Page 17 of 27
CM10.6-7 | CM10.6-7 | Family Planning and Family Welfare Programme — SDL Guide (Part 2)
Permanent Methods and Post-Partum Family Planning
Permanent contraceptive methods are appropriate for couples who have completed their desired family size and are certain they do not want future pregnancies — informed consent requires explicit counselling that reversal is possible only in 40-70% of cases (vasectomy reversal) and carries significant cost and uncertainty. Female sterilization is the most widely used contraceptive method in India (37.9% mCPR, NFHS-5). The two common approaches are: laparoscopic tubectomy (interval or post-abortion), performed under general anaesthesia through a small subumbilical incision, using Falope rings, Filshie clips, or electrocoagulation to occlude the fallopian tubes; and minilaparotomy (postpartum, when the uterus is still enlarged and the tubes are easily accessible), performed under local anaesthesia through a 2-3 cm suprapubic incision — the modified Pomeroy technique (loop ligation and excision) is the standard. Both achieve 99.5%+ effectiveness. Complications include anaesthetic risk, bowel or vessel injury during laparoscopy (rare, <0.5%), and the risk of ectopic pregnancy if sterilization fails (because the remaining tubal stumps may facilitate fertilisation without allowing normal tubal transport). Male sterilization (vasectomy): grossly underutilised in India (0.3% mCPR, NFHS-5), though it is safer, faster, and cheaper than female sterilization. No-Scalpel Vasectomy (NSV) uses a puncture technique rather than a skin incision, reducing haematoma and infection risk; the procedure takes 10-15 minutes under local anaesthesia and requires a 48-hour rest period. Effectiveness is 99.9%; men are not sterile immediately — 15-20 ejaculations or 3 months of alternate contraception are required to clear the vas of residual sperm. NSV was promoted by the GOI as the preferred male sterilization technique from 2001. PPIUCD: inserting a Cu-T 380A IUCD within 48 hours of delivery (the postpartum IUCD) capitalises on the high motivation of the delivery contact and the accessible os; beyond 48 hours the uterus begins to involute, making insertion more difficult and increasing expulsion risk. At 6 weeks postpartum (interval IUCD), the uterus has fully involuted and Cu-T 380A insertion follows the standard technique. Post-abortion contraception: IUCD, COC, or DMPA should be offered immediately after management of incomplete abortion or medical termination, as ovulation can resume as early as 2 weeks after first-trimester abortion.
SELF-CHECK
A 32-year-old woman had an emergency caesarean section 30 hours ago, is breastfeeding her newborn, and now wants reliable long-term contraception. Which of the following is the MOST appropriate option at this moment?
A. Combined oral contraceptive pill, started today
B. DMPA (Depo-Provera injectable) 150 mg IM, given today
C. PPIUCD (Cu-T 380A) inserted now, within the 48-hour window
D. Counsel and defer — no contraceptive option is safe before 6 weeks postpartum
Reveal Answer
Answer: C. PPIUCD (Cu-T 380A) inserted now, within the 48-hour window
PPIUCD must be inserted within 48 hours of delivery; at 30 hours she is still within the window. After a caesarean section, PPIUCD can be inserted under direct vision at the time of CS or manually via the uterine incision before closure — the postpartum uterus is well-defined and the fundus accessible. If not inserted at CS, manual insertion vaginally within 48 hours is still possible. COC (Option A) is WHO MEC category 3 during exclusive breastfeeding in the first 6 months (estrogen suppresses lactation). DMPA (Option B) is WHO MEC 2 postpartum — safe while breastfeeding — but less than ideal at 30 hours postpartum because of bleeding risk; DMPA is generally deferred 6 weeks postpartum unless PPIUCD is not accepted. Option D is incorrect — PPIUCD and DMPA are both safe postpartum contraceptive options.
Family Welfare Programme: Organisation and Operational Aspects
The Family Welfare Programme is India's longest-standing vertical health programme (launched as the Family Planning Programme in 1952, the world's first national family planning programme) and has undergone four major phases of evolution. The current cafeteria approach (adopted 1996 after abandoning the target-based system) offers clients a full basket of choices — all methods are available, all are presented without directive pressure, and the client selects based on informed consent after counselling. The institutional structure flows from: Central Ministry of Health and Family Welfare (MOHFW) → State Department of Health/Family Welfare → District Health Society (DHS) and District Chief Medical Officer → Block PHC Medical Officer → Sub-centre ANM → ASHA at the village level. At the PHC level, the Medical Officer is responsible for: family planning counselling OPD; IUD insertion services; laparoscopic or minilaparotomy sterilization services (at CHC/district hospital); Antara injectable programme (ASHA delivers DMPA from sub-centre); and HMIS reporting of monthly acceptors and cumulative method-mix. The Antara programme (DMPA injectable, launched nationally 2017-18) operationalises injectables as a sub-centre-level service: the ASHA escorts the client to the ANM at the sub-centre, who administers the injection and schedules the next visit in 12-13 weeks; the ASHA follows up to ensure repeat injection adherence. Mission Parivar Vikas: a targeted programme for 146 high-fertility districts across 7 states (UP, Bihar, Rajasthan, MP, Chhattisgarh, Jharkhand, Assam) where TFR remains >3; it intensifies supply of contraceptives through mobile medical units, contraceptive vending machines at rural locations, and targeted ASHA incentives. The compensation scheme for sterilization acceptors provides a cash payment to compensate for the income loss and medical expenses associated with the procedure — this is an enablement rather than an incentive, a distinction the GOI has emphasised since the coercive era.
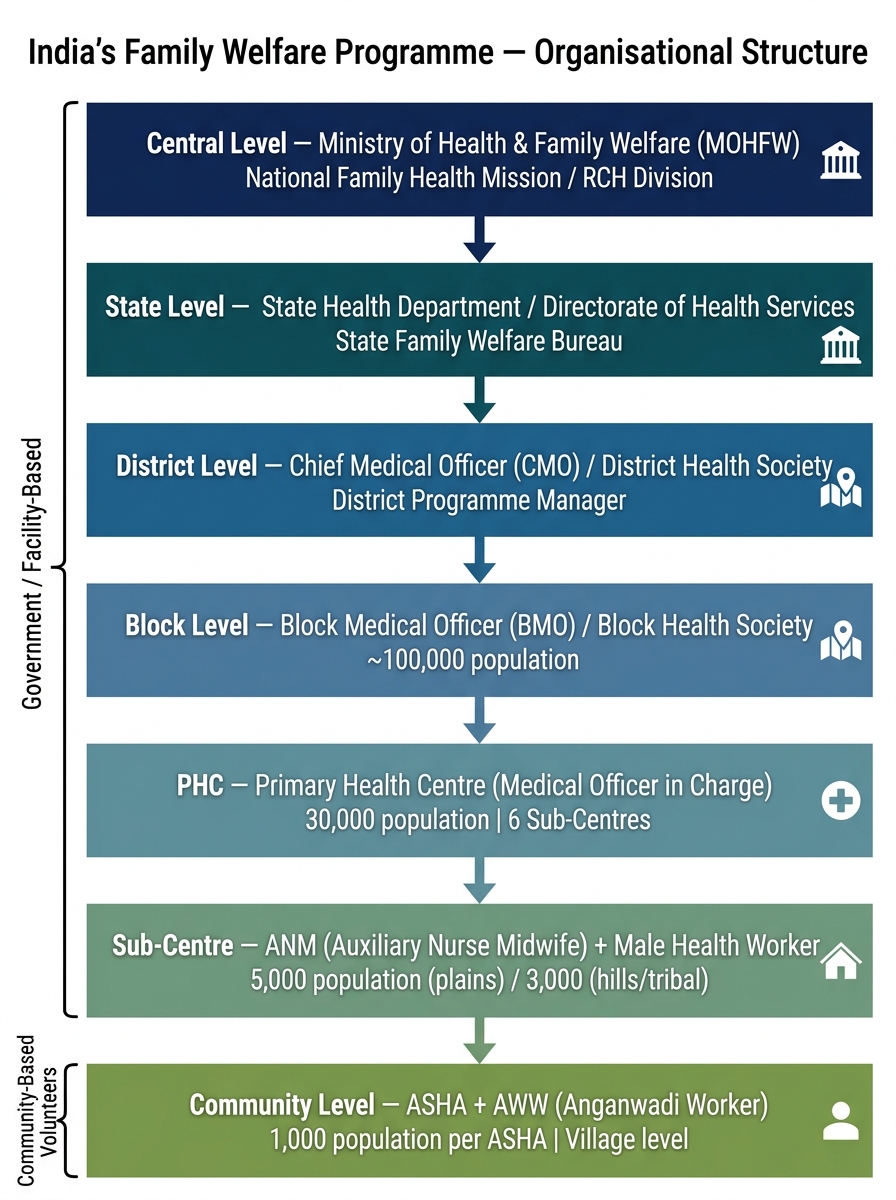
Organisational Structure of India's Family Welfare Programme (Central to Community Level)
Evaluating the Family Welfare Programme
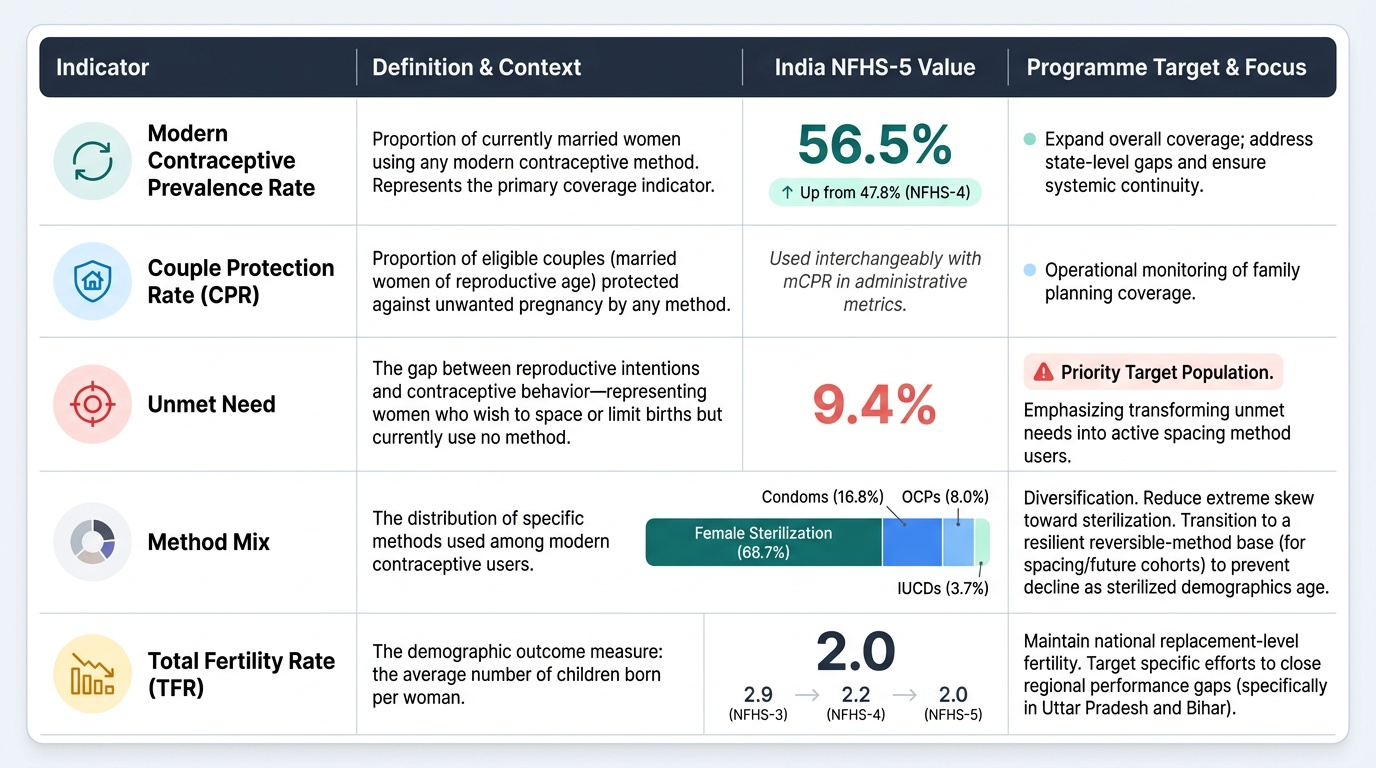
Programme evaluation uses a layered set of indicators that track both method-specific uptake and population-level fertility outcomes. The modern Contraceptive Prevalence Rate (mCPR) — the proportion of currently married women using any modern contraceptive method — is the primary coverage indicator; India's NFHS-5 mCPR is 56.5%, representing substantial progress from 47.8% in NFHS-4 (2015-16). The Couple Protection Rate (CPR) — sometimes used interchangeably with mCPR in Indian programme documents — represents the proportion of eligible couples (married women of reproductive age) protected against an unwanted pregnancy by any contraceptive method. Unmet need (NFHS-5: 9.4%) quantifies the gap between reproductive intentions and contraceptive behaviour — it is the programme's priority target population because these are women who want to space or limit childbearing but are not currently using any method. Method mix refers to the distribution of methods used among mCPR users: India's method mix is dominated by female sterilization (NFHS-5: 66.7% of all modern contraceptive users), followed by condom (16.8%), OCP (8.0%), and IUCD (3.7%). This skewed method mix is a programme quality concern because sterilization, once done, requires replacement by spacing methods for future cohorts — a system that does not build a robust reversible-method base will face declining effective coverage as the sterilized cohort ages out. TFR trend provides the demographic outcome measure: reduction from 2.9 (NFHS-3, 2005-06) to 2.2 (NFHS-4, 2015-16) to 2.0 (NFHS-5, 2019-21) demonstrates sustained programme progress, though national achievement masks the UP/Bihar gap.
Provided image
CLINICAL PEARL
The PPIUCD insertion window of 48 hours postpartum is the most clinically important time constraint in family planning — missing it is irreversible until the 6-week interval visit. The highest-motivation contraceptive counselling contact in a woman's reproductive life is DURING labour — before delivery, while she is still in the facility. Train ANMs to conduct brief family planning counselling during latent labour (not active labour), obtain consent for PPIUCD insertion if she is interested, and insert at the time of delivery of the placenta (if spontaneous vaginal delivery) or manually via the uterine incision (if caesarean section). This strategy — called the 'Immediate Postpartum Family Planning' approach — has dramatically increased PPIUCD uptake in facilities that implement it systematically.