Page 1 of 11
CM20.1-3 | CM20.1-3 | Recent Public Health Events and Outbreak Issues — SDL Guide
Learning Objectives
- List the major public health events of the last five years at national and global levels (CM20.1)
- Describe the determinants, outbreak dynamics, and prevention strategies for recent infectious disease events (CM20.2)
- Describe significant community health events and explain their public health importance (CM20.3)
INSTRUCTIONS
The world has experienced an unprecedented cluster of public health emergencies between 2019 and 2024 — a global pandemic, re-emerging zoonoses, a growing antimicrobial resistance crisis, and India's own rapid digital health transformation. As a community physician, you will be expected not only to recall these events but to explain their epidemiological patterns, understand why they occurred, and apply outbreak-response principles in your district practice. This module builds that situational awareness and connects it to the frameworks — One Health, IDSP, ABDM, WHO IHR — that structure India's public health response.
References
- Park's Textbook of Preventive and Social Medicine, 27th ed., Ch 5 (Communicable Diseases), Ch 6 (Epidemiology of Non-Communicable Diseases), Ch 21 (Health Programmes) (textbook)
- WHO International Health Regulations 2005 (IHR 2005) (guideline)
- India Ministry of Health: Integrated Disease Surveillance Programme (IDSP) Annual Reports 2020-2024 (report)
- Ayushman Bharat Digital Mission (ABDM) Operational Guidelines, NHA 2021 (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is March 2020. You are the District Medical Officer in a Tier-2 Indian city when your morning briefing includes an unusual cluster: twelve patients in three wards of the district hospital share a strikingly similar presentation — high fever, dry cough, and oxygen saturations dropping to 88%. Three had returned from international travel the week before; the rest had no obvious link. Within 48 hours the WHO has declared COVID-19 a pandemic. Your district, like every other in India, is suddenly the front line. What does a community physician do when a global health event lands at the district gate? This module helps you answer that question — not just for COVID-19, but for the wave of outbreaks and health emergencies that have followed.
WHY THIS MATTERS
Competency CM20.1–20.3 explicitly requires Year-3 students to know the major public health events of the last five years and to describe outbreak issues and their prevention. But the deeper reason this matters is professional readiness. The next PHEIC — whether a novel respiratory pathogen, a Nipah re-emergence, or a mass antimicrobial-resistance event — will reach your district before national directives do. Community physicians who can recognise unusual event patterns, trigger the right reporting chain, and communicate clearly to communities are the first and often most critical layer of public health defence. This module gives you the factual inventory and the conceptual frameworks to act with confidence under uncertainty.
RECALL
Before we move to recent events, pause and recall three foundational concepts from earlier in your CM course. First, the epidemiological triad: host, agent, and environment interact to produce disease — every outbreak you will study in this module is ultimately a failure or perturbation in one or more of these three nodes. Second, surveillance system architecture: India's Integrated Disease Surveillance Programme (IDSP) sits at the centre of outbreak detection, with a three-tier structure (subdistrict → district → state/central) and the P (peripheral), L (laboratory), and S (syndromic) reporting forms. Third, national health programme framework: programmes like the National Vector Borne Disease Control Programme (NVBDCP) and the National TB Elimination Programme (NTEP) provide the institutional channels through which outbreak alerts are converted into coordinated responses. Keeping these three frameworks in mind will help you structure everything that follows.
The Burden of Recent Public Health Events in India and Globally
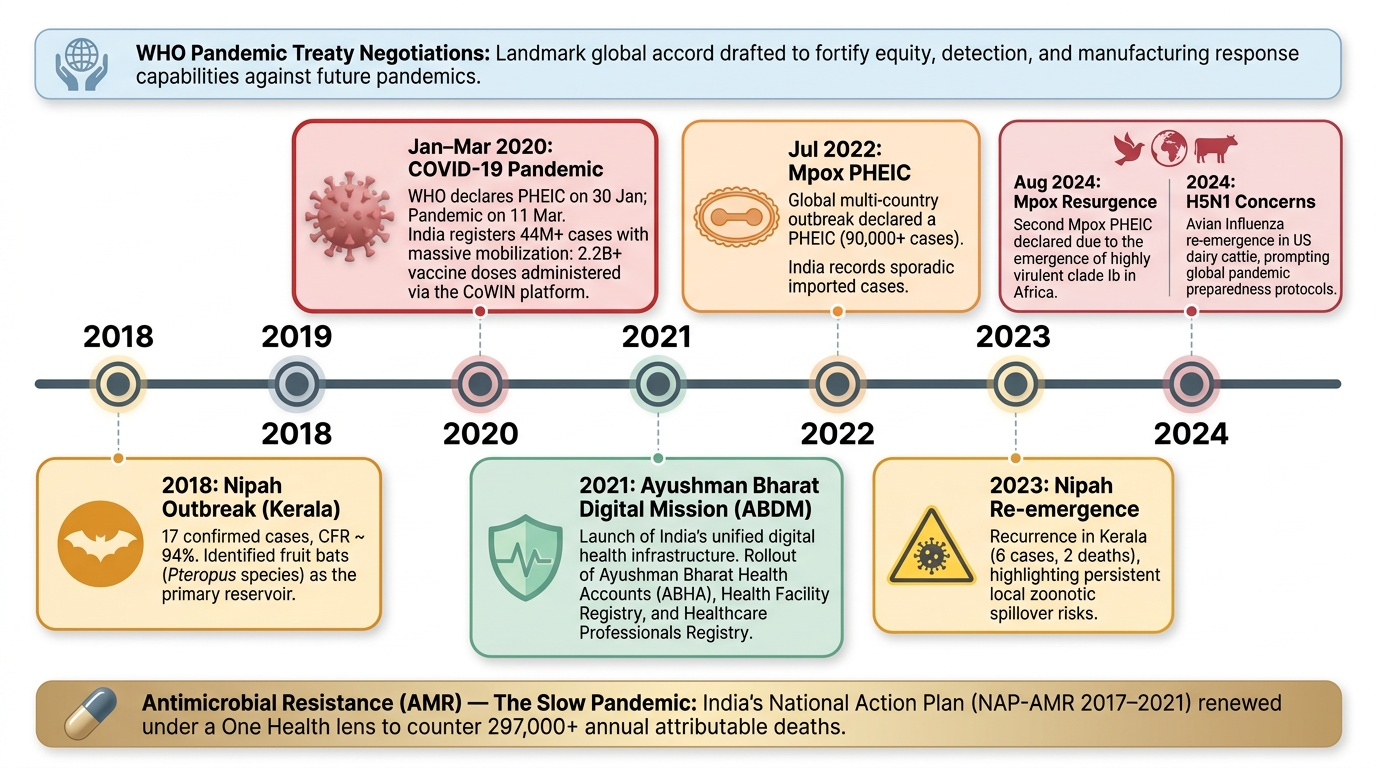
Between 2019 and 2024, the global public health landscape was reshaped by an extraordinary sequence of events. The most defining was the COVID-19 pandemic — caused by SARS-CoV-2, a novel betacoronavirus with zoonotic origins traced to Wuhan, China. The WHO declared COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020, and a pandemic on 11 March 2020. India recorded over 44 million confirmed cases and approximately 530,000 reported deaths by mid-2024, though excess mortality estimates suggest the true toll was several times higher. The pandemic triggered the largest mass vaccination drive in human history — India's CoWIN platform administered over 2.2 billion doses, including indigenous vaccines COVAXIN (Bharat Biotech) and Covishield (SII/AstraZeneca).
Beyond COVID-19, several other events demand the community physician's attention. Mpox (formerly monkeypox), caused by Monkeypox virus (genus Orthopoxvirus), was declared a PHEIC twice — in July 2022 during a multi-country outbreak (over 90,000 cases globally), and again in August 2024 following the emergence of clade Ib in Africa. India reported sporadic imported cases. Nipah virus caused outbreaks in Kerala in 2018 (17 cases, CFR 94%) and 2023 (6 cases, 2 deaths), underscoring the continued zoonotic threat from fruit bats (Pteropus species). H5N1 avian influenza re-emerged globally in cattle in the United States in 2024, raising pandemic preparedness concerns. On the programmatic front, India's Ayushman Bharat Digital Mission (ABDM), launched in 2021, represents one of the most significant public health infrastructure events of the decade — creating a national digital health ecosystem with Ayushman Bharat Health Accounts (ABHA), the Health Facility Registry, and the Healthcare Professionals Registry, all aimed at transforming surveillance and continuity of care. Antimicrobial resistance (AMR) continues as a slow pandemic: India bears one of the highest burdens globally, with an estimated 297,000 deaths attributable to AMR in 2019 (ICMR surveillance data), and the National Action Plan on AMR (India NAP-AMR 2017–2021) has been renewed under a One Health lens.
Provided image
For a community physician, the key skill is not memorising each event in isolation but recognising common patterns: the WHO PHEIC declaration as the international alert threshold, the unusual cluster signal as the local detection mechanism, and the One Health framework as the explanatory lens for why most modern outbreaks begin at the human-animal-environment interface.
| Event | Period | Causative Agent | India Relevance |
|---|---|---|---|
| COVID-19 pandemic | 2019–ongoing | SARS-CoV-2 (betacoronavirus) | 44M+ cases; largest vaccination drive |
| Mpox multi-country | 2022, 2024 | Monkeypox virus (Orthopoxvirus) | Sporadic imported cases; watch in MSM |
| Nipah Kerala | 2018, 2023 | Nipah virus (Henipavirus) | Fruit bat reservoir; CFR up to 94% |
| H5N1 avian influenza | 2024 | Influenza A/H5N1 | Pandemic preparedness alert |
| AMR (ongoing) | 2019–2024 | Multiple pathogens | 297,000 attributable deaths (India 2019) |
| ABDM launch | 2021 | — (programmatic) | ABHA IDs, digital surveillance infrastructure |
SELF-CHECK
Which of the following statements about the mpox (formerly monkeypox) PHEIC declarations is CORRECT?
A. WHO declared mpox a PHEIC once — in July 2022 — and has not repeated the declaration
B. WHO declared mpox a PHEIC twice — in July 2022 and again in August 2024 following clade Ib emergence in Africa
C. Mpox was declared a pandemic (not a PHEIC) in 2022 because it spread across more than 10 countries
D. India declared mpox a national health emergency in 2022 following community transmission
Reveal Answer
Answer: B. WHO declared mpox a PHEIC twice — in July 2022 and again in August 2024 following clade Ib emergence in Africa
WHO declared mpox a PHEIC twice: first in July 2022 (multi-country clade IIb outbreak, >90,000 cases globally) and again in August 2024 following the emergence of the more severe clade Ib in the Democratic Republic of Congo and neighbouring countries. A PHEIC is not the same as a pandemic declaration. India reported sporadic imported cases but no declared national emergency.
Determinants of Modern Outbreak Emergence
Understanding why these outbreaks occurred requires moving beyond the isolated event to the structural determinants that make the modern world increasingly vulnerable to infectious disease emergence. The One Health framework, formalised by the WHO-FAO-UNEP-WOAH Quadripartite in 2022, provides the most rigorous explanatory lens: it holds that human health, animal health, and environmental health are inextricably linked, and that outbreak emergence is most often a failure at one or more of these interfaces.
The dominant driver of emerging infectious disease in the 21st century is zoonotic spillover — the crossing of a pathogen from an animal reservoir into the human population. An estimated 60–70% of emerging infections are zoonotic in origin (Park, 27th ed). The Nipah virus outbreak in Kerala illustrates the pathway clearly: Pteropus (fruit bat) populations harbouring Nipah virus have expanded their range partly due to deforestation, which brings bats into contact with date palm sap collection sites and domestic animals. Human encroachment into bat habitats, driven by agricultural expansion, increases exposure. COVID-19 similarly emerged from a bat reservoir (with a likely intermediate host) in the context of a wildlife market with poor biosafety controls.
Climate change is an increasingly important determinant. Rising temperatures have expanded the geographic range of Aedes aegypti (dengue, chikungunya, Zika) and Anopheles mosquitoes (malaria) into previously non-endemic highland areas of India. Extreme weather events — cyclones, floods — displace populations, overwhelm sanitation systems, and create conditions for cholera and leptospirosis. The IPCC and WHO project a continued increase in climate-sensitive disease burden, with India as a high-vulnerability country given its large rural population and climate-exposed geography.
Antimicrobial resistance is the third major determinant class — what is sometimes called the 'silent pandemic'. Inappropriate antibiotic use in humans, agricultural overuse (approximately 70% of all antibiotics are used in food animals globally), and poor wastewater treatment create selective pressure that drives resistance. When an outbreak occurs against a background of AMR, therapeutic options narrow and case fatality rates rise.
Globalisation and rapid transit ensure that once a pathogen breaches the zoonotic barrier, it can reach any city on the planet within 24–36 hours. This is the core argument for the WHO International Health Regulations 2005 (IHR) — the global legal framework that obligates member states to build core surveillance capacities and report events that may constitute PHEICs. India is a signatory to IHR 2005 and has built IDSP as its primary IHR compliance mechanism.
| Outbreak | Primary Determinant | One Health Failure Domain | Amplifying Factor | |
|---|---|---|---|---|
| COVID-19 | Zoonotic spillover (bat/pangolin) | Human-animal interface | Global air travel, delayed reporting | |
| Nipah Kerala | Fruit bat habitat encroachment | Human-animal interface | Healthcare amplification (nosocomial) | |
| Mpox 2022 | Sexual network transmission | Human-human | Cessation of smallpox vaccination (1980) | |
| AMR | Antibiotic overuse (human+animal) | Human-animal-environment | Agricultural antibiotic use | |
| Dengue surge | Climate-driven vector expansion | Environment | Urbanisation, water storage practices |
Outbreak Response and Prevention Strategies
Knowing that an outbreak is occurring is only the first step. The community physician must understand the response and prevention architecture that translates detection into control. India's primary tool is the Integrated Disease Surveillance Programme (IDSP), launched in 2004 and significantly strengthened after COVID-19. IDSP operates through a three-tier structure: Subdistrict Surveillance Units (SSU), District Surveillance Units (DSU), and State/Central Surveillance Units. The programme uses three reporting formats — P forms (peripheral/community health workers reporting syndromes weekly), L forms (laboratory confirmed cases), and S forms (syndromic reports from health facilities). Any unusual clustering of cases triggers a Rapid Response Team (RRT) — a multidisciplinary team of epidemiologist, clinician, microbiologist, and district health officer — tasked with field investigation within 24–48 hours of alert.
The international framework is the WHO International Health Regulations 2005 (IHR 2005), the legally binding global instrument that establishes core surveillance and response capacities for 196 member states. Under IHR, India must notify WHO within 24 hours of any event that may constitute a PHEIC. WHO assesses notifications using a decision algorithm based on four criteria: seriousness of public health impact, unusualness or unexpectedness, potential for international spread, and potential for travel or trade restrictions. The IHR framework is evaluated through the Joint External Evaluation (JEE) tool, which scores countries across 19 technical areas including surveillance, laboratory capacity, and emergency response operations.
Specific outbreak control strategies vary by pathogen but share common elements. Isolation and case management reduce onward transmission from confirmed cases. Contact tracing identifies exposed individuals before they develop symptoms — this was operationalised at massive scale during COVID-19 via the Aarogya Setu app (integrated with ABDM). Ring vaccination is the preferred strategy when vaccine supply is limited and the outbreak is geographically concentrated (used for mpox in 2022 and for Ebola historically). Infection Prevention and Control (IPC) protocols protect healthcare workers, who are particularly vulnerable in high-CFR outbreaks like Nipah. Risk communication — accurate, timely, and culturally appropriate messaging — prevents the parallel epidemic of misinformation, which has been documented to cause as much harm as the pathogen itself in modern outbreaks.
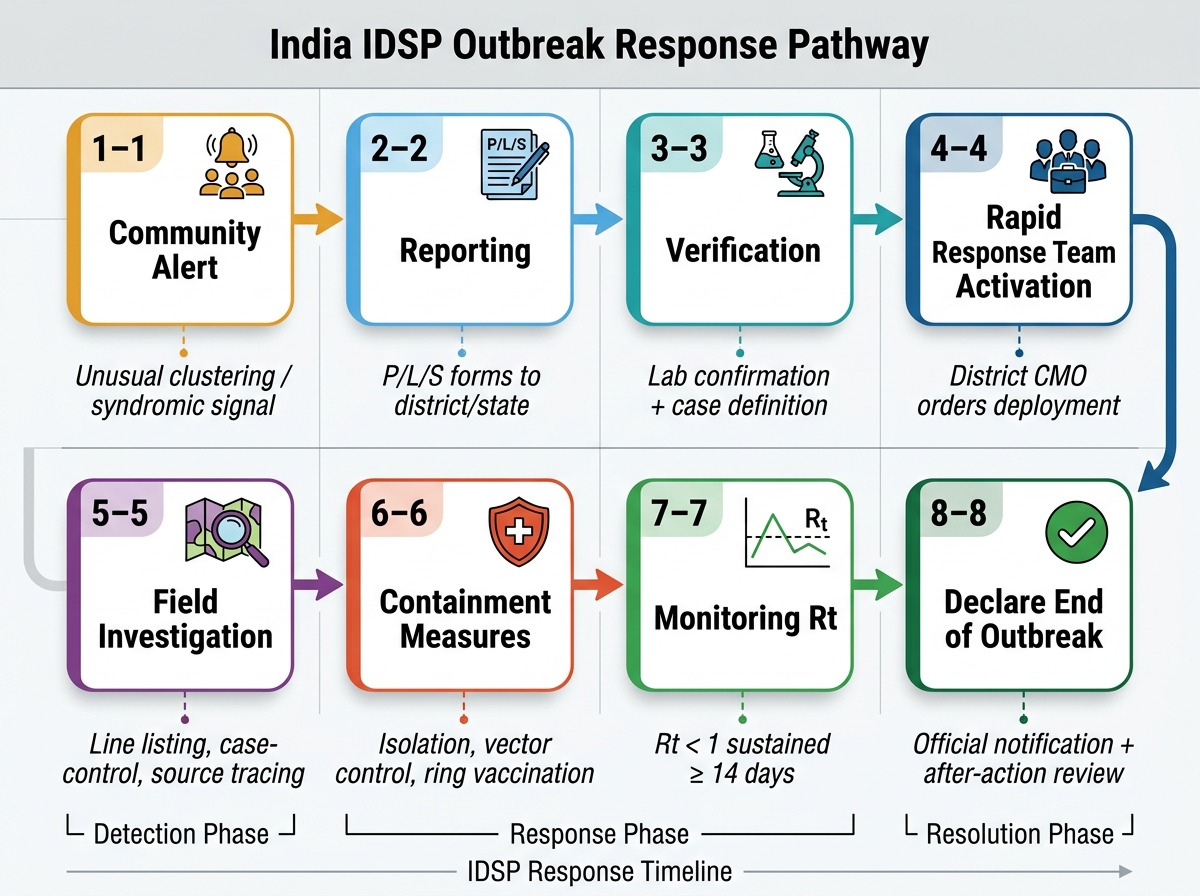
India IDSP Outbreak Response Pathway: Eight-Step Framework
Digital tools have transformed outbreak response. ABDM's ABHA-linked health records allow rapid identification of vulnerable populations. The IHIP platform (Integrated Health Information Platform, the upgraded IDSP) enables near-real-time national surveillance dashboards. CoWIN's vaccination tracking infrastructure was repurposed for COVID-19 but its architecture is now available for future outbreak vaccination campaigns. These tools collectively represent what Park describes as 'surveillance 2.0' — a shift from passive, periodic reporting to active, continuous, digital surveillance.
SELF-CHECK
A Rapid Response Team (RRT) under India's IDSP is activated when:
A. Any single case of a notifiable disease is confirmed by a laboratory
B. An unusual clustering of cases is identified, suggesting a potential outbreak beyond expected baseline
C. The district records more than 100 reported syndromes in a single P-form submission
D. A new pathogen with no prior Indian documentation is isolated from a clinical sample
Reveal Answer
Answer: B. An unusual clustering of cases is identified, suggesting a potential outbreak beyond expected baseline
The RRT trigger under IDSP is an unusual clustering of cases — a signal that exceeds the expected baseline in time, place, or person, suggesting a potential outbreak. It does not require laboratory confirmation as the trigger (that would delay response); instead, the RRT investigates to establish whether a true outbreak exists and to characterise the pathogen. A single confirmed notifiable disease case may generate a case report but not automatically an RRT dispatch. The RRT aims to reach the field within 24–48 hours of the alert.