Page 9 of 32
CM5.3 | CM5.3 | Nutrition Related Disorders — SDL Guide
Learning Objectives
- Define and describe common nutrition-related health disorders including macro-PEM and key micronutrient deficiencies (iron, zinc, iodine, Vitamin A)
- Describe the clinical features that distinguish kwashiorkor from marasmus
- Outline the control and management strategies for major nutrition-related disorders including national programme components
- Recognise clinical and community presentations of nutritional deficiency and initiate appropriate management
INSTRUCTIONS
India simultaneously battles undernutrition that stunts children's development and overnutrition that drives a rising epidemic of diabetes and hypertension. This module covers the specific disorders that result from nutritional deficiency — their clinical features, their burden in India, and how to prevent and manage them.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 11 — Nutrition and Health (textbook)
- WHO/UNICEF 2023 — Management of Severe Acute Malnutrition (textbook)
- ICMR-NIN 2020 — Recommended Dietary Allowances for Indians (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At an Anganwadi Centre in a tribal district of Jharkhand, a health worker weighs a 3-year-old boy. His weight-for-height Z-score is -3.2 and his MUAC is 11.2 cm. He has bilateral pitting oedema of the feet, sparse reddish hair, and patches of skin with peeling hyperpigmentation — 'flaky paint' appearance. In the next village, a 2-year-old girl weighs 7.1 kg (expected ~12 kg for age) with a wizened, 'old man' face, gross muscle wasting, prominent ribs, and no oedema. These two children represent the two ends of the protein-energy malnutrition (PEM) spectrum — kwashiorkor and marasmus respectively — and together they illustrate why nutrition-related disorders remain India's most prevalent and preventable cause of child mortality and morbidity. Recognising the difference matters: it changes the management protocol, the prognosis, and the family counselling.
WHY THIS MATTERS
Nutrition-related disorders are the single largest contributor to India's disease burden among under-5s and a major driver of adult NCDs. CM5.3 requires you to define and describe these disorders including 'their control and management' — making this a comprehensive competency spanning clinical recognition, community prevention, and national programme knowledge. In community medicine postings, at Anganwadi visits, NRC (Nutrition Rehabilitation Centre) rounds, and village health surveys, you will encounter PEM, IDA, VAD, and IDD as real clinical and public health problems. In OSCE settings, clinical case photographs and examination findings will test your ability to distinguish kwashiorkor from marasmus, identify xerophthalmia stages, and describe the appropriate national programme response to each disorder.
RECALL
From the cm-nutrition-requirements module: recall that protein yields 4 kcal/g with an RDA of 0.83 g/kg/day; iron RDA adult woman is 29 mg/day; iodine RDA adult is 150 µg/day; Vitamin A RDA adult man is 900 µg RAE/day. From the cm-nutrition-assessment module: recall the ABCD framework for assessment — anthropometry, biochemistry, clinical signs, and dietary recall. The clinical signs you are about to learn in this module are the 'C' (Clinical) component of that framework. From Biochemistry (BI): recall the role of thyroid hormones (requiring iodine) in metabolic regulation, and retinol's role in vision (rhodopsin formation).
Burden of Nutrition-Related Disorders in India
India's nutritional disorder burden is simultaneously one of the largest in the world and one of the most complex, because it reflects the double burden of malnutrition — undernutrition and overnutrition coexisting at the population level. NFHS-5 (2019-21) documents that 35.5% of children under five are stunted (chronic PEM), 19.3% are wasted (acute PEM or SAM/MAM), and 32.7% are underweight. Anaemia — predominantly iron deficiency — affects 67.1% of children aged 6-59 months and 57.0% of women aged 15-49. Simultaneously, 24.0% of adult women and 22.9% of adult men are overweight or obese, and the prevalence of Type 2 diabetes has risen to 8-10% of adults in India (ICMR-India Diabetes study 2023).
The economic costs are staggering. The World Bank estimates that malnutrition costs India approximately 3% of GDP annually through lost productivity, increased healthcare expenditure, and reduced cognitive human capital. Hidden hunger — the term for micronutrient deficiency without visible wasting — is particularly insidious: a child may have a normal weight-for-height yet be simultaneously deficient in iron, Vitamin A, and zinc, each deficiency compounding the others through immune impairment and growth signalling disruption.
India's National Family Health Survey reveals substantial state-wise heterogeneity: Bihar, Uttar Pradesh, and Jharkhand bear the highest burdens of undernutrition, while Kerala, Goa, and the metro cities lead in overweight prevalence. This heterogeneity demands locally calibrated programme strategies rather than a single national response.
Protein-Energy Malnutrition: Comparative Features of Kwashiorkor, Marasmus, and Marasmic-Kwashiorkor
Protein-Energy Malnutrition — Kwashiorkor and Marasmus
Provided image
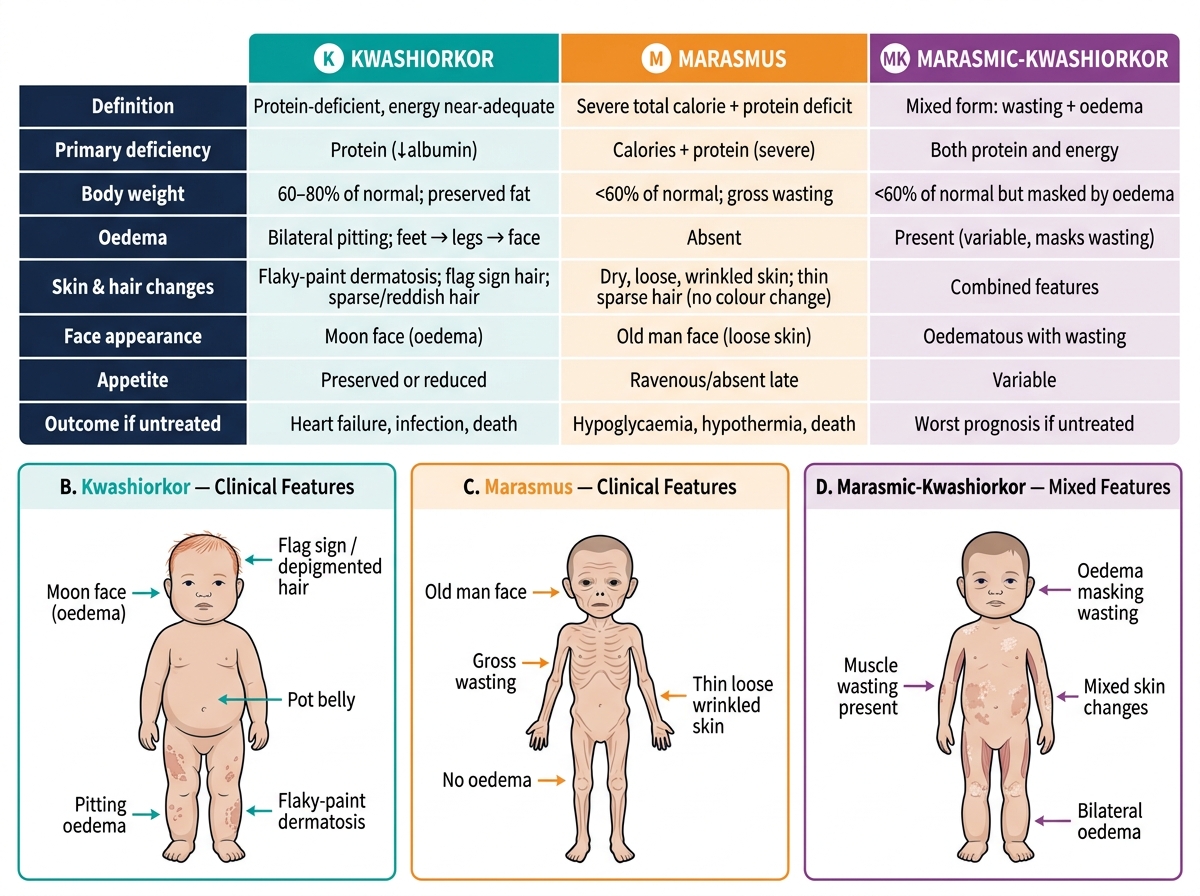
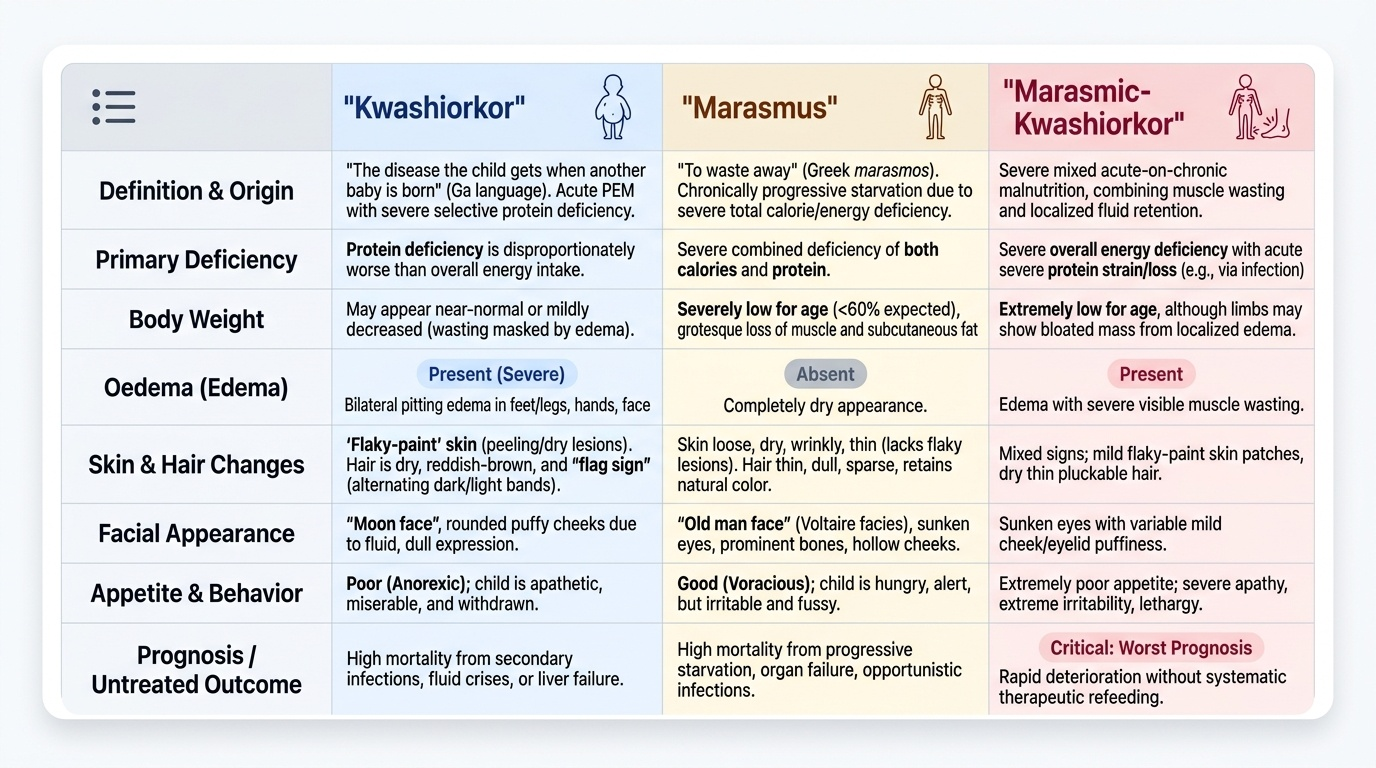
Protein-Energy Malnutrition (PEM) is the collective term for disorders resulting from inadequate intake of calories, protein, or both, leading to deficits in body mass and function. The two classical syndromes are kwashiorkor and marasmus, though in practice the mixed form — marasmic-kwashiorkor — is equally common.
Kwashiorkor (from the Ga language of Ghana: 'the disease the child gets when another baby is born') is caused primarily by protein deficiency, often in the context of adequate or near-adequate energy intake. The pathophysiology centres on hypoalbuminaemia (low serum albumin → reduced oncotic pressure → oedema), deficiency of transport proteins, and immune failure. Cardinal clinical features:
- Bilateral pitting oedema — the sine qua non; begins in feet, progresses to legs and face ('moon face')
- 'Flaky-paint' skin — hyper- and hypopigmented, dry, peeling areas; especially over pressure points
- Hair changes — sparse, reddish-brown, easily pluckable ('flag sign' — bands of hair colour reflecting nutritional episodes)
- Apathy and misery — withdrawn, anorexic
- 'Pot belly' — from hepatomegaly (fatty liver) + ascites + muscle wasting of abdominal wall
- Weight may appear near-normal due to oedema masking wasting
Marasmus (from Greek marasmos, 'to waste away') results from severe, prolonged combined energy and protein deficiency — essentially starvation. The body catabolises its own protein (skeletal muscle) and fat (subcutaneous) for energy. Cardinal clinical features:
- Severe wasting — 'skin and bones'; grossly visible rib cage, prominent long bones
- 'Old man face' (Voltaire facies) — loss of buccal fat pads, sunken eyes, wizened appearance
- NO oedema — this is the key distinguishing feature from kwashiorkor
- Weight severely low for age (usually <60% expected weight-for-age)
- Serum albumin may be low but less dramatically than in kwashiorkor
- Child is often alert, hungry, irritable (unlike the apathetic kwashiorkor child)
Marasmic-kwashiorkor shows wasting (from energy deficiency) PLUS oedema (from superimposed protein deficiency), often triggered by a precipitating infection in a marasmic child. It carries the worst prognosis of the three.
Determinants of PEM in the community: inadequate household food security, inappropriate complementary feeding (starting too late, too dilute, too infrequent), recurrent infections (diarrhoea, respiratory infections — increasing nutrient demands and reducing absorption), poverty, lack of maternal education, and poor WASH (water, sanitation, hygiene). The nutrition-infection cycle is critical: PEM impairs immune function → increased infection frequency and severity → infection causes anorexia and catabolism → worsening PEM. Breaking this cycle requires simultaneous nutritional rehabilitation AND infection management.
SELF-CHECK
A 2-year-old child from a food-insecure household is brought to an NRC with severe oedema of the feet and lower legs. His hair is sparse and reddish. He is apathetic and anorexic. His weight-for-height Z-score is -2.1. What is the most likely diagnosis?
A. Marasmus
B. Marasmic-kwashiorkor
C. Kwashiorkor
D. Moderate Acute Malnutrition (MAM)
Reveal Answer
Answer: C. Kwashiorkor
Bilateral pitting oedema, reddish sparse hair, apathy, and anorexia in the context of food insecurity point to kwashiorkor — a primarily protein-deficiency form of PEM. Note that the WHZ of -2.1 is above the -3 cutoff for SAM by weight criteria, but bilateral oedema ALONE qualifies as SAM regardless of weight (WHO diagnostic criteria). In marasmus, there is NO oedema. Marasmic-kwashiorkor shows both severe wasting (WHZ <-3) AND oedema — this child's WHZ of -2.1 with oedema suggests kwashiorkor predominating.
Micronutrient Deficiency Disorders — Iron, Iodine and Vitamin A
Micronutrient deficiency disorders constitute India's 'hidden hunger' — deficiencies that impair health, cognition, and immune function without always producing visible wasting. The three most epidemiologically significant in India are Iron Deficiency Anaemia (IDA), Iodine Deficiency Disorders (IDD), and Vitamin A Deficiency (VAD).
Iron Deficiency Anaemia (IDA): Iron deficiency is the world's most prevalent nutritional disorder, affecting an estimated 2 billion people globally. In India, NFHS-5 records anaemia in 57.0% of women aged 15-49 and 67.1% of children 6-59 months. IDA develops in stages: (1) iron depletion (reduced ferritin, serum ferritin <12 µg/L); (2) iron-deficient erythropoiesis (reduced transferrin saturation, increased TIBC); (3) iron deficiency anaemia (haemoglobin <12 g/dL in non-pregnant women, <11 g/dL in pregnant women; microcytic, hypochromic red cells). Clinical features: pallor (conjunctival, palmar), fatigue, palpitations, breathlessness on exertion, koilonychia (spoon nails), angular stomatitis, glossitis (in severe cases), and in children: impaired cognitive development and reduced attention span. Key determinants: low dietary iron, high phytate diet reducing non-haem iron bioavailability, menstrual losses in women, hookworm infestation, repeated pregnancies.
Iodine Deficiency Disorders (IDD): Iodine is essential for synthesis of thyroid hormones T3 and T4. Deficiency affects all ages but consequences are most severe during foetal development and infancy. The spectrum of IDD includes:
- Goitre — enlargement of the thyroid gland; the most visible sign of iodine deficiency; classified by WHO grading (0=no goitre; 1=palpable but not visible; 2=visible without neck extension)
- Cretinism — severe neurological impairment from intrauterine/neonatal iodine deficiency; clinical features: intellectual disability (the most devastating consequence), deaf-mutism, squint, spastic diplegia, growth retardation (myxoedematous type: hypothyroidism + growth failure). Cretinism is irreversible — prevention is the only solution, via adequate maternal iodine during pregnancy
- Other IDD: increased spontaneous abortion, stillbirth, neonatal hypothyroidism, impaired cognitive function at subclinical levels
Prevention: Universal Salt Iodisation (USI) — mandating 15 ppm iodine in all edible salt at consumer level (India's NIDDCP). USI has reduced goitre prevalence from ~54% (1980s) to <5% in most Indian districts.
Vitamin A Deficiency (VAD): Vitamin A (retinol) is essential for photoreceptor function (rhodopsin in rod cells — night vision), epithelial integrity, and immune function. Deficiency produces a spectrum of eye disease called xerophthalmia, staged by WHO:
- XN: Night blindness — earliest and most common clinical sign; impaired dark adaptation
- X1A: Conjunctival xerosis — dryness and wrinkling of bulbar conjunctiva
- X1B: Bitot's spots — triangular, foamy white patches of keratinised epithelium on the temporal bulbar conjunctiva, pathognomonic of VAD
- X2: Corneal xerosis — dryness, haziness of cornea
- X3A/X3B: Corneal ulceration (kwashiorkor + VAD accelerates corneal ulceration)
- XS: Corneal scar (permanent, even with treatment)
- XF: Xerophthalmic fundus (rare — fundal changes)
Beyond vision: VAD impairs epithelial barriers (respiratory, GI, urinary tracts) → increased severity of infections. Children with VAD have 24% higher all-cause mortality (WHO). India's Vitamin A supplementation programme (biannual megadose: 100,000 IU for children 6-11 months; 200,000 IU for 12-59 months) under VHSND (Village Health, Sanitation and Nutrition Days) is the primary control strategy.
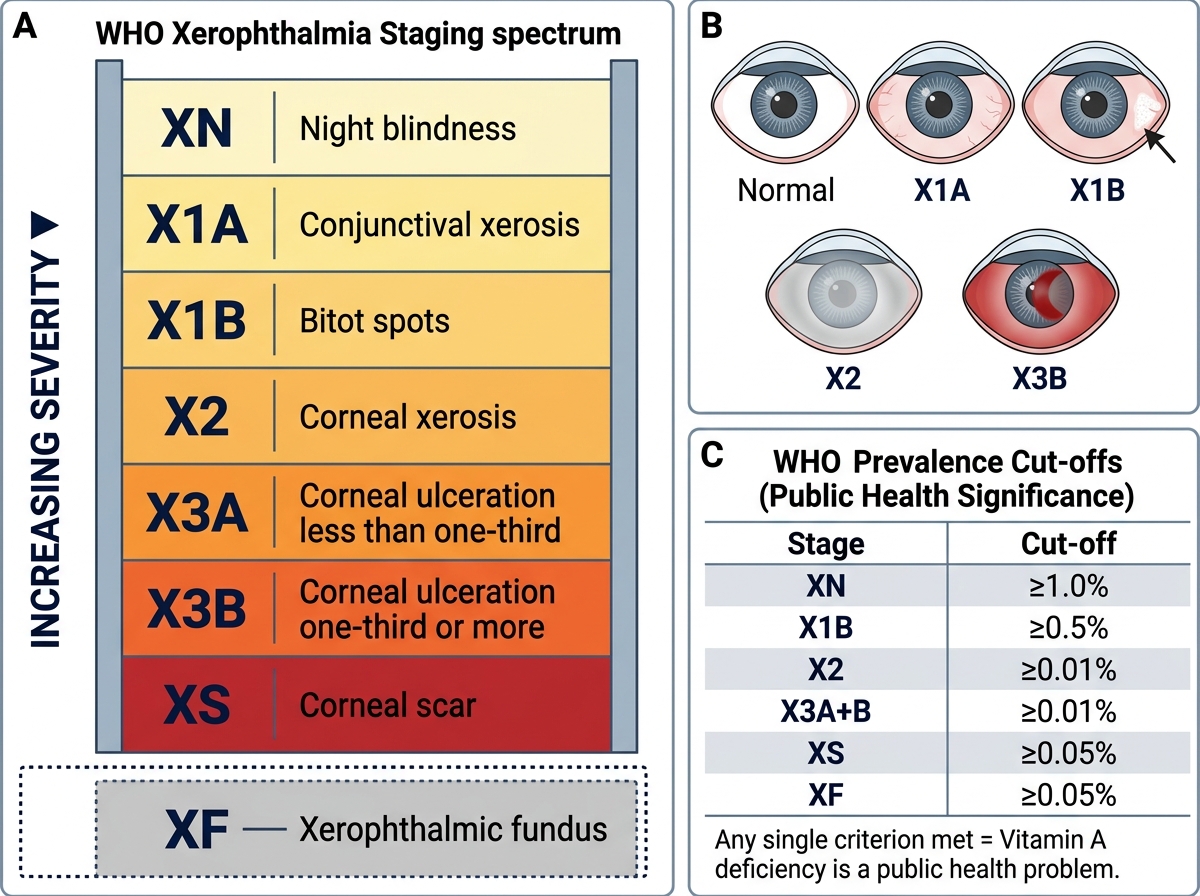
WHO Xerophthalmia Staging: Spectrum of Vitamin A Deficiency Eye Signs with Prevalence Cut-offs
SELF-CHECK
A village health worker identifies two children in a tribal hamlet. Child A: night blindness for 2 months, white foamy patches on the temporal conjunctiva bilaterally, otherwise well. Child B: corneal haziness and dullness, very malnourished, pallor. What are the xerophthalmia stages for Child A and Child B respectively, and which requires EMERGENCY treatment to prevent blindness?
A. Child A: XN; Child B: X1B — both require equal urgency
B. Child A: X1B; Child B: X2 — Child B requires emergency treatment
C. Child A: X1A; Child B: XS — Child A requires treatment first
D. Child A: X2; Child B: X3A — Child A requires emergency treatment
Reveal Answer
Answer: B. Child A: X1B; Child B: X2 — Child B requires emergency treatment
Child A has Bitot's spots (triangular foamy conjunctival patches) = stage X1B, combined with XN (night blindness). Child B has corneal xerosis (haziness/dullness) = stage X2. Stage X2 and beyond (corneal involvement) constitutes an ophthalmic emergency — rapid progression to corneal ulceration (X3) and perforation can lead to permanent blindness within days to weeks, especially if the child is concurrently malnourished or infected. Child A's Bitot's spots (X1B) are clinically significant and should be treated (Vitamin A megadose), but do not carry the same emergency urgency as corneal involvement. Both should receive Vitamin A treatment, but Child B is the emergency.