Page 4 of 11
CM20.4 | CM20.4 | Community Medicine Practice Laws — SDL Guide
Learning Objectives
- Demonstrate awareness of the major laws that govern community medicine practice in India (CM20.4)
- Identify the legal framework applicable to key situations: informed consent, mandatory notification, PCPNDT compliance, epidemic duty, and consumer complaints
- Apply medico-legal principles to prevent negligence and ensure professional accountability in community health settings
INSTRUCTIONS
Community medicine practice does not happen in a legal vacuum. Every clinic decision — from how you document a patient encounter to whether you report a notifiable disease, from whether you conduct a third-trimester termination to how you respond during an epidemic — is governed by a web of statutes, court decisions, and regulatory frameworks. A community physician who is unaware of these laws is not just professionally vulnerable; they may inadvertently harm patients, enable rights violations, or fail in public health duties. This module maps the legal terrain you will navigate as a community medicine practitioner.
References
- Park's Textbook of Preventive and Social Medicine, 27th ed., Ch 23 (Health Administration), Ch 24 (Health Legislation) (textbook)
- National Medical Commission Act, 2020 (Government of India) (legislation)
- Consumer Protection Act, 2019 (Government of India) (legislation)
- Medical Termination of Pregnancy (Amendment) Act, 2021 (legislation)
- Epidemic Diseases Act, 1897 (as amended 2020) (legislation)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Priya is a 32-year-old medical officer at a Primary Health Centre in rural Maharashtra. One Monday morning she faces three situations in quick succession: a patient's family demands to know the sex of the foetus during a routine ultrasound scan; a local politician asks her to suppress the weekly IDSP P-form to avoid 'creating panic' about a gastroenteritis cluster; and a colleague tells her a patient has filed a consumer complaint in the District Consumer Forum alleging negligence in a delivery that resulted in a stillbirth. Three situations — three different laws — and potentially three career-defining decisions. Dr Priya, like many community physicians, received no formal training in medico-legal awareness. This module gives you what she did not have.
WHY THIS MATTERS
Competency CM20.4 requires you to demonstrate awareness about laws pertaining to the practice of community medicine. But the practical stakes go beyond exam recall. The consumer protection case load against doctors in India has increased substantially in the last decade, with the National Consumer Disputes Redressal Commission receiving hundreds of medical negligence complaints annually. Healthcare workers have faced criminal prosecution for alleged negligence. The Epidemic Diseases Act 1897 — dormant for a century — was invoked repeatedly during COVID-19. PCPNDT prosecutions have led to imprisonment of doctors who conducted prenatal sex determination. Understanding these laws is professional self-protection, patient rights operationalisation, and public health duty all at once.
RECALL
Before entering the legislative detail, recall three foundational concepts. First, the structure of Indian health administration: the Union Government holds concurrent jurisdiction with states on matters of public health under Schedule VII of the Constitution; both Parliament and State Legislatures may pass health legislation, which is why some laws are central (NMC Act, MTP Act) and others may have state variations (Clinical Establishments). Second, public health ethics: the four principles of biomedical ethics — autonomy, beneficence, non-maleficence, and justice — underpin much of health legislation. The PCPNDT Act prioritises justice (correcting sex ratio) over pure autonomy; the MTP Act balances foetal potential moral status against maternal autonomy. Third, the concept of standard of care: a community physician is expected to practise at the standard of a reasonable medical professional in similar circumstances (the Bolam principle from English law, applied in Indian courts). Understanding this standard is the baseline for understanding what constitutes negligence.
Burden of Medico-Legal Issues in Community Medicine Practice
The medico-legal landscape facing community physicians in India has transformed fundamentally over the last three decades, and understanding the magnitude of this change is the first step toward navigating it safely. The landmark Indian Medical Association vs V.P. Shantha (1995) Supreme Court ruling established that medical services fall within the definition of 'service' under the Consumer Protection Act — meaning that patients who allege deficiency in medical service may sue doctors in civil consumer forums without needing to go through the criminal courts. This single ruling opened a flood of consumer complaints: by the 2010s, thousands of medical negligence cases were being filed annually across District, State, and National Consumer Forums.
The burden is not symmetrical across specialties or settings. Community physicians — particularly those working in public health centres, during epidemic response, or in maternal health settings — face specific legal pressures. Maternal death complaints (inadequate antenatal monitoring, missed high-risk pregnancy, delayed referral) constitute a significant portion of primary care-level consumer cases. Epidemic duty situations — where a community physician may be required to isolate patients, restrict movement, or report disease patterns that community members resist — have their own legal framework and their own liability risks when that framework is violated. Prenatal diagnosis at PHC level (where ultrasound machines are now common) creates PCPNDT compliance obligations that, if not met, result in criminal prosecution rather than civil liability.
Beyond civil consumer complaints, community physicians face criminal liability in cases of gross negligence. The Jacob Mathew vs State of Punjab (2005) Supreme Court ruling is the governing precedent for criminal medical negligence in India: it established that a medical professional can be prosecuted under Section 304A IPC (causing death by negligence) only when the negligence is 'gross, culpable, or reckless' — mere error of judgment or insufficient skill does not amount to criminal negligence. However, the bar, while high, is not insurmountable, and community settings — where systemic resource constraints may force suboptimal care — are precisely the environments where the distinction between 'system failure' and 'doctor negligence' gets litigated.
Healthcare worker violence is a separate dimension of medico-legal burden. The 2020 amendment to the Epidemic Diseases Act specifically added provisions criminalising attacks on healthcare workers during epidemic duty — with imprisonment up to 7 years for causing grievous hurt and up to 5 years for obstruction. This was a direct legislative response to documented violence against healthcare workers during COVID-19 and preceding outbreaks, but the practical enforceability at PHC level remains an open question.
SELF-CHECK
The landmark Supreme Court ruling that brought medical services under the Consumer Protection Act was:
A. Jacob Mathew vs State of Punjab (2005) — established that doctors owe a duty of care to patients
B. Indian Medical Association vs V.P. Shantha (1995) — established that medical services constitute 'service' under the Consumer Protection Act
C. Parmanand Katara vs Union of India (1989) — established the right to emergency medical care
D. Vincent Panikurlangara vs Union of India (1987) — established the right to safe medicines
Reveal Answer
Answer: B. Indian Medical Association vs V.P. Shantha (1995) — established that medical services constitute 'service' under the Consumer Protection Act
Indian Medical Association vs V.P. Shantha (1995) was the foundational Supreme Court ruling that held medical services (including free services in government hospitals, with a nuanced caveat) fall within the definition of 'service' under the Consumer Protection Act 1986, making doctors liable to consumer complaints. Jacob Mathew (2005) addressed criminal negligence (Section 304A IPC). Parmanand Katara (1989) is the right to emergency care. Vincent Panikurlangara (1987) related to the right to safe medicines under Article 21.
Determinants of the Current Medico-Legal Landscape
The dramatic expansion of medico-legal complexity in Indian community medicine is not random — it reflects identifiable social, economic, and political determinants that a community physician must understand to navigate the landscape effectively and advocate for systemic change where individual compliance is insufficient.
The most fundamental determinant is patient and community empowerment. Rising literacy, smartphone access to medical information, and a cultural shift from deferential to transactional relationships with doctors have increased patients' willingness to question clinical decisions and pursue legal redress. The same forces that make patients better advocates for their own health — access to information, awareness of rights, community networks — also fuel litigation when those expectations are not met.
Commercialisation of healthcare is the second major determinant. When patients pay significant out-of-pocket costs for private care (India's out-of-pocket expenditure as a percentage of total health expenditure remains among the highest in Asia), they bring correspondingly high expectations of outcomes. Adverse outcomes that might be accepted as inherent risk in a publicly funded system feel like 'deficiency of service' when significant money has changed hands. Even in public facilities, the consumer protection framework applies: the V.P. Shantha ruling explicitly noted that services available to the public free of charge or partly subsidised are covered under the Act.
Legislative modernisation is the third determinant. The Consumer Protection Act 2019 (replacing the 1986 Act) introduced significant changes: it created the Central Consumer Protection Authority (CCPA) with powers to recall products and impose penalties; it introduced provisions for product liability (relevant for medical devices and drugs); it empowered e-commerce regulation (relevant for telemedicine, which has grown significantly post-COVID under the Telemedicine Practice Guidelines 2020). The NMC Act 2020 replaced the Indian Medical Council Act 1956 and reorganised professional self-regulation under the National Medical Commission, with greater government representation and new mechanisms for medical ethics enforcement.
Digital health and telemedicine are emerging determinants. The Ministry of Health's Telemedicine Practice Guidelines 2020 (the first such guidelines in India, issued during COVID-19 lockdown) established the legal framework for virtual consultations, including which types of prescriptions are permissible via telemedicine, documentation requirements, and the requirement that the physician be registered with a State Medical Council. As ABDM enables telemedicine at scale, the medico-legal framework for remote community medicine practice is still evolving — but the burden on community physicians to understand and comply with it is already real.
Finally, legislative gaps and overlaps between central and state laws create compliance complexity. The Clinical Establishments (Registration and Regulation) Act 2010 is a central law but applies to states only on adoption — several states have their own parallel registration regimes. This fragmentation means community physicians working across state boundaries or in institutions that span multiple regulatory frameworks must navigate different compliance requirements.
Key Laws Governing Community Medicine Practice
The legislative framework governing community medicine practice in India spans five domains. Understanding the core provision and the community physician's specific obligation under each is essential for safe practice.
1. Professional Regulation: NMC Act 2020. The National Medical Commission Act 2020 replaced the Indian Medical Council Act 1956, creating a new apex regulatory body — the National Medical Commission (NMC) — with four autonomous boards: the Under-Graduate Medical Education Board (UGMEB), Post-Graduate Medical Education Board (PGMEB), Medical Assessment and Rating Board (MARB), and Ethics and Medical Registration Board (EMRB). The EMRB is the body that handles professional misconduct complaints and can suspend or cancel registration. Community physicians must ensure they are registered with their State Medical Council (maintained under EMRB oversight) and understand what constitutes 'professional misconduct' (unethical advertising, fee-splitting, sexual misconduct with patients, intoxication during duty).
2. Consumer and Negligence Law: Consumer Protection Act 2019 + IPC. Under the Consumer Protection Act 2019, a patient alleging deficiency in medical service may file a complaint with the appropriate Consumer Forum — District Commission for claims under Rs 1 crore, State Commission for claims between Rs 1-10 crore, and National Commission for claims above Rs 10 crore. The 2019 Act strengthened consumer rights with e-filing, mediation, and product liability provisions. Criminal negligence is governed by Section 304A IPC — applicable only when negligence is gross and reckless (Jacob Mathew standard). The key protective measure for community physicians is meticulous informed consent documentation and complete medical record keeping, both of which serve as primary evidence in consumer and criminal proceedings.
3. Maternal and Reproductive Law: MTP Act 1971 (amended 2021) and PCPNDT Act 1994. The Medical Termination of Pregnancy Act permits termination up to 20 weeks of gestation with opinion of one registered medical practitioner; between 20 and 24 weeks for special categories (survivors of rape or sexual assault, minors, differently-abled women, change in marital status, foetal malformations) with opinion of two registered practitioners; and beyond 24 weeks only for substantial foetal abnormality, with approval by a Medical Board constituted by the state government. The Pre-Conception and Pre-Natal Diagnostic Techniques (PCPNDT) Act 1994 bans sex determination for non-medical purposes, requires mandatory registration of all facilities with ultrasound machines with the district Appropriate Authority, mandates consent forms for every prenatal diagnostic procedure, and prohibits communicating the foetal sex to any person. Violations attract criminal prosecution — imprisonment up to 5 years and fine up to Rs 10,000 for first offence.
4. Public Health Emergency Law: Epidemic Diseases Act 1897 (amended 2020). The Epidemic Diseases Act 1897 — India's oldest public health emergency legislation — grants state governments power to issue special measures during epidemics, including mandatory quarantine, isolation, inspection of travellers, and detention of persons suspected of harbouring a dangerous disease. The 2020 amendment added central government powers to provide assistance during epidemics, and introduced provisions specifically criminalising violence against healthcare workers: imprisonment up to 7 years for causing grievous hurt to a healthcare worker during epidemic duty and up to 5 years for obstruction, harassment, or damage to property. Community physicians deployed during epidemic response are protected persons under this Act.
5. Drug, Tobacco, and Environment Laws. The Drugs and Cosmetics Act 1940 regulates the import, manufacture, distribution, and sale of drugs — community physicians need awareness of Schedule H (prescription-only drugs), Schedule H1 (antibiotics and other high-risk drugs requiring additional monitoring), and the prohibition on dispensing without valid prescription. COTPA 2003 (Cigarettes and Other Tobacco Products Act) prohibits smoking in public places (Section 4), bans tobacco advertisement (Section 5), prohibits sale to persons under 18 years (Section 6), and mandates pictorial health warnings covering at least 85% of the principal display area of tobacco product packages (Section 7). Community physicians have a role in enforcement reporting and patient counselling under COTPA. The Clinical Establishments (Registration and Regulation) Act 2010 requires all clinical establishments (government and private) to be registered and to provide minimum standard of facilities.
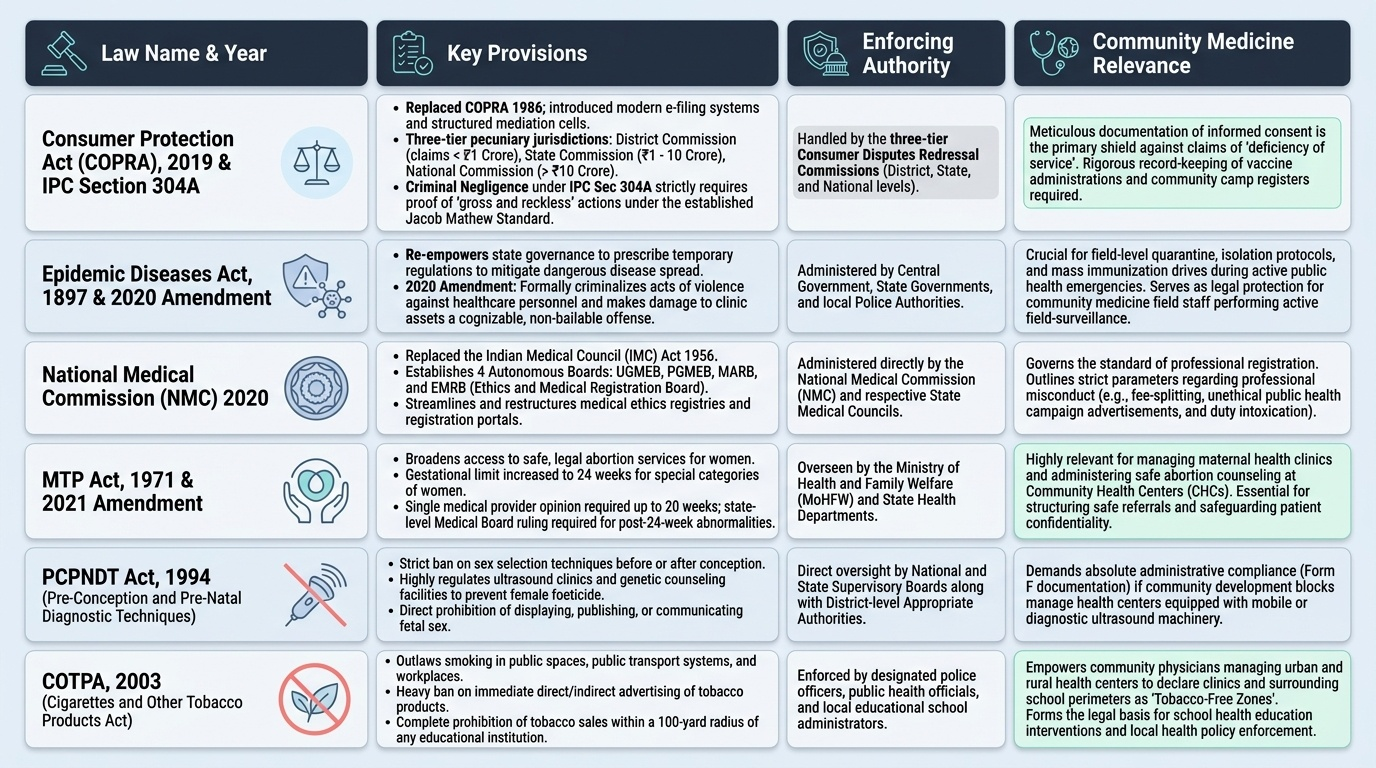
Provided image
| Law | Year | Key Provision | Enforcing Authority | Community Medicine Relevance |
|---|---|---|---|---|
| Consumer Protection Act | 2019 | Medical services = 'service'; three-tier forums | District/State/National Consumer Commission | Consumer complaints for negligence |
| NMC Act | 2020 | EMRB handles professional misconduct; registration | Ethics and Medical Registration Board | Registration, professional conduct |
| MTP Act | 1971/2021 | Gestational limits; special categories up to 24w | RMP + Medical Board for >24w | Termination of pregnancy services |
| PCPNDT Act | 1994 | Bans prenatal sex determination; mandatory registration | Appropriate Authority (district) | PHC ultrasound compliance |
| Epidemic Diseases Act | 1897/2020 | State/central epidemic powers; protects HCW | State/Central Government | Epidemic duty, HCW protection |
| COTPA | 2003 | No smoking in public places; ban on tobacco ads | State/district authorities | Tobacco cessation counselling |
SELF-CHECK
Under the Medical Termination of Pregnancy (Amendment) Act 2021, termination of pregnancy between 20 and 24 weeks of gestation is PERMITTED for which of the following categories?
A. Any woman who requests it, with a single registered medical practitioner's opinion
B. Special categories including survivors of sexual assault, minors, and differently-abled women, with opinion of two registered medical practitioners
C. Only when the foetus has a lethal anomaly, confirmed by a Medical Board constituted by the state government
D. Any married woman who requests it at any gestational age, with one registered medical practitioner's opinion
Reveal Answer
Answer: B. Special categories including survivors of sexual assault, minors, and differently-abled women, with opinion of two registered medical practitioners
The MTP (Amendment) Act 2021 permits termination between 20-24 weeks for special categories: survivors of rape or sexual assault, minors, women with disability, change in marital status (widowhood, divorce), or foetal malformations. Two registered medical practitioners' opinions are required. Beyond 24 weeks, only foetal anomalies incompatible with life or severely disabling are permitted — with a Medical Board's approval. Any woman (not just special categories) can terminate up to 20 weeks with one RMP's opinion. There is no upper gestational limit for foetal anomalies, but the bar is very high.