Page 13 of 27
CM10.5 | CM10.5 | Immunization and Childhood Illness Programmes — SDL Guide (Part 2)
Cold Chain and Vaccine Logistics
The cold chain is the unbroken series of refrigerated storage and transport links that maintains vaccines at safe temperatures from manufacture to administration. A failure at any link renders the entire downstream vaccine supply potentially ineffective — and unlike a clinical drug that might simply lose potency, a degraded vaccine offers no protection while still being administered, creating false coverage records. The cold chain hierarchy in India operates from: State Vaccine Store (large walk-in cold rooms, 2-8°C; separate deep-freeze for OPV and BCG at -15 to -25°C) → District Cold Chain Point (ice-lined refrigerators and deep freezers) → CHC/PHC (ice-lined refrigerators, ILRs, at 2-8°C) → Sub-centre (vaccine carrier with ice packs for outreach sessions, maintaining 2-8°C for 4-6 hours) → Immunization session (insulated vaccine carrier, 2-8°C). OPV requires -15 to -25°C at state and district levels but can be stored at 2-8°C at peripheral levels for up to 1 month. The Vaccine Vial Monitor (VVM) is a heat-sensitive chemical indicator affixed to each vial: the inner square is lighter than the outer ring when the vaccine is safe to use; the vaccine must be discarded when the inner square colour matches or is darker than the outer ring. For vaccines sensitive to freezing (DTP, Hepatitis B, Pentavalent, TT), the shake test is the standard field method for detecting freeze damage: shake a suspect vial alongside an intentionally frozen control vial of the same type — if both form similar flocculate patterns after settling, the test vial is frozen-damaged and must be discarded. Every vaccine session begins with a cold chain equipment check: VVM verification on each vial, ice pack status in the carrier, and temperature log review.
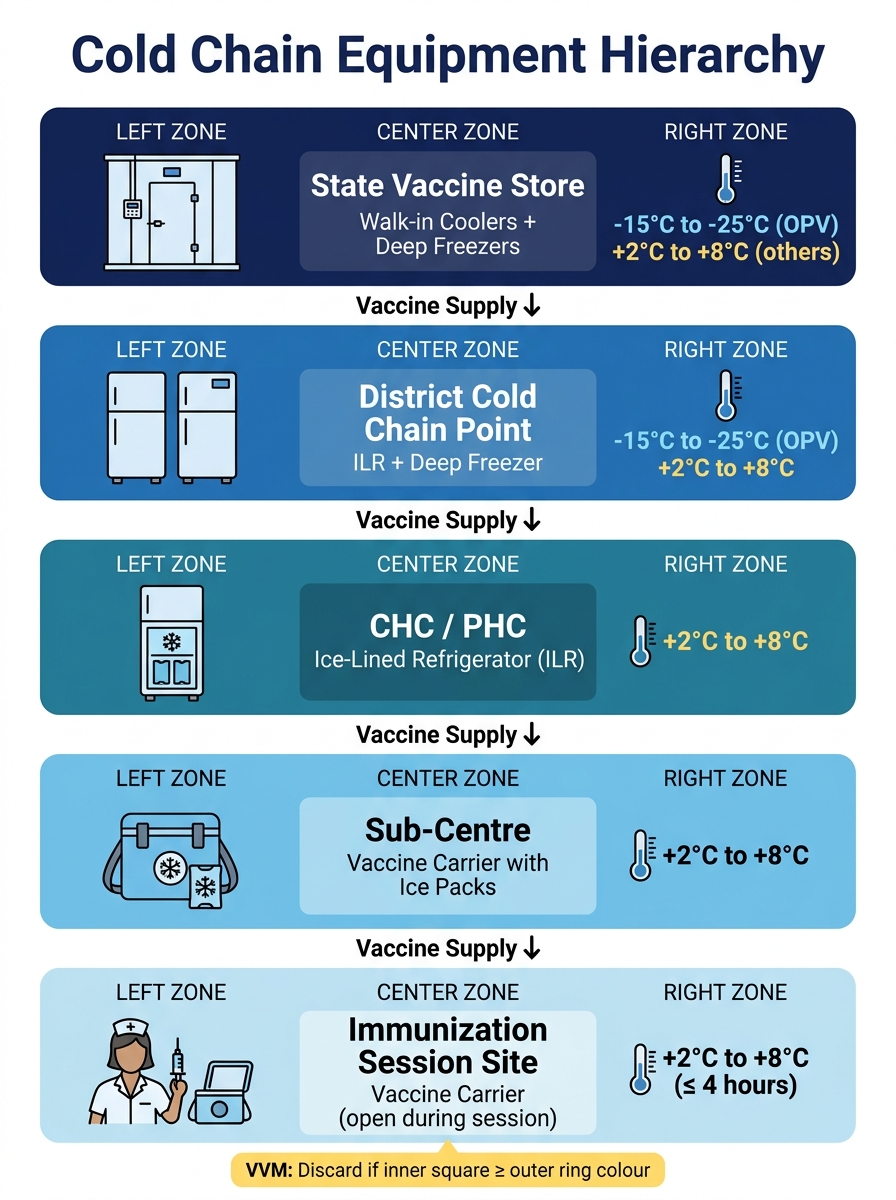
Cold Chain Equipment Hierarchy: State Store to Immunization Session
SELF-CHECK
An ANM opens a vial of Pentavalent vaccine at an outreach session and notices the VVM inner square is slightly darker than the outer circle ring. What should she do?
A. Use the vial — minor colour change is acceptable within WHO guidelines
B. Perform the shake test to confirm and then discard if confirmed freeze-damaged
C. Discard the vial immediately — VVM darkening indicates heat exposure and the vaccine is unusable
D. Keep the vial for BCG reconstitution since BCG is not heat-sensitive
Reveal Answer
Answer: C. Discard the vial immediately — VVM darkening indicates heat exposure and the vaccine is unusable
When the VVM inner square is darker than the outer ring, the vaccine has been exposed to cumulative heat beyond safe limits and MUST be discarded immediately, regardless of the shake test. This is the final discard point. Note: the shake test is used for freeze-sensitive vaccines (Pentavalent, DTP, Hepatitis B) to detect FREEZE damage (not heat damage), which requires a different detection method. If the VVM is at or past the discard point, no shake test is needed — the vial is already condemned by the VVM alone. Using such a vial risks giving an ineffective dose, creating false immunisation records.
IMNCI: Integrated Management of Neonatal and Childhood Illness
The Integrated Management of Neonatal and Childhood Illness (IMNCI) is a WHO/GOI case-management protocol that consolidates the assessment and treatment of the five major childhood killers into a single, structured clinical encounter — replacing the fragmented vertical approach where diarrhoea, pneumonia, and malaria were each managed by separate specialists or separate protocols. IMNCI applies to children from birth to 5 years (IMNCI extends to neonates 0-2 months; the original IMCI covered only 2 months to 5 years). The protocol proceeds through three sequential steps for every child who presents to a health worker. Step 1 — ASSESS: the health worker checks for general danger signs first (not able to drink/breastfeed, vomiting everything, convulsions, lethargic or unconscious) — any danger sign mandates immediate referral. Then each of the five illness domains is assessed systematically: diarrhoea (duration, blood in stool, dehydration signs), respiratory infection (fast breathing — RR ≥60/min in <2 months; ≥50/min in 2-12 months; ≥40/min in 1-5 years — and chest in-drawing or stridor), fever (duration, malaria zone, neck stiffness, measles signs), malnutrition (weight-for-age, MUAC, oedema), and ear infection. Step 2 — CLASSIFY: based on assessment findings, each illness domain is classified as severe (needs urgent referral), moderate (needs treatment at facility), or mild (home management). Classification uses colour-coded categories: pink = urgent referral, yellow = treatment + follow-up, green = home care counselling. Step 3 — TREAT: for each classification, the protocol specifies the exact treatment (e.g., pneumonia — moderate — receives oral amoxicillin 25 mg/kg twice daily for 5 days; referral-level pneumonia with severe chest in-drawing gets IM benzylpenicillin before referral). Home management guidance is given for all categories, including ORS for diarrhoea, home-mixed feeding advice, and when to return immediately.
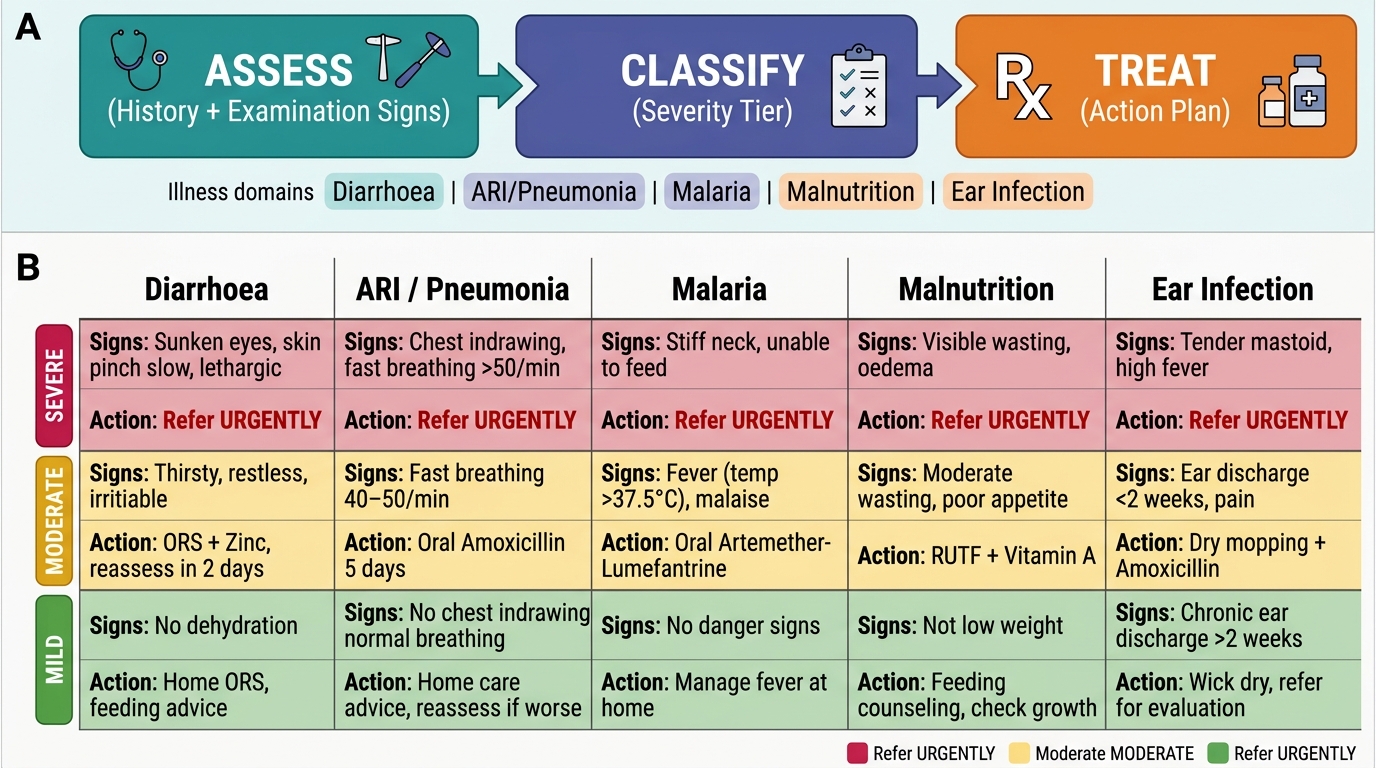
IMNCI Assess-Classify-Treat Framework: Five Illness Domains and Severity-Based Action Tiers
Monitoring UIP Coverage and Programme Evaluation
UIP monitoring uses two complementary measurement approaches: administrative coverage (reported through the programme system) and survey-based coverage (from independent surveys like NFHS). Administrative coverage is calculated monthly at each facility level: (number of doses administered / target population for that antigen) × 100. The target population for child immunization is the estimated number of live births (approximately 2.5% of total population × 12/12 for annual births). Administrative data are collected through HMIS and the RCH portal (MCTS). NFHS-5 provides the survey-based coverage: fully immunized children (12-23 months receiving BCG + 3 doses of OPV + 3 doses of DPT + MR) = 76.4% in India (NFHS-5 2019-21). The gap between administrative coverage (often reported as 85-90%) and survey-based coverage (76.4%) is the administrative-survey discrepancy — it reflects data quality issues, denominator errors, or actual coverage gaps. The dropout rate (DPT1 to DTP3) should be below 10% at the PHC level. Mission Indradhanush (launched 2014) is a targeted catch-up immunization campaign for children who have missed routine UIP doses — it focuses on high-risk districts with <90% coverage, hard-to-reach populations (migrants, slum-dwellers, tribal communities), and zero-dose children (who have received no vaccine at all). Intensified Mission Indradhanush (IMI) campaigns conduct 4-7 rounds of intensified outreach in identified blocks, using fixed and outreach immunization sessions with extended timing. Coverage evaluation at PHC level uses the 30-cluster survey method (30 clusters of 7 children per cluster, 210 children total) to estimate facility-level coverage independent of administrative reporting.
CLINICAL PEARL
The most common cold chain error at outreach sessions is leaving the vaccine carrier open between administrations while managing the queue — ambient temperature equilibration degrades vaccines faster than any other field failure. Train session staff to: open the carrier only to remove one vial at a time; keep ice packs frozen (do not use partially melted packs); and return unused open vials to the carrier between children. The 'open multi-dose vial policy' allows BCG, OPV, and MR/Measles multi-dose vials to be reused at subsequent sessions within 28 days IF they meet three criteria: the VVM has not reached the discard point, the expiry date has not passed, and aseptic technique was maintained. DTP, Pentavalent, and TT single-dose or multi-dose vials opened at a session should not be reused.