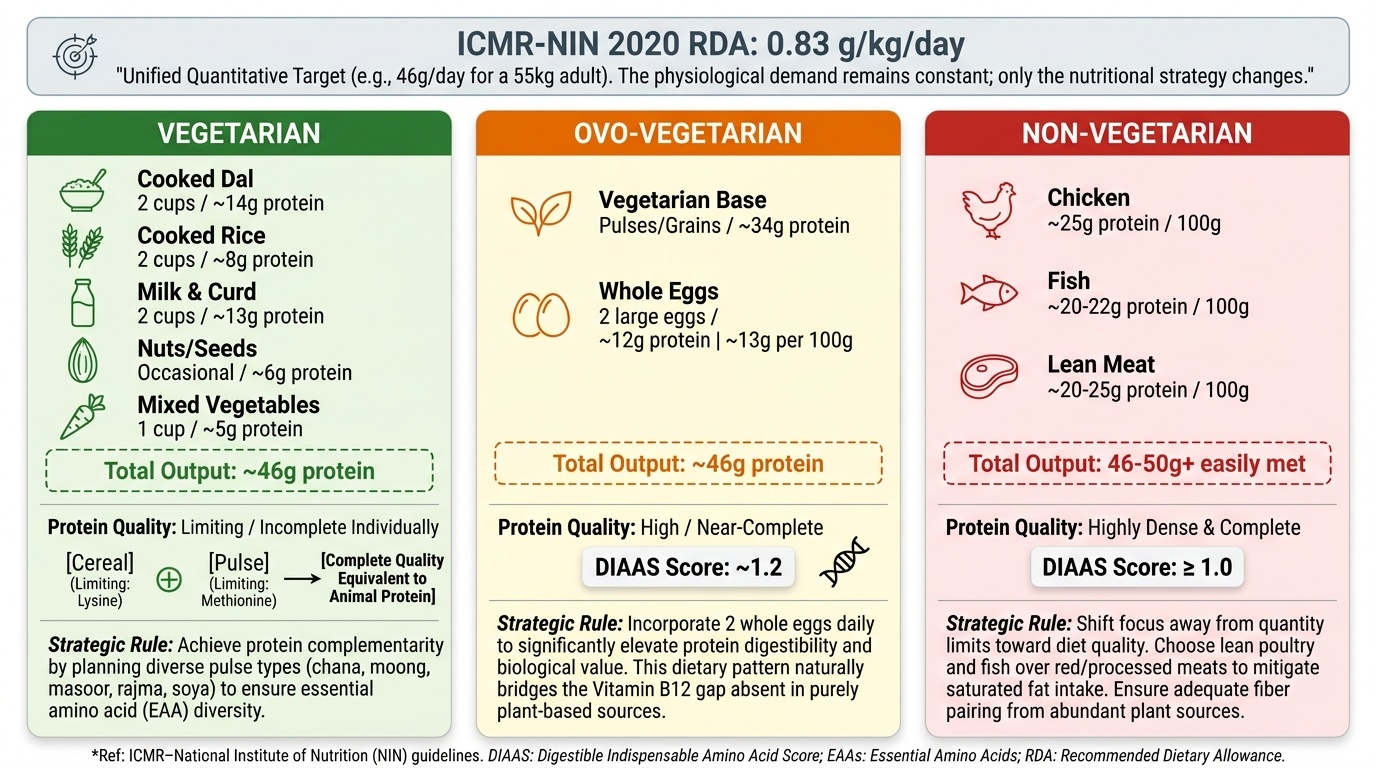
The ICMR-NIN 2020 protein RDA of 0.83 g/kg/day applies to all dietary patterns — vegetarian, ovo-vegetarian, and non-vegetarian alike. What changes across dietary patterns is the source and biological quality of protein, not the quantity required by the body. This is a key conceptual distinction: the recommendation is the same; the strategy to meet it differs.
Protein quality and complementarity: Animal proteins (eggs, meat, fish, milk, paneer) are 'complete' — they contain all nine essential amino acids (EAA) in adequate proportions and have high digestibility (DIAAS ≈ 1.0 for eggs). Most plant proteins are 'limiting' in one or more EAA: cereals are limiting in lysine; pulses are limiting in methionine and cysteine. However, complementary protein combining — eating limiting plant proteins together — achieves a complete EAA profile. The classic Indian example: rice + dal combines cereal methionine + pulse lysine to produce a complementary EAA profile equivalent to animal protein. This is not merely traditional wisdom — it is biochemically sound nutrition.
For a vegetarian adult (55 kg woman, sedentary): To meet 46 g protein/day from plant sources — 2 cups of cooked dal (~14 g protein), 2 cups cooked rice (~8 g), 1 cup milk (~8 g), 1 cup curd (~5 g), occasional nuts/seeds (~6 g), 1 cup cooked mixed vegetables (~5 g) = approximately 46 g. The key is variety across pulse types (chana, moong, masoor, rajma, soya) to ensure EAA diversity.
For an ovo-vegetarian adult: Eggs are nutritionally near-complete proteins (DIAAS ~1.2). One large egg provides ~6 g high-quality protein. Adding 2 eggs/day to a vegetarian base significantly improves both protein quantity and quality without requiring other animal foods. Egg consumption also provides Vitamin B12, which is absent from purely plant-based diets.
For a non-vegetarian adult: Animal proteins (chicken ~25 g protein/100 g; fish ~20-22 g/100 g; meat ~20-25 g/100 g) are dense and high-quality. Meeting 46-50 g protein is readily achievable. The planning consideration shifts toward avoiding excess saturated fat (from red/processed meat) and ensuring adequate fibre from plant foods alongside animal protein sources.
Practical rule: For vegetarians, the key constraints are (1) meeting lysine needs from diverse pulses (not just wheat-based diet), and (2) ensuring Vitamin B12 adequacy (dairy is the primary source; strict vegans need supplementation or fortified foods). For non-vegetarians, the constraint is often excess caloric density from animal fat rather than protein inadequacy.
Provided image
SELF-CHECK
A strict vegetarian adult man (60 kg, sedentary) wants to plan a diet meeting his protein RDA. According to ICMR-NIN 2020, what is his daily protein requirement, and which combination of plant foods best addresses the lysine-methionine complementarity problem?
A. 60 g/day; wheat chapati + green vegetables
B. 50 g/day; rice + dal (pulse)
C. 75 g/day; rice + dal + vegetables
D. 50 g/day; wheat only, if consumed in sufficient quantity
Reveal Answer
Answer: B. 50 g/day; rice + dal (pulse)
ICMR-NIN 2020 protein RDA is 0.83 g/kg/day; for 60 kg man = 50 g/day. Rice and other cereals are limiting in lysine; pulses (dal) are limiting in methionine. When combined, they provide a complementary EAA profile — rice's methionine supplements the pulse's lysine deficiency and vice versa. Wheat alone, even in large quantities, remains lysine-limiting. This is the biochemical basis of the traditional Indian rice-dal combination as a protein-adequate vegetarian meal.
Monitoring and Evaluating Diet Adequacy
A diet plan is only as good as its follow-up. Monitoring transforms a one-time clinical interaction into a sustained nutrition intervention. At the individual level, monitoring includes: repeat anthropometry (weight, BMI, MUAC) at defined intervals (monthly for SAM/MAM children; quarterly for adults with nutritional deficiency); repeat biochemical markers (haemoglobin at 3 months for iron deficiency anaemia treatment; serum ferritin at 6 months); symptom review (energy levels, appetite, wound healing); and a follow-up 24-hour dietary recall to assess whether dietary advice was actually implemented.
At the community level, nutritional surveillance is systematic: ICDS weighing of children under 5 monthly at Anganwadi Centres generates growth faltering data that triggers referral to NRC; ASHA workers conduct home visits to monitor complementary feeding practices; NFHS surveys every 5 years provide state- and district-level trend data for programme planning.
Dietary diversity score monitoring is a simple community tool: a score ≥5 of 10 food groups in 24 hours (MDD-W, Women's Dietary Diversity, WHO) indicates micronutrient adequacy. Anganwadi workers and ASHA workers can administer this at household visits. For children 6-23 months, a dietary diversity score of ≥5 of 8 food groups is the IYCF indicator for minimum dietary diversity.
Programme-level evaluation links individual assessment data to population outcomes: POSHAN Abhiyaan's real-time POSHAN Tracker allows state-level monitoring of stunting, wasting, underweight, and anaemia progress, supporting course correction in programme delivery.