Page 5 of 27
CM10.3 | CM10.3 | Pregnancy, Childbirth and Feeding Practices — SDL Guide (Part 2)
Childbirth Practices and Postnatal Customs
The period of delivery and the first 28 neonatal days concentrate the highest density of harmful traditional practices. Home delivery by an untrained dai remains common in remote areas despite Janani Suraksha Yojana incentives: dais typically lack skill in recognising prolonged labour, managing shoulder dystocia, or providing neonatal resuscitation; their primary risk is delayed referral. The Clean Delivery Kit (CDK) — containing a sterilised blade, cord clamp or tie, a plastic sheet, soap, and cord dressing — represents the minimum harm-reduction tool for planned home deliveries; the dai or ASHA should use the CDK every time. Cord-cutting and stump care: applying cow dung, ash, mud, or engine oil to the cord stump is the primary driver of neonatal tetanus in areas where it still occurs. The recommended practice is dry cord care (clean and dry, nothing applied to the stump). Denial of colostrum is practised in many communities (particularly in UP, Bihar, Rajasthan, and tribal belts of central India): the yellowish first milk is called 'dirty,' 'stale,' or 'beestings' and is discarded for the first 2-3 days. This removes the infant's primary passive immune protection in the most vulnerable window. Prelacteal feeding — giving honey, animal milk, sugar water, or rice water before the first breastfeed — is associated with higher rates of early neonatal infections and delays the establishment of adequate maternal milk supply. Oil massage of the newborn (mustard oil, coconut oil) is a near-universal practice: topical mustard oil may disrupt the neonatal skin barrier and increase transepidermal water loss, while coconut oil has a neutral-to-beneficial skin-conditioning effect; this is an area where advocacy should target mustard oil specifically while affirming the tactile stimulation benefit of any gentle massage. Seclusion of the mother: in some communities the mother is confined to a separate room for 40 days postnatally, which may limit her access to health workers during the highest-risk period for puerperal sepsis and neonatal infection.
SELF-CHECK
According to WHO recommendations, when should complementary foods be introduced for a breastfed infant?
A. At 4 months, when the infant shows readiness signs
B. At 6 completed months, alongside continued breastfeeding
C. At 9 months, because the gut is immature before that
D. Only at 12 months, to maximise exclusive breastfeeding benefit
Reveal Answer
Answer: B. At 6 completed months, alongside continued breastfeeding
WHO recommends exclusive breastfeeding for the first 6 completed months, with introduction of complementary foods at exactly 6 months alongside continued breastfeeding up to 2 years or beyond. Introduction before 6 months (even at 4-5 months) increases infection risk because gut closure is incomplete and the infant's immune system is not ready. After 6 months, breast milk alone cannot meet growing energy and micronutrient needs, so complementary foods become essential.
Breastfeeding and Child Feeding Practices
Optimal infant and young child feeding (IYCF) is one of the most evidence-backed interventions in global health: appropriate breastfeeding alone could prevent an estimated 13% of all under-5 deaths globally. Colostrum — the thick, yellow fluid produced in the first 2-3 days — contains high concentrations of secretory IgA (the primary mucosal immune antibody), lactoferrin (an antimicrobial protein), oligosaccharides (prebiotics that establish the neonatal microbiome), and fat-soluble vitamins, especially vitamin A. Denying colostrum removes all of these benefits simultaneously. The WHO IYCF recommendations are: (1) Early initiation of breastfeeding within 1 hour of birth — India's NFHS-5 rate is 41.8%, well below the 70% target; early initiation reduces all-cause neonatal mortality by 19-22% in community trials. (2) Exclusive breastfeeding for the first 6 completed months — meaning only breast milk, no water, juice, or other foods; India's NFHS-5 exclusive breastfeeding rate is 63.7%. (3) Complementary feeding beginning at exactly 6 months, with continued breastfeeding up to 2 years or beyond — complementary foods must be timely (not too early, not too late), adequate in energy and micronutrients, safe (prepared hygienically), and responsive (fed by a caregiver who responds to hunger cues). India's NFHS-5 minimum adequate diet coverage for children 6-23 months is only 11.3% — a critical gap. Traditional weaning practices include abrupt removal of the breast (sometimes with bitter substances applied to the nipple) and rapid replacement with diluted animal milk or water-based gruel; abrupt weaning causes psychological distress and accelerates the transition to nutritionally inadequate diets.
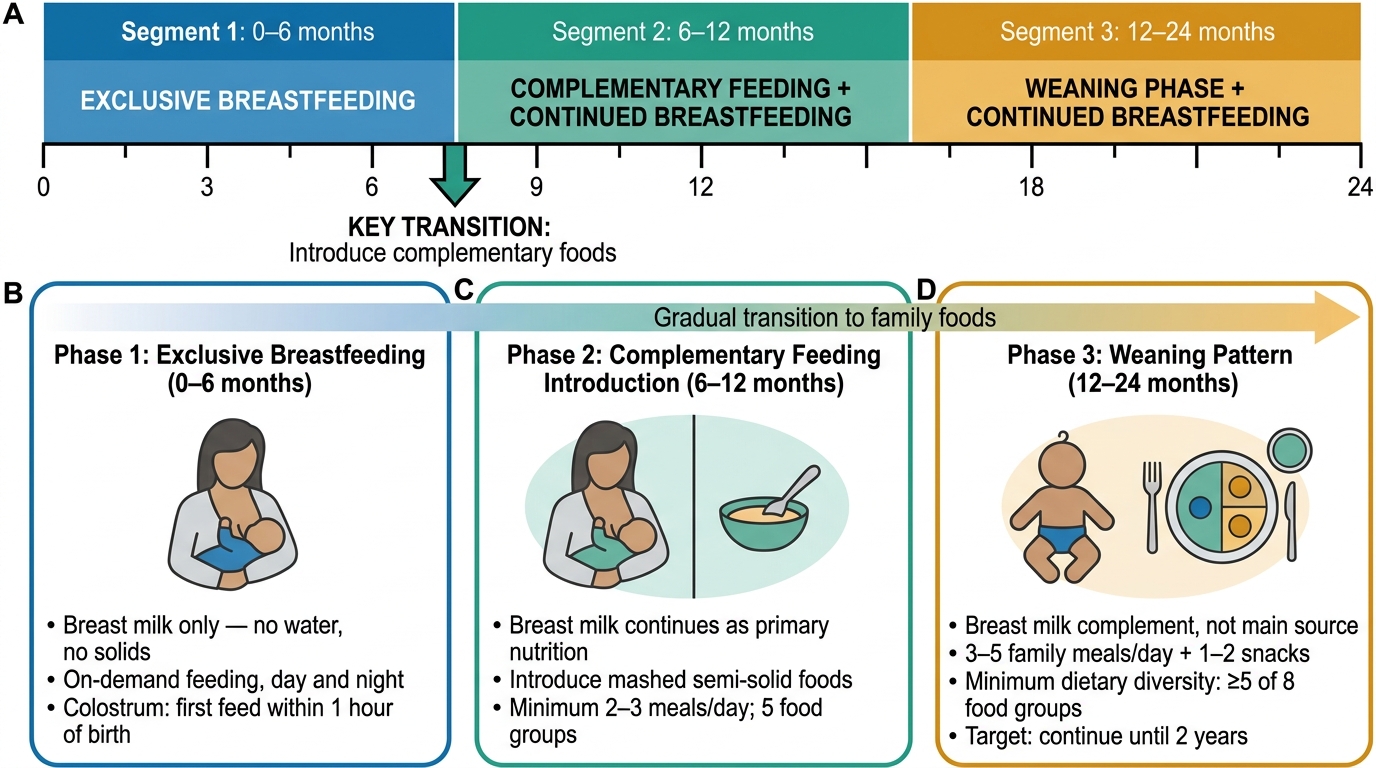
Recommended Infant and Young Child Feeding (IYCF) Timeline: Birth to 24 Months
Monitoring and Evaluation of Feeding Practice Interventions
Changing infant feeding practices requires sustained community-level intervention and measurable tracking to determine whether counselling is working. The primary HMIS and NFHS indicators used to monitor IYCF in India are: (i) early initiation of breastfeeding rate (target: ≥70%); (ii) exclusive breastfeeding rate in children under 6 months (target: ≥70%); (iii) continuation of breastfeeding at 1 year; (iv) minimum meal frequency (number of times a day a child 6-23 months is fed solid or semi-solid foods); (v) minimum dietary diversity (receives foods from ≥5 of 8 food groups in the previous 24 hours); and (vi) minimum adequate diet (a composite of meal frequency and dietary diversity). These indicators are collected routinely through ASHA registers (the HBNC and IYCF register), AWW records (the Anganwadi growth register), and periodically through NFHS rounds. The MAA (Mothers' Absolute Affection) programme is the GOI's flagship IYCF initiative: it trains ANMs and ASHAs in counselling technique, creates lactation support counsellors at community health facilities, and uses mass media campaigns to change social norms around colostrum denial and prelacteal feeding. POSHAN Abhiyaan (National Nutrition Mission, 2018) integrates IYCF monitoring into its convergence dashboard, tracking progress toward reducing stunting by 2% per year and anaemia by 3% per year.
CLINICAL PEARL
When counselling a family about colostrum, avoid the word 'dirty' — even to refute it. Repeating the negative label ('colostrum is NOT dirty') activates the negative frame in the listener's mind. Instead, use positive framing: 'This yellow milk is your baby's first vaccine. It contains special proteins that protect your baby from infections in the first weeks of life — no formula can give your baby this protection.' This reframing technique from health communication research is consistently more effective at changing behaviour than factual counter-arguments.