Page 1 of 15
CM11.{1,3-4} | CM11.{1,3-4} | Occupational Illness, Hazards and Ergonomics — SDL Guide
Learning Objectives
- Enumerate and describe the presenting features of patients with occupational illness, including agriculture-related illness (CM11.1)
- Enumerate and describe specific occupational health hazards, their risk factors, and preventive measures (CM11.3)
- Describe the principles of ergonomics in health preservation (CM11.4)
INSTRUCTIONS
Millions of workers worldwide are exposed daily to hazards in their workplaces — from silica dust in stone quarries to organophosphate pesticides in agriculture. Occupational illness is both preventable and under-diagnosed; a physician who takes a thorough occupational history can identify causes of disease that no investigation will reveal. This module equips you to recognise, classify, and prevent the major occupational diseases, and to apply ergonomic principles to protect worker health.
References
- Park's Textbook of Preventive & Social Medicine, 26th ed. — Chapter: Occupational Health (textbook)
- ILO International Classification of Radiographs of Pneumoconioses (2011 revision) (textbook)
- Factories Act 1948 (India) and Rules — health, safety, and welfare provisions (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old man from Rajasthan is brought to the district hospital with progressive breathlessness and a dry cough over three years. He has never smoked. His wife mentions he worked for ten years in a granite stone-crushing unit. On examination you find diminished breath sounds at the right base, and a chest X-ray shows bilateral upper lobe nodular opacities with eggshell calcification of hilar nodes. His spirometry reveals a restrictive pattern. The occupational history — ten words from the family — has just given you the diagnosis that all investigations together could not have supplied. This module teaches you to read that history and to protect the next worker before the disease begins.
WHY THIS MATTERS
The World Health Organization estimates that 1.9 million deaths per year are attributable to occupational risk factors — placing occupational disease alongside major non-communicable diseases as a public health priority. In India, millions of workers in mining, construction, agriculture, textile, and chemical industries face daily hazardous exposures. As a physician you will encounter occupational illness in community clinics, rural health centres, and factory medical rooms. The ability to take a systematic occupational history, recognise sentinel diseases such as silicosis and organophosphate poisoning, and apply preventive frameworks is a core clinical and public health competency — directly relevant to CM11.1, CM11.3, and CM11.4.
RECALL
Before proceeding, recall from your basic-science years: (1) the respiratory anatomy of the lung — bronchopulmonary segments, alveolar structure, and lymphatic drainage — that determines where inhaled dust deposits and causes pneumoconiosis; (2) from Physiology, the autonomic nervous system — cholinergic receptors and the SLUD syndrome (salivation, lacrimation, urination, defaecation) that underlies organophosphate poisoning; (3) from Biochemistry, basic toxicokinetics — how lipid-soluble chemicals such as organochlorines bioaccumulate. These Year-1 foundations make the pathology of occupational disease mechanistically clear, not just memorisable.
Magnitude of Occupational Illness — A Public Health Burden
Occupational illness refers to any disease caused, exacerbated, or otherwise related to a worker's employment environment. The global burden is substantial: according to the International Labour Organization (ILO) and WHO joint estimates, work-related diseases and injuries cause approximately 2 million deaths annually, of which around 1.9 million are attributable to diseases rather than injuries. Respiratory diseases — chiefly pneumoconioses — account for the largest share of occupational deaths globally, followed by cardiovascular diseases (work-related stress, shift work, chemical exposures) and occupational cancers.
In India, the burden is disproportionately borne by workers in the unorganised sector — stone quarrying, brick kilns, gem polishing, incense-stick rolling, and small-scale agriculture — where occupational health services are absent and regulatory enforcement is weak. The National Institute of Occupational Health (NIOH), Ahmedabad, estimates that silicosis alone affects hundreds of thousands of quarry workers in Rajasthan, Gujarat, and Jharkhand. Agricultural workers, representing the largest single occupational group in India, face unique risks from pesticide exposures, biological agents (zoonoses such as leptospirosis and brucellosis), ergonomic loads from manual harvesting, and heat stress.
Occupational diseases are classified by the ILO and the Factories Act 1948 as notifiable diseases in India — certain diseases (silicosis, lead poisoning, occupational dermatitis, etc.) must be reported to the inspector of factories. Notification enables surveillance, targeted intervention, and compensation — making it a public health tool as much as a legal obligation.
IMPORTANT CONTEXTUAL NOTE: The magnitude of occupational illness in India is almost certainly an underestimate. Most occupational deaths are recorded as cause-of-death without occupational attribution (e.g. a silicosis death coded as 'pulmonary fibrosis' with no mention of mining). Building occupational history into routine clinical practice is therefore a surveillance act, not merely a clinical courtesy.
Occupational Hazard Classification and Key Disease-Agent Pairs
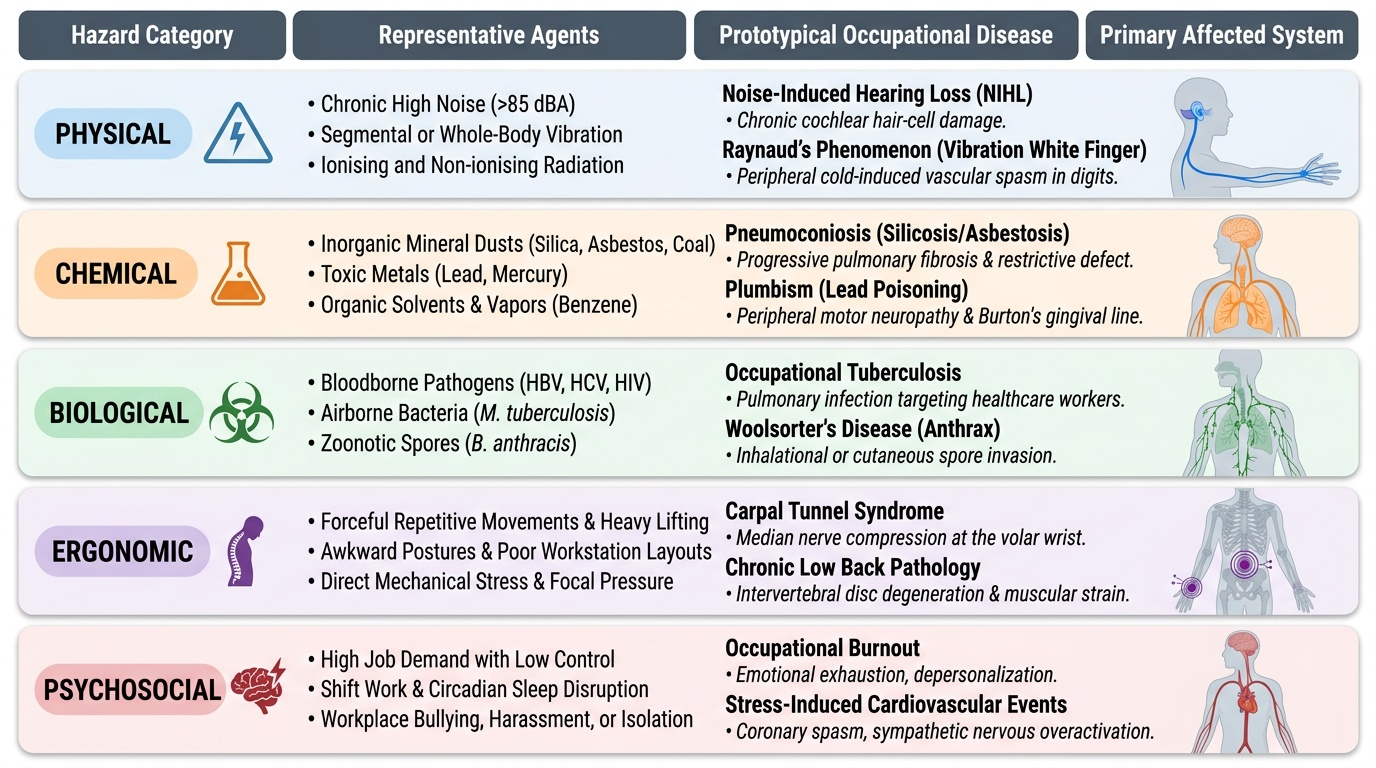
Occupational hazards are classified into five broad categories based on the nature of the harmful agent. Understanding this taxonomy helps the clinician systematically screen any workplace for risks and anticipate which disease patterns to expect.
1. Physical hazards include noise, vibration, extremes of temperature (heat and cold), non-ionising radiation (ultraviolet, infrared, microwave, laser), and ionising radiation (X-ray, gamma, alpha, beta). Noise-induced hearing loss (NIHL) — the most prevalent occupational disease globally — results from chronic exposure to sounds above 85 dB(A). Vibration causes Raynaud's phenomenon (vibration white finger) in workers using pneumatic drills; whole-body vibration causes low back pathology in transport workers.
2. Chemical hazards constitute the largest group by agent diversity. These include mineral dusts, organic dusts, metallic fumes, gases, vapours, and solvents. The major pneumoconioses arise from inorganic dust inhalation:
- Silicosis: caused by free crystalline silica (quartz) dust; affects stone cutters, quarry workers, sand-blasters, foundry workers, and gem polishers. Progressive fibrosis causes restrictive lung disease; may be complicated by tuberculosis (silicotuberculosis).
- Asbestosis: caused by asbestos fibre inhalation; affects shipyard workers, insulation workers, brake lining manufacturers. Causes diffuse interstitial fibrosis (lower zones); associated with mesothelioma and lung cancer.
- Coal Workers' Pneumoconiosis (CWP): caused by coal dust; affects underground coal miners. Ranges from simple CWP (nodules, asymptomatic) to progressive massive fibrosis.
- Byssinosis: caused by cotton dust; affects cotton gin and textile workers. Characteristically worse on the first workday after a break (Monday morning fever) — an important distinguishing feature.
Metallic hazards: Lead (plumbism) — occurs in battery manufacturing, paint stripping, printing, smelting. Presents with peripheral motor neuropathy (wrist/foot drop), colicky abdominal pain, basophilic stippling of red cells, and the Burton's lead line (blue-grey line at gum margin). Mercury — affects thermometer manufacturers, dentists (amalgam), chloralkali workers. Causes erethism (irritability, shyness, memory loss), tremor, and gingivitis. Benzene — used in petroleum refining, dye manufacturing; causes aplastic anaemia and is a recognised cause of acute myeloid leukaemia.
Agricultural chemical hazards: Organophosphate (OP) pesticides (malathion, chlorpyrifos, parathion) are the commonest occupational poisoning in Indian agriculture. They irreversibly inhibit acetylcholinesterase, causing cholinergic excess — SLUD syndrome (salivation, lacrimation, urination, defaecation), plus miosis, bradycardia, bronchospasm, and in severe cases seizures and respiratory paralysis. Organochlorine pesticides (DDT, aldrin, endrin — now largely banned) are lipophilic, bioaccumulate in adipose tissue, and cause CNS excitation and hepatotoxicity.
3. Biological hazards include bacteria, viruses, fungi, and parasites. Agriculture workers face zoonoses — brucellosis (cattle), leptospirosis (rodent-contaminated water/soil), anthrax (handling infected hides), and Q fever. Healthcare workers face bloodborne pathogen exposure (hepatitis B, hepatitis C, HIV). Farmers may develop farmer's lung — a hypersensitivity pneumonitis from inhaling thermophilic actinomycetes in mouldy hay.
4. Ergonomic hazards arise from the interface between the worker's body and the physical demands of work. They cause musculoskeletal disorders (MSDs): carpal tunnel syndrome (repetitive wrist flexion-extension in typists, assembly line workers), work-related upper limb disorders (WRULDs), low back pain (manual handling, prolonged sitting), and cervical spondylosis (sustained head postures in microscopists, jewellers).
5. Psychosocial hazards — shift work, work overload, job insecurity, workplace violence — cause stress-related disorders including hypertension, depression, and burnout.
IMPORTANT AGRICULTURAL NOTE: Agriculture is the most hazardous single industry in India by absolute disease burden. The occupational history must always ask about pesticide mixing and spraying practices (bare hands, no mask = OP exposure), type of crops, livestock contact, and water sources.
Provided image
SELF-CHECK
A cotton textile worker reports that her chest tightness is worst on Monday morning but improves by midweek. This pattern is most characteristic of:
A. Silicosis
B. Byssinosis
C. Asbestosis
D. Coal workers' pneumoconiosis
Reveal Answer
Answer: B. Byssinosis
Byssinosis, caused by cotton dust, classically presents with Monday morning fever — chest tightness and breathlessness that is worst on the first day of work after the weekend break and improves as the week progresses. Silicosis and CWP do not follow this weekly pattern. Asbestosis typically causes lower-zone fibrosis and does not have this feature.
Pneumoconioses and Chemical Occupational Diseases — Clinical Features
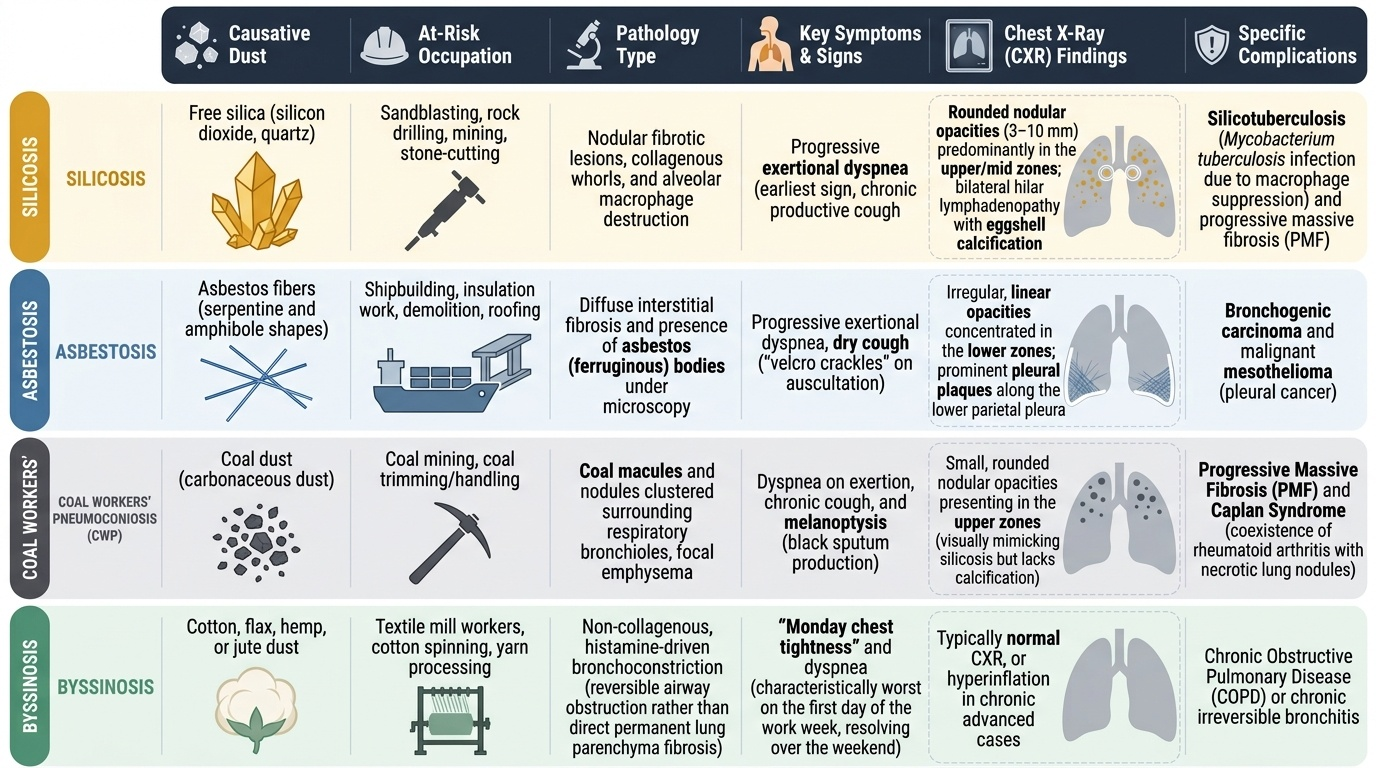
The pneumoconioses form the most recognisable group of occupational diseases and share a common diagnostic logic: a characteristic exposure history + compatible chest X-ray + appropriate clinical features. Understanding the distinguishing features of each helps avoid diagnostic confusion.
Silicosis typically has a latency of 10–20 years for chronic silicosis (acute silicosis — massive exposure, <5 years). The presenting features include progressive exertional dyspnoea (earliest), chronic productive cough, and constitutional symptoms in advanced disease. The chest X-ray is pathognomonic in advanced cases: rounded nodular opacities (3–10 mm) predominantly in the upper and mid zones, with bilateral hilar lymphadenopathy showing eggshell calcification — a finding that, when present, virtually confirms silicosis. Spirometry shows a restrictive pattern. The major complication is silicotuberculosis — silica suppresses macrophage function, creating a permissive environment for Mycobacterium tuberculosis. All silicosis patients must be screened for TB.
Asbestosis presents with progressive dyspnoea and a dry (velcro) cough. Bibasilar crackles on auscultation are characteristic. Chest X-ray shows lower-zone predominant irregular (linear) opacities — contrasting with silicosis's upper-zone nodular pattern. HRCT is more sensitive: honeycombing, traction bronchiectasis. Pleural plaques — discrete calcified areas on the parietal pleura — are the hallmark of asbestos exposure even without parenchymal disease. Mesothelioma (malignant tumour of the pleura) and bronchogenic carcinoma are the feared malignant complications. There is no reversal once fibrosis is established.
Coal Workers' Pneumoconiosis (CWP) produces rounded opacities (simpler nodules, <1 cm) in upper zones; the lung may turn grey-black (anthracosis). Progressive Massive Fibrosis (PMF) — masses >1 cm — develops in a minority and causes severe airflow obstruction. The occupational history of underground coal mining for >10 years is essential to the diagnosis.
Byssinosis is unique in being reversible early. Acute byssinosis — chest tightness, dyspnoea, and reduced FEV₁ on Monday morning — recovers by Thursday. Chronic byssinosis (prolonged exposure) produces irreversible airways obstruction mimicking chronic obstructive pulmonary disease (COPD). The biological mechanism involves endotoxin-mediated airway inflammation rather than fibrosis.
Plumbism (lead poisoning) presents along three clinical dimensions: neurological (peripheral motor neuropathy — classical wrist-drop and foot-drop from lead's selective effect on motor neurons; in children, encephalopathy), gastrointestinal (lead colic — severe colicky abdominal pain with constipation), and haematological (hypochromic microcytic anaemia with basophilic stippling of erythrocytes on blood film — fragmented ribosomal RNA). The Burton's line — a blue-grey discolouration at the gingival margin — is a classical but late sign seen when blood lead is high. Diagnosis: blood lead level (>25 µg/dL is concerning; >45 µg/dL requires chelation). Treatment: remove from exposure; dimercaprol (BAL) or succimer (DMSA) chelation for severe cases.
Mercury poisoning (mercurialism) causes the triad of erethism (a cluster of psychological changes — excessive shyness, irritability, insomnia, and memory impairment), intention tremor (starting distally, progressing centrally), and gingivitis with tooth loss. The Mad Hatter phenomenon (from hat-making using mercuric nitrate in 19th-century England) describes erethism. Organic mercury (methylmercury — Minamata disease) additionally causes cerebellar ataxia and visual field constriction.
Organophosphate poisoning (agricultural workers): muscarinic features = SLUD + miosis + bradycardia + bronchospasm; nicotinic features = fasciculations → paralysis; CNS features = anxiety, seizures, coma. The diagnostic test is plasma or RBC cholinesterase activity (markedly reduced). Treatment: remove from exposure, maintain airway, atropine (blocks muscarinic effects — large doses needed until secretions dry) + pralidoxime (regenerates cholinesterase if given early, before 'ageing' of the OP-enzyme bond).
Provided image
SELF-CHECK
A 45-year-old battery manufacturing worker presents with wrist-drop, colicky abdominal pain, and a blue-grey line at the gum margin. Blood film shows basophilic stippling. The most likely diagnosis is:
A. Mercury poisoning
B. Organophosphate poisoning
C. Lead poisoning (plumbism)
D. Benzene toxicity
Reveal Answer
Answer: C. Lead poisoning (plumbism)
The triad of peripheral motor neuropathy (wrist-drop), lead colic (severe abdominal pain), and haematological changes (basophilic stippling on blood film) together with Burton's line at the gum margin is pathognomonic of plumbism. Mercury causes erethism and tremor (not wrist-drop). Organophosphate causes cholinergic features (SLUD, miosis). Benzene causes aplastic anaemia/leukaemia without these neurological/GI features.